I have all the data I need. Now let me write the complete, comprehensive learning note:
COMPLETE LEARNING NOTE
CHOLINERGIC DRUGS AND ANTICHOLINERGIC DRUGS
From Absolute Beginner to MBBS Examination Mastery
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics; Lippincott Illustrated Reviews: Pharmacology; Guyton & Hall Textbook of Medical Physiology; Katzung's Basic and Clinical Pharmacology
SECTION 1: BIG PICTURE OVERVIEW
What problem do cholinergic and anticholinergic drugs solve?
Before we touch a single drug name, let us build the scene in your mind.
Your body has two main control systems running constantly behind the scenes:
- The sympathetic nervous system - the "fight or flight" system. Imagine you see a lion. Your heart races, your pupils dilate, your mouth dries up, your muscles tense. Your body is ready to run or fight.
- The parasympathetic nervous system - the "rest and digest" system. After dinner, relaxing at home: your heart slows, saliva flows, your gut moves food along, your bladder contracts to empty urine.
These two systems are always in balance, like two people on a seesaw. When one side goes up, the other goes down.
The parasympathetic nervous system uses acetylcholine (ACh) as its messenger. ACh is the chemical it releases to tell organs what to do.
Now, here is the big picture:
- Cholinergic drugs = drugs that MIMIC or ENHANCE the action of acetylcholine. They push the parasympathetic side of the seesaw down.
- Anticholinergic drugs = drugs that BLOCK the action of acetylcholine. They push the sympathetic side down (by removing parasympathetic influence).
Why do we need these drugs?
| Problem | Drug Solution |
|---|
| Urinary retention (bladder won't contract) | Cholinergic drug - makes bladder contract |
| Glaucoma (eye pressure too high) | Cholinergic drug - opens drainage channels |
| Myasthenia gravis (muscles too weak) | Anticholinesterase - keeps ACh in synapse longer |
| Bradycardia (heart too slow) | Anticholinergic drug - removes vagal brake on heart |
| Asthma/COPD (airways too narrow) | Anticholinergic drug - relaxes airway muscles |
| Motion sickness (nausea from brain signals) | Anticholinergic drug - blocks nausea signals |
| Organophosphate poisoning (too much ACh) | Anticholinergic drug - blocks excess ACh effects |
SECTION 2: BUILD THE FOUNDATION
Part A: The Nervous System - A Child's Mental Picture
Think of your nervous system as a telephone network connecting your brain to every organ in your body.
The brain sends messages through cables (nerves). At the end of each cable, the message must jump across a tiny gap to reach the organ. This gap is called the synapse (from Greek: "clasp together").
How does the message jump the gap? It uses chemical messengers called neurotransmitters (neuro = nerve; transmitter = sender). They are like tiny ferryboats carrying a message across the gap.
Acetylcholine (ACh) is the key neurotransmitter of the parasympathetic system. It is also used at certain other key locations, which we will map out shortly.
Part B: The Autonomic Nervous System in Full Detail
"Autonomic" means self-controlling - these nerves control functions you do not consciously think about: your heartbeat, digestion, breathing, urination.
The autonomic nervous system has two main divisions:
AUTONOMIC NERVOUS SYSTEM
│
├── PARASYMPATHETIC (rest and digest)
│ Uses ACh everywhere (pre AND post ganglionic)
│ Receptors: Muscarinic (on effector organs)
│ Nicotinic (at ganglia)
│
└── SYMPATHETIC (fight or flight)
Pre-ganglionic: uses ACh (Nicotinic receptors)
Post-ganglionic: uses Norepinephrine (Adrenergic receptors)
Exception: Sweat glands = ACh (Muscarinic)
Adrenal medulla = ACh (Nicotinic)
Key insight that many students miss: ACh is used at ALL autonomic ganglia (both sympathetic and parasympathetic). ACh is only used at parasympathetic post-ganglionic junctions. This is why understanding receptor types is so important.
Part C: Where Exactly Does ACh Work? - The Cholinergic Junctions
There are five main places where ACh acts:
1. PARASYMPATHETIC POSTGANGLIONIC JUNCTIONS
→ Nerve → Organ (heart, gut, eye, bladder, glands)
→ Receptor type: MUSCARINIC
→ ACh effects: slow heart, increase gut motility, contract bladder, etc.
2. ALL AUTONOMIC GANGLIA
→ Preganglionic nerve → Postganglionic nerve
→ Both sympathetic and parasympathetic
→ Receptor type: NICOTINIC (Nn subtype - "N for neurons")
3. NEUROMUSCULAR JUNCTION (Skeletal muscle)
→ Motor nerve → Skeletal muscle
→ Receptor type: NICOTINIC (Nm subtype - "N for muscle")
→ ACh effects: muscle contraction
4. CNS (Brain and Spinal Cord)
→ Brain neurons use ACh for memory, cognition, movement control
→ Both muscarinic and nicotinic receptors
5. ADRENAL MEDULLA
→ Preganglionic fibers → Adrenal cells
→ Receptor type: NICOTINIC
→ Result: Adrenaline (epinephrine) release into blood
Part D: Synthesis, Storage, and Release of Acetylcholine
This is the mechanism map. Every drug that enhances or blocks ACh acts at one of these six steps.
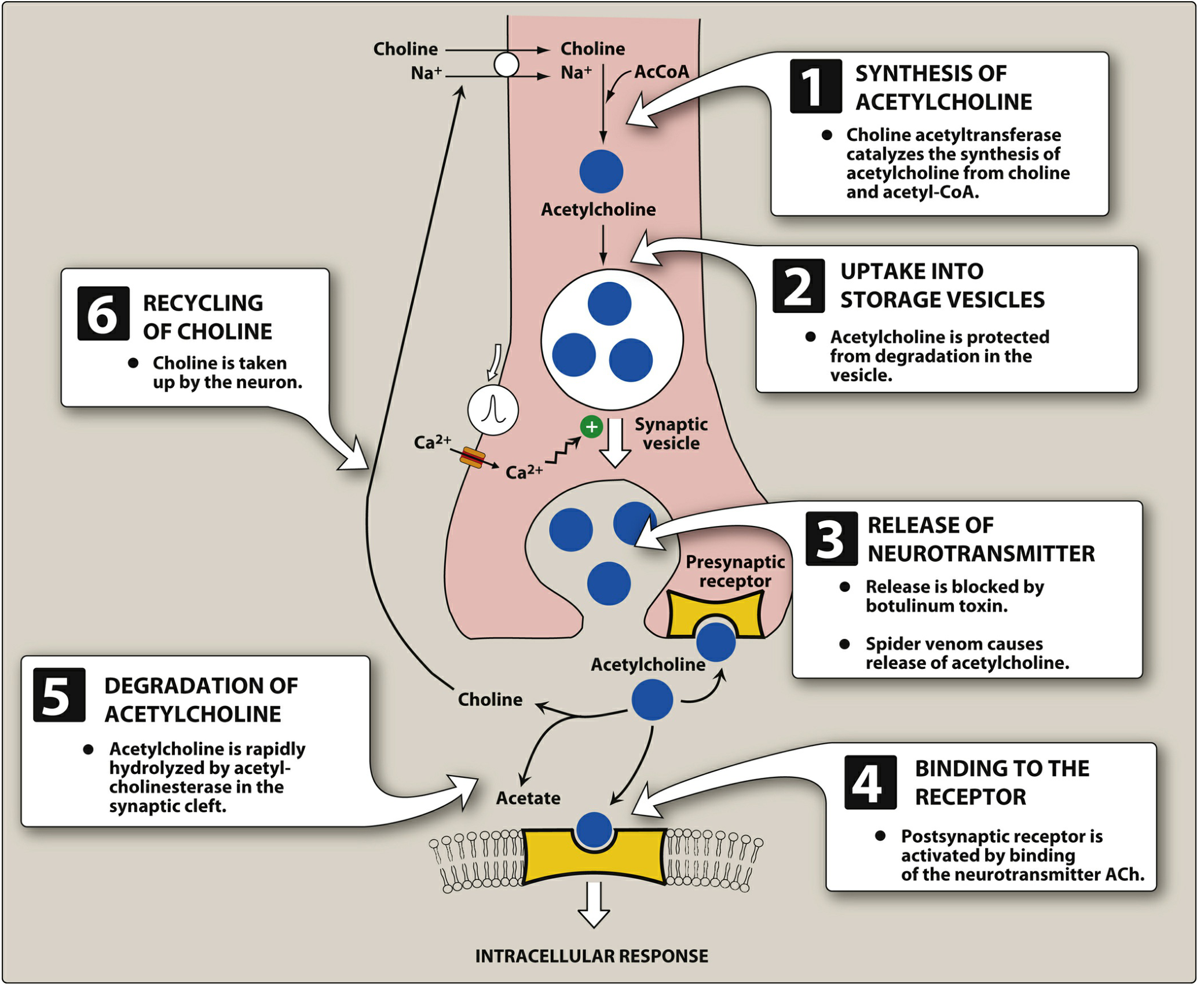
Figure: Synthesis and Release of ACh - Lippincott Pharmacology
Step 1 - Synthesis of ACh:
- Choline is transported FROM extracellular fluid INTO the nerve terminal by a sodium-coupled carrier (active transport, energy-dependent)
- This uptake of choline is the rate-limiting step in ACh synthesis
- Inside the terminal, the enzyme Choline Acetyltransferase (ChAT) combines choline + Acetyl-CoA → Acetylcholine
- Drug point: Hemicholinium blocks choline uptake → depletes ACh synthesis
Step 2 - Storage in vesicles:
- ACh is packaged into synaptic vesicles by active transport (VAChT - vesicular ACh transporter)
- Protected from degradation inside the vesicle
- ATP is stored alongside ACh as a co-transmitter
- Drug point: Vesamicol blocks vesicular uptake of ACh
Step 3 - Release:
- Action potential arrives → voltage-gated Ca²+ channels open → Ca²+ flows in
- Elevated intracellular Ca²+ causes vesicle fusion with membrane → exocytosis of ACh into synapse
- Drug point: Botulinum toxin BLOCKS vesicle fusion → no ACh released → paralysis
- Drug point: Black widow spider venom causes MASSIVE ACh release
Step 4 - Receptor Binding:
- ACh diffuses across synapse and binds to:
- Postsynaptic receptors (muscarinic or nicotinic) → produces effect
- Presynaptic receptors (autoreceptors) → negative feedback, reduces further ACh release
Step 5 - Degradation by Acetylcholinesterase (AChE):
- Acetylcholinesterase (AChE) is an enzyme in the synapse that rapidly breaks ACh into choline + acetate
- This terminates the ACh signal almost instantly
- This is the fastest enzymatic reaction known in biology - one AChE molecule can destroy 25,000 ACh molecules per second
- Drug point: Anticholinesterase drugs (neostigmine, physostigmine, organophosphates) block AChE → ACh accumulates → prolonged and intensified effect
Step 6 - Recycling of Choline:
- Choline is taken back up into the neuron by the high-affinity choline transporter
- Used again to make more ACh
Part E: Muscarinic vs. Nicotinic Receptors
This is probably the single most important distinction in this entire topic. Learn it cold.
The naming story:
- Muscarine is a poison from the mushroom Amanita muscaria (the red toadstool with white dots). It activates only muscarinic receptors.
- Nicotine is from tobacco. It activates only nicotinic receptors.
- Acetylcholine activates BOTH types, because it is the natural neurotransmitter.
Muscarinic Receptors
Muscarinic receptors are G-protein-coupled receptors (GPCRs). Think of them as a locked door that needs a special key (ACh). When the key fits, it does not directly open a channel - instead it activates an interior protein (G-protein) that then triggers a second messenger cascade inside the cell.
There are 5 subtypes: M1 through M5.
| Subtype | Location | G-protein | Effect |
|---|
| M1 | Gastric glands, CNS neurons (cortex, hippocampus) | Gq → IP3 → ↑Ca²+ | Increased gastric acid secretion; CNS cognition |
| M2 | Heart (SA node, AV node) | Gi → ↓cAMP | Decreased heart rate, decreased AV conduction |
| M3 | Smooth muscle (GI, bronchi, bladder), exocrine glands, eye | Gq → IP3 → ↑Ca²+ | Smooth muscle contraction, gland secretion |
| M4 | CNS, striatum | Gi | Modulation of dopamine, movement |
| M5 | CNS (substantia nigra) | Gq | Dopamine modulation |
Clinically, M1, M2, M3 are the most important.
Memory aid for M2 in heart: M2 says "slow down" to the heart (M2 = Myocardial inhibition → bradycardia).
Memory aid for M3: M3 = More secretion + More smooth muscle contraction.
Nicotinic Receptors
Nicotinic receptors are ligand-gated ion channels. Think of them as a direct door - when ACh binds, the door (ion channel) immediately opens and sodium and calcium rush in, directly causing depolarization. No intermediate G-protein. Much faster than muscarinic signaling.
There are two clinically important subtypes:
| Subtype | Location | Effect |
|---|
| Nn (Neuronal) | All autonomic ganglia (sympathetic + parasympathetic), CNS | Ganglionic transmission; CNS excitation |
| Nm (Muscle) | Neuromuscular junction | Skeletal muscle contraction |
Structural difference: Nicotinic receptors at ganglia (Nn) and muscle (Nm) have different subunit compositions, which is why some drugs can selectively block muscle nicotinic (e.g., curare) vs. ganglionic nicotinic.
Part F: Effects of Parasympathetic Stimulation (= Muscarinic Effects)
Learning the organ-by-organ effects of ACh on muscarinic receptors is essential. Use the mnemonic SLUDGE/DUMBELS (covered in Section 6) but first understand the physiology:
ORGAN ACh EFFECT (MUSCARINIC) CLINICAL RELEVANCE
─────────────────────────────────────────────────────────────────────
Heart ↓ HR (SA node), ↓ Conduction Bradycardia, AV block
(AV node), ↓ contractility
Eyes Pupil CONSTRICTION (miosis) Glaucoma treatment
Ciliary muscle CONTRACTION Near vision (accommodation)
(lens becomes rounder for near)
Lungs Bronchoconstriction Asthma trigger
↑ Bronchial secretions Mucus production
GI Tract ↑ Motility + secretions Diarrhea, cramps, nausea
Relax sphincters Facilitates defecation
Salivary Glands ↑ Salivation (watery saliva) SLUD - Salivation
Lacrimal Glands ↑ Tearing (lacrimation) SLUD - Lacrimation
Sweat Glands ↑ Sweating Diaphoresis (note: sympathetic
innervation but muscarinic receptor)
Bladder Detrusor CONTRACTS Urination
Internal sphincter RELAXES Facilitates voiding
Male Genital Erection (Parasympathetic) "Point and Shoot" mnemonic
Blood Vessels Vasodilation (endothelium Decreases blood pressure
releases NO via M3)
Secretions ↑ Exocrine secretions: Excessive secretions in
tears, saliva, sweat, gastric organophosphate poisoning
acid, bronchial secretions
SECTION 3: DRUG CLASS FRAMEWORK
CLASS 1: CHOLINERGIC AGONISTS (Parasympathomimetics)
These drugs mimic or enhance the action of acetylcholine.
Sub-class 1A: Direct-Acting Cholinergic Agonists (Muscarinic Agonists)
These drugs directly activate muscarinic receptors, bypassing the nerve and the ACh synthesis/release machinery. They act just like ACh would - but they are more resistant to breakdown by AChE.
Why more resistant? ACh is broken down almost instantly by AChE. If you give ACh as a drug, it is destroyed before it does anything clinically useful. So we use synthetic analogues that are structurally similar but resistant to degradation.
Key Drugs:
| Drug | Key Features | Main Clinical Use | Special Note |
|---|
| Acetylcholine | Natural transmitter; destroyed instantly by AChE | Only used topically in eye (intraocular) during surgery | Too short-acting for systemic use |
| Methacholine | Muscarinic selective; resistant to AChE; given by inhalation | Bronchial provocation test to diagnose asthma | Diagnostic only - causes bronchoconstriction in asthmatics |
| Carbachol | Acts on both muscarinic AND nicotinic; resistant to AChE and BuChE | Glaucoma (topical eye drops); intraocular surgery | Long duration of action |
| Bethanechol | Muscarinic selective, no nicotinic; resistant to AChE; acts mainly on GI and bladder | Postoperative ileus, neurogenic bladder (urinary retention) | Does not affect heart significantly; given orally or SC (never IV - could cause severe hypotension) |
| Pilocarpine | Tertiary amine (crosses blood-brain barrier); mixed muscarinic + weak nicotinic | Glaucoma (topical); Xerostomia (Sjogren's syndrome, post-radiation); Sjogren's syndrome | Most widely used cholinergic agonist in ophthalmology |
Mechanism of Action:
ACh-like molecule → binds muscarinic receptor (M1, M2, M3) → activates G-protein → intracellular signaling cascade → organ effects as listed in the table above
Spectrum of Effects:
All muscarinic effects - SLUDGE (see Section 6)
Adverse Effects:
All adverse effects are extensions of muscarinic stimulation:
- GI: Nausea, vomiting, diarrhea, abdominal cramps (↑ gut motility)
- CV: Bradycardia, hypotension, flushing (vasodilation via NO)
- Respiratory: Bronchoconstriction, ↑ bronchial secretions (dangerous in asthma)
- Eyes: Miosis, blurred vision (spasm of accommodation)
- Exocrine glands: Sweating, salivation, lacrimation
Contraindications:
- Asthma / COPD (bronchoconstriction is dangerous)
- Mechanical bowel obstruction (↑ motility against fixed obstruction = perforation risk)
- Mechanical urinary obstruction (↑ bladder contraction against fixed block)
- Peptic ulcer disease (↑ gastric acid)
- Bradycardia / Heart block
- Hypotension
High-Yield Clinical Scenarios:
- Bethanechol: post-operative urinary retention / ileus = exam favorite
- Pilocarpine eye drops: primary open-angle glaucoma
- Methacholine challenge test: diagnosing bronchial hyperreactivity in asthma
Sub-class 1B: Indirect-Acting Cholinergic Agonists (Anticholinesterases)
These drugs do NOT directly activate receptors. Instead, they inhibit acetylcholinesterase (AChE) - the enzyme that destroys ACh in the synapse.
Analogy: Imagine ACh is a worker doing a job. AChE is a supervisor who fires the worker the moment the job is done. Anticholinesterases are drugs that "fire the supervisor" - so the worker (ACh) keeps working longer and harder.
The result: ACh accumulates in ALL synapses where it is released - muscarinic, nicotinic ganglionic, AND neuromuscular junctions.
Important Sub-classification by Type of Inhibition:
1. Reversible Inhibitors (Short to medium duration)
| Drug | Type | Duration | Main Use |
|---|
| Edrophonium | Reversible, electrostatic bond | Ultra-short (5-10 min) | Tensilon test - diagnosis of myasthenia gravis |
| Neostigmine | Reversible carbamylate | Short (1-2 h) | Myasthenia gravis (oral); reversal of NMJ block after surgery; postoperative ileus/urinary retention |
| Pyridostigmine | Reversible carbamylate | Intermediate (3-6 h) | Myasthenia gravis (preferred long-term) |
| Physostigmine | Reversible carbamylate | Short; LIPID SOLUBLE - crosses BBB | Antidote for anticholinergic poisoning (atropine overdose) - can enter brain to reverse CNS effects |
| Donepezil, Rivastigmine, Galantamine | Reversible | Long-acting | Alzheimer's disease - improves memory by increasing ACh in brain (brain has lost cholinergic neurons) |
| Tacrine | Reversible | - | Alzheimer's (older; hepatotoxic, rarely used now) |
2. Irreversible Inhibitors (Organophosphates)
These form a covalent bond with the serine residue in the active site of AChE. The bond is so strong that recovery requires synthesis of new AChE enzyme (days to weeks), unless an antidote is given quickly.
| Drug | Source | Use |
|---|
| Echothiophate | Pharmaceutical | Glaucoma (eye drops) |
| Parathion, Malathion | Insecticide | Agricultural pest control; source of poisoning |
| Sarin, VX, Soman, Tabun | Chemical warfare agents | Weapons of mass destruction |
Aging: When an organophosphate-AChE complex exists for too long, it undergoes a process called "aging" - the bond becomes even more permanent and cannot be reversed by antidotes. This is why antidote treatment must be given EARLY.
Mechanism in Full:
Normal: ACh released → binds receptor → AChE destroys ACh → effect stops
With Anticholinesterase:
ACh released → binds receptor → AChE is BLOCKED
↓
ACh stays in synapse
↓
Prolonged, intensified effect
↓
BOTH muscarinic AND nicotinic receptors activated
Clinical Effects of Anticholinesterases:
Muscarinic effects (peripheral, glands, smooth muscle, heart):
- SLUDGE: Salivation, Lacrimation, Urination, Defecation, GI distress, Emesis
Nicotinic effects at NMJ:
- Fasciculations (involuntary muscle twitches) → then muscle weakness → paralysis (due to depolarization blockade - muscles depolarize and cannot repolarize)
CNS effects (only drugs that cross BBB):
- Anxiety, restlessness, seizures, coma (from excess ACh in brain)
Organophosphate Poisoning - A Full Clinical Picture
This is the most important clinical scenario for anticholinesterases.
Cause: Farmer sprays pesticide; soldier exposed to nerve agent; or deliberate poisoning.
Pathophysiology:
Organophosphate inhibits AChE → massive ACh accumulation everywhere → simultaneous activation of all muscarinic and nicotinic receptors
Clinical features:
MUSCARINIC (Periphery + Brain): NICOTINIC (NMJ + Ganglia):
- Pinpoint pupils (miosis) - Muscle fasciculations
- Excessive sweating - Muscle weakness
- Excessive salivation - Paralysis (respiratory muscles!)
- Lacrimation (tears) - Tachycardia (ganglionic Nn)
- Bronchospasm + ↑ secretions
- Bradycardia CNS:
- Vomiting, diarrhea - Anxiety, restlessness
- Urinary incontinence - Seizures
- Coma
CAUSE OF DEATH: Respiratory failure
(bronchospasm + secretions + paralysis of respiratory muscles)
Treatment of organophosphate poisoning:
Step 1 - Atropine (muscarinic blocker):
- Blocks muscarinic effects immediately
- Dose titrated to dry secretions (not to heart rate!)
- Very large doses may be needed (10-100 mg in severe cases!)
- Reverses: bradycardia, bronchospasm, secretions, GI symptoms
- Does NOT reverse muscle weakness (nicotinic effect)
Step 2 - Pralidoxime (PAM - 2-PAM):
- An oxime that regenerates ("reactivates") AChE by breaking the phosphate bond
- MUST be given EARLY (before "aging" occurs)
- Reverses BOTH muscarinic AND nicotinic effects
- Specifically helps with muscle weakness that atropine cannot address
- Crosses BBB poorly, so limited CNS benefit
Step 3 - Benzodiazepines:
- For seizures (diazepam IV)
Step 4 - Supportive:
- Mechanical ventilation (respiratory paralysis)
- Airway suction (secretions)
Sub-class 1C: Nicotinic Agonists (Ganglionic Stimulants)
These act specifically at nicotinic receptors.
| Drug | Use |
|---|
| Nicotine | Tobacco addiction; nicotine replacement therapy (patches, gum) |
| Succinylcholine | Depolarizing neuromuscular blocker (technically a nicotinic agonist at NMJ that causes persistent depolarization) |
CLASS 2: ANTICHOLINERGIC DRUGS (Cholinergic Antagonists / Parasympatholytics)
These drugs BLOCK muscarinic or nicotinic receptors, preventing ACh from producing its effects.
The term "anticholinergic" in clinical medicine almost always refers to muscarinic antagonists (not nicotinic blockers).
Sub-class 2A: Muscarinic Receptor Antagonists (Antimuscarinics)
The Belladonna Alkaloids
"Belladonna" means "beautiful woman" in Italian. Why? In the Renaissance, women would put drops of belladonna plant extract in their eyes to dilate their pupils - because large pupils were considered beautiful. Now we know this was causing mydriasis by blocking M3 receptors in the iris.
The belladonna plants (Atropa belladonna, Hyoscyamus niger, Datura stramonium / Jimson weed) contain naturally occurring alkaloids.
Key Drugs:
| Drug | Classification | Key Properties | Main Uses |
|---|
| Atropine | Tertiary amine (lipophilic) | Crosses BBB; short duration (~4h); balanced muscarinic blockade | Bradycardia, AV block; organophosphate poisoning; pre-anesthetic; eye drops (mydriasis); antidiarrheal |
| Scopolamine (Hyoscine) | Tertiary amine | Crosses BBB MORE than atropine; more CNS effects | Motion sickness (transdermal patch behind ear); pre-anesthetic (drying + amnesia) |
| Homatropine | Semi-synthetic tertiary | Shorter duration than atropine | Mydriasis/cycloplegia for eye exams |
| Tropicamide | Synthetic | Shortest duration mydriatic (~3-6h) | Eye examination |
| Cyclopentolate | Synthetic | Moderate duration | Eye examination, cycloplegia |
Quaternary ammonium compounds (cannot cross BBB - peripheral effects only):
| Drug | Main Use | Why Quaternary is Preferred Here |
|---|
| Ipratropium | COPD, asthma (inhaled) | No systemic effects; stays in lungs |
| Tiotropium | COPD (inhaled, once daily; M1+M3 selective) | No systemic effects; long duration |
| Aclidinium, Umeclidinium | COPD (inhaled) | Long-acting bronchodilators |
| Glycopyrrolate | Pre-anesthetic drying; excessive salivation | No CNS effects, no amnesia |
| Propantheline | Peptic ulcer (older use); overactive bladder | Reduces gastric secretion and motility |
| Oxybutynin | Overactive bladder (OAB) | M3 blockade → detrusor relaxation |
| Tolterodine | Overactive bladder | M3 selective, fewer dry mouth side effects |
| Solifenacin, Darifenacin | OAB | M3 selective |
| Hyoscine butylbromide (Buscopan) | GI spasm, renal/biliary colic | Smooth muscle relaxation |
Mechanism of Action - Atropine as the Prototype
ACh released from parasympathetic nerve
↓
Normally: ACh → Muscarinic receptor → G-protein → Response
With Atropine:
Atropine occupies receptor → ACh CANNOT bind → NO response
↓
Competitive antagonism (can be overcome by large doses of ACh)
Atropine blocks all five muscarinic subtypes (M1-M5) without selectivity. This is why it has wide-ranging effects AND wide-ranging side effects.
Organ-by-Organ Effects of Atropine/Antimuscarinics:
ORGAN EFFECT OF MUSCARINIC BLOCKADE CLINICAL USE
──────────────────────────────────────────────────────────────────
Heart ↑ Heart rate (tachycardia) Sinus bradycardia, AV block
↑ AV conduction
Eyes PUPIL DILATION (mydriasis) Eye examination
Ciliary muscle relaxes Refraction measurement
→ CYCLOPLEGIA (loss of accommodation) Iridocyclitis treatment
→ Blurred near vision
GI Tract ↓ Motility, ↓ secretions Peptic ulcer (old use)
↑ Sphincter tone (constipation) Antidiarrheal
Dry mouth (↓ saliva) GI spasm
Bronchi Bronchodilation COPD, asthma
↓ Bronchial secretions Thickened mucus in bronchi
Bladder Detrusor RELAXATION Overactive bladder
Internal sphincter CONTRACTS → Urinary retention if excess!
→ Urinary hesitancy/retention
Sweat Glands ↓ Sweating → HYPERTHERMIA Danger in hot weather
(Sympathetic innervation, muscarinic receptors)
Salivary Dry mouth (xerostomia) Problematic side effect
Glands
CNS Restlessness → Sedation Scopolamine for motion sickness
Amnesia (scopolamine) Pre-anesthetic
Confusion/delirium in elderly Danger in geriatrics
A crucial dose-dependent sequence for atropine:
As you increase the dose of atropine, different organs are affected at different doses:
Dose Effect
0.5 mg ↓ Salivation, sweating, bronchial secretions; Slight bradycardia
(Paradoxical bradycardia at very low doses due to presynaptic M1 blockade
on the vagal nerve causing MORE ACh release initially)
1.0 mg Tachycardia; Mild mydriasis; Dry mouth
2.0 mg Tachycardia; Palpitations; More pronounced mydriasis; Blurred vision
5.0 mg All above + Hot dry flushed skin; Urinary retention; Constipation
≥10 mg Excitement → Delirium → Hallucinations → Coma → Death
Adverse Effects of Antimuscarinics (= Atropine Toxicity / Anticholinergic Syndrome):
Mnemonic: "Hot as a hare, dry as a bone, red as a beet, blind as a bat, mad as a hatter, full as a flask"
| Symptom | Cause |
|---|
| Hot as a hare | ↓ Sweating → hyperthermia |
| Dry as a bone | ↓ Salivary, lacrimal, bronchial, skin secretions → dry mouth, dry skin |
| Red as a beet | Cutaneous vasodilation (compensatory) → flushing |
| Blind as a bat | Mydriasis + cycloplegia → blurred vision, photophobia |
| Mad as a hatter | CNS effects → confusion, delirium, hallucinations (especially scopolamine) |
| Full as a flask | Urinary retention (bladder relaxation + sphincter contraction) |
| + Tachycardia | M2 blockade at SA node → fast heart rate |
| + Constipation | ↓ GI motility |
Contraindications:
| Condition | Why Contraindicated |
|---|
| Glaucoma (narrow-angle) | Mydriasis → pupil pushes into trabecular meshwork → aqueous drainage blocked → acute attack → permanent blindness |
| Benign Prostatic Hyperplasia (BPH) | Urinary retention → acute retention in already compromised outflow |
| Myasthenia gravis | Reduces ACh available at NMJ → worsens weakness |
| Tachyarrhythmias | Will increase heart rate further |
| Paralytic ileus | ↓ GI motility worsens ileus |
| Ulcerative colitis | ↓ Motility → toxic megacolon |
Drug Interactions:
| Drug | Interaction |
|---|
| Other anticholinergics (TCAs, antihistamines, antipsychotics) | Additive anticholinergic toxicity |
| Physostigmine | Antidote for anticholinergic poisoning |
| Prokinetics (metoclopramide) | Antagonistic effects on gut motility |
Sub-class 2B: Ganglionic Blockers (Nicotinic Nn Antagonists)
These block nicotinic receptors at autonomic ganglia (both sympathetic AND parasympathetic), blocking transmission in both divisions.
Key drugs: Hexamethonium (historic), Trimethaphan, Mecamylamine (rarely used today)
Effect: Blocks BOTH sympathetic and parasympathetic ganglia simultaneously. The dominant tone in each organ determines which effect predominates:
| Organ | Dominant Tone | Effect of Ganglionic Block |
|---|
| Heart | Parasympathetic (vagal) | Tachycardia |
| Blood vessels | Sympathetic | Vasodilation, hypotension |
| GI tract | Parasympathetic | Constipation, ↓ motility |
| Bladder | Parasympathetic | Urinary retention |
| Eye | Parasympathetic | Mydriasis, cycloplegia |
Clinical Use: Largely obsolete. Trimethaphan was used for hypertensive emergencies and aortic dissection. Now replaced by better drugs.
Sub-class 2C: Neuromuscular Blocking Drugs (Nicotinic Nm Antagonists)
These block nicotinic receptors specifically at the neuromuscular junction. They cause skeletal muscle paralysis. Used in anesthesia/surgery to achieve muscle relaxation.
Two types:
1. Non-depolarizing (Competitive) Blockers:
Block nicotinic receptor → ACh cannot bind → no depolarization → muscle relaxed
| Drug | Duration | Onset |
|---|
| Tubocurarine (d-Tubocurarine) | Long | Slow - prototype; now rarely used |
| Atracurium, Cisatracurium | Intermediate | Intermediate |
| Vecuronium, Rocuronium | Intermediate | Fast (rocuronium fastest) |
| Pancuronium | Long | Slow |
Reversal: Neostigmine + Glycopyrrolate (glycopyrrolate prevents muscarinic side effects of neostigmine)
2. Depolarizing Blockers:
Bind and ACTIVATE nicotinic receptor → persistent depolarization → muscle cannot repolarize → paralysis
| Drug | Duration | Note |
|---|
| Succinylcholine (Suxamethonium) | Ultra-short (5-10 min) | Rapid onset - used for intubation; hydrolyzed by plasma cholinesterase |
Succinylcholine adverse effects:
- Hyperkalemia - depolarization releases K+ from muscle (dangerous in burns, crush injury, denervation injuries)
- Malignant hyperthermia (rare genetic susceptibility - uncontrolled Ca²+ release from muscle → extreme hyperthermia; treat with dantrolene)
- Increased intraocular pressure (contraindicated in open-eye injuries)
- Post-operative myalgia (fasciculations first, then pain)
- Prolonged block in pseudocholinesterase deficiency
SECTION 4: TEACH USING ANALOGIES
Analogy 1: ACh Release - The Mail System
Imagine each cholinergic nerve ending is a post office. The post office (nerve terminal) manufactures letters (ACh), seals them into envelopes (vesicles), and waits for a delivery signal. When the mail truck arrives (action potential), the doors open (Ca²+ enters) and all letters are delivered to mailboxes (receptors) across the street. A mail shredder (AChE) sits right next to the mailboxes and destroys each letter the moment it is read. This ensures the message is brief.
- Hemicholinium = blockade of paper delivery to the post office (no raw material, no letters)
- Botulinum toxin = jams the post office doors shut (no delivery)
- Anticholinesterases = destroy the shredder (letters pile up and keep sending their message)
- Muscarinic agonists = send fake letters directly to the mailboxes (bypass post office)
- Atropine = blocks all the mailboxes with padlocks (letters cannot be read)
Analogy 2: Muscarinic vs. Nicotinic - Two Types of Light Switches
Imagine the cell has two types of light switches:
Muscarinic = Dimmer switch: When you push it, it activates a complex electrical panel (G-protein) that slowly but smoothly adjusts the brightness over a few seconds. You can fine-tune it. Takes longer. More complex.
Nicotinic = Simple on/off toggle switch: When you flip it, electricity immediately flows (ions rush in). Immediate response. Binary - on or off. Fast.
This is why nicotinic effects (like muscle contraction) are fast and nicotinic blocking drugs (curare) cause immediate paralysis, while muscarinic effects (like gut motility changes) are slower and more sustained.
Analogy 3: Atropine at the Eye - The Telescope Lens
Your pupil is normally like a camera aperture. In bright light, the iris muscle (sphincter pupillae) contracts (via M3 receptor) to make the pupil small, protecting the retina. In dark, it relaxes.
Atropine blocks M3 on the iris sphincter → cannot contract → pupil stays wide open (mydriasis), even in bright light.
It also blocks the ciliary muscle → lens cannot change shape for near focus → everything near appears blurry (cycloplegia).
This is useful for eye exams (doctor can see the whole retina), but dangerous in narrow-angle glaucoma (the wide pupil blocks fluid drainage channels → pressure spikes).
Analogy 4: Organophosphate Poisoning - The Stuck Accelerator
Normally, ACh is like your car's accelerator pedal. You press it (nerve fires), the car moves (organ responds), you release it (AChE destroys ACh), car returns to idle.
Organophosphate = supergluing the accelerator pedal to the floor. AChE is completely paralyzed. ACh keeps stimulating everything simultaneously: heart slows down to dangerous levels, lungs fill with secretions and go into spasm, bladder and bowel discharge involuntarily, muscles twitch then go limp.
Atropine = disconnects the engine from the pedal (blocks muscarinic receptors so the pedal being stuck doesn't matter for those effects). But the pedal is still stuck, so skeletal muscle (nicotinic) weakness persists.
Pralidoxime = mechanic who actually unsticks the pedal (reactivates AChE). Restores both muscarinic AND nicotinic control.
Analogy 5: Myasthenia Gravis + Neostigmine - The Failing Mail Route
In myasthenia gravis, the immune system attacks the nicotinic receptors at the neuromuscular junction (Nm). So letters (ACh) are sent, but half the mailboxes are destroyed. The message gets through weakly - muscles are too weak.
Neostigmine destroys the shredder (AChE) → letters pile up at the synapse → even the remaining mailboxes get letters read multiple times → muscle gets a stronger signal → patient can move better.
Analogy 6: The "DUMBELS" Flooding House
Imagine ACh is water, and the body is a house with many pipes. Normally, water flows in controlled amounts to each room (organ). AChE is a drainage system.
With organophosphate poisoning, the drainage fails. Water floods EVERY ROOM at once:
- Defecation room: pipes burst → uncontrolled diarrhea
- Urination bathroom: floods → incontinence
- Miosis eyes: pupils shrink in the flood
- Bradycardia heart room: slows to a crawl
- Emesis kitchen: vomiting
- Lacrimation tear ducts: overflow
- Salivation mouth: drooling
SECTION 5: STEP-BY-STEP CLINICAL REASONING
Case 1: Patient with Myasthenia Gravis
Scene: A 28-year-old woman presents with progressive muscle weakness, worse at end of day, drooping eyelids (ptosis), and double vision (diplopia). Symptoms improve after rest.
Step 1 - What organisms/cause?
Myasthenia gravis is an autoimmune disease. The body makes antibodies against nicotinic (Nm) receptors at the NMJ. Also anti-MuSK antibodies in some cases.
Step 2 - What is going wrong physiologically?
Motor nerve fires → ACh released → MOST nicotinic receptors are BLOCKED by antibodies
→ Very few receptors available for ACh to bind
→ Weak, easily fatigued muscle contraction
With repeated stimulation, ACh stores deplete faster than they are replenished → muscles fatigue during the day.
Step 3 - Which drug helps?
Neostigmine or Pyridostigmine (oral)
- Inhibits AChE → ACh accumulates in the NMJ → saturates even the reduced number of receptors → stronger muscle contraction
- Pyridostigmine preferred (longer acting, better tolerated)
Step 4 - What about patient factors?
- Tensilon (Edrophonium) test: Give IV edrophonium (ultra-short acting AChEI) → immediate improvement in ptosis/weakness for 5-10 min = diagnostic of myasthenia gravis
- Monitor for cholinergic crisis - if too much anticholinesterase given → excess ACh → SLUDGE symptoms + paradoxically MORE weakness (depolarization block at NMJ)
- Differentiate cholinergic crisis from myasthenic crisis by edrophonium: improves myasthenic crisis, worsens cholinergic crisis
Step 5 - Adverse effects to watch?
- SLUDGE symptoms from muscarinic overstimulation
- Can give glycopyrrolate or atropine alongside neostigmine to block unwanted muscarinic effects while allowing nicotinic (muscle) effect to continue
Case 2: Patient with Acute Angle-Closure Glaucoma
Scene: 65-year-old patient with sudden, severe eye pain, blurred vision, halos around lights, headache, nausea. Pupil is mid-dilated and non-reactive. Intraocular pressure (IOP) is 50 mmHg (normal <21).
Step 1 - What is happening anatomically?
In narrow-angle glaucoma: The drainage angle (trabecular meshwork) between the iris and cornea is very narrow. When the pupil dilates, the iris bunches up and physically blocks this drainage channel. Aqueous humor cannot drain → IOP skyrockets → optic nerve damage → permanent vision loss.
Step 2 - Which drugs are dangerous here?
Anything that DILATES the pupil (mydriasis):
- Antimuscarinics (atropine, tropicamide)
- Sympathomimetics (phenylephrine, decongestants)
- Tricyclic antidepressants
- Antihistamines
→ ALL are contraindicated in narrow-angle glaucoma
Step 3 - What drug HELPS?
Pilocarpine (cholinergic agonist, M3):
- Causes miosis (pupil constriction via iris sphincter)
- Opens the drainage angle
- Reduces IOP → emergency treatment while awaiting laser iridotomy
Also used for: Open-angle glaucoma (different mechanism - increases trabecular meshwork drainage via contraction of ciliary muscle)
Step 4 - Other glaucoma drugs (not cholinergic, for completeness):
- Beta-blockers (timolol): ↓ aqueous humor production
- Carbonic anhydrase inhibitors (acetazolamide): ↓ aqueous production
- Prostaglandin analogues (latanoprost): ↑ uveoscleral outflow
Case 3: Patient with COPD on Anticholinergic Inhaler
Scene: 68-year-old smoker with COPD on tiotropium. He also has benign prostatic hyperplasia (BPH).
Step 1 - Why tiotropium for COPD?
In COPD: The parasympathetic tone is relatively high → excessive M3-mediated bronchoconstriction and mucus secretion. Tiotropium blocks M1 and M3 receptors in the airway → bronchodilation + reduced secretions. Given as once-daily inhaled powder (reaches lungs directly - minimizes systemic effects).
Step 2 - Why does tiotropium have preference over ipratropium?
- Tiotropium shows kinetic selectivity: dissociates slowly from M3 (desired effect) but quickly from M2 (presynaptic). M2 inhibition would cause more ACh release → counteracts the M3 blockade. Tiotropium avoids this problem.
- Once-daily dosing (better compliance)
Step 3 - What is the BPH concern?
Any muscarinic blocker can relax the bladder (detrusor) → urinary hesitancy/retention. In BPH where flow is already impaired due to enlarged prostate, this worsens outflow → acute urinary retention.
Step 4 - Does inhaled tiotropium cause significant urinary effects?
- Very limited systemic absorption from inhaled route (quaternary ammonium → doesn't cross mucosa well; ~90% swallowed but not absorbed from GI)
- Risk of urinary retention with inhaled agents is low but real
- Monitor patient for urinary symptoms; may need to switch or add alpha-blocker for BPH
Case 4: Organophosphate Poisoning (Agricultural Worker)
Scene: Farm worker brought in confused, unconscious, with miosis, copious secretions from mouth, wheezing, bradycardia, muscle fasciculations, then paralysis.
Clinical reasoning:
- Recognize SLUDGE + DUMBELS = excess muscarinic stimulation
- Fasciculations + paralysis = nicotinic NMJ involvement
- Exposure history = organophosphate pesticide (or nerve agent)
Treatment reasoning:
Problem Drug Why
────────────────────────────────────────────────────────────────────
Bradycardia, bronchospasm, Atropine (IV, large) Blocks muscarinic receptors
secretions, GI symptoms titrated to secretions Dose to "dry" the lungs
Muscle weakness/paralysis Pralidoxime (2-PAM) Regenerates AChE before aging
(nicotinic) given EARLY Reverses both M and N effects
Seizures Diazepam Benzodiazepine for seizures
Respiratory failure Mechanical ventilation Paralyzed respiratory muscles
Skin exposure Decontamination Remove source of continued
poisoning
Key exam point: Atropine is titrated to DRYING OF SECRETIONS, not to heart rate. Very large doses (10-100 mg) may be needed. Do not stop early.
SECTION 6: MEMORY TOOLS
Mnemonic 1: Muscarinic Effects (Parasympathetic = "SLUDGE" or "DUMBELS")
SLUDGE:
- Salivation (↑)
- Lacrimation (↑ tears)
- Urination (↑ - bladder contracts)
- Defecation (↑ GI motility)
- GI distress (cramps, nausea, vomiting)
- Emesis (vomiting)
DUMBELS (preferred for organophosphate toxidrome):
- Defecation / Diarrhea
- Urination
- Miosis
- Bradycardia / Bronchoconstriction / Bronchorrhea
- Emesis
- Lacrimation
- Salivation / Sweating
Mnemonic 2: Anticholinergic Effects (Atropine Toxicity)
"Hot as a Hare, Dry as a Bone, Red as a Beet, Blind as a Bat, Mad as a Hatter, Full as a Flask, Fast as a Fiddle"
| Phrase | Effect | Organ |
|---|
| Hot as a Hare | Hyperthermia | ↓ Sweating |
| Dry as a Bone | Dry mouth, dry skin | ↓ Secretions |
| Red as a Beet | Flushing | Cutaneous vasodilation |
| Blind as a Bat | Blurred vision | Mydriasis + Cycloplegia |
| Mad as a Hatter | Delirium, hallucinations | CNS |
| Full as a Flask | Urinary retention | Bladder |
| Fast as a Fiddle | Tachycardia | Heart (M2 block) |
Mnemonic 3: Point and Shoot (Erection vs. Ejaculation)
- Parasympathetic = Point (erection)
- Sympathetic = Shoot (ejaculation)
Erection is mediated by parasympathetic (cholinergic) stimulation of blood flow.
Mnemonic 4: ACh Synthesis - "A CHAT in the terminal"
- A = Acetyl CoA
- CHAT = Choline Acetyltransferase (the enzyme)
- in the terminal = synthesis occurs in nerve terminal
Mnemonic 5: "Muscarinic M subtypes and G proteins" - M2 is the ODD ONE OUT
- M1, M3, M5 → Gq → increase IP3 → increase calcium (ODD numbers = Gq)
- M2, M4 → Gi → decrease cAMP (EVEN numbers = Gi = Inhibitory)
This matters because:
- M2 (heart) → Gi → ↓ cAMP → ↓ HR, ↓ conduction
- M3 (smooth muscle, glands) → Gq → ↑ Ca²+ → contraction, secretion
Mnemonic 6: Cholinergic Agonists - "BCMP"
Bethanechol - Bladder (urinary retention, ileus)
Carbachol - Cornea/Conjunctiva (glaucoma)
Methacholine - Measure airways (methacholine challenge for asthma)
Pilocarpine - Pressure in eye (glaucoma) + Parotid gland (xerostomia)
Comparison Table: Neostigmine vs. Physostigmine
| Feature | Neostigmine | Physostigmine |
|---|
| Chemical structure | Quaternary ammonium | Tertiary amine |
| Crosses BBB? | NO | YES |
| Origin | Synthetic | Natural (Calabar bean) |
| Duration | Short-moderate | Short |
| Clinical uses | Myasthenia gravis; reversal of NMJ block; ileus/retention | Antidote for anticholinergic (atropine) poisoning - ONLY one effective for CNS symptoms |
| Nicotinic effects? | YES (NMJ) | YES (NMJ + CNS) |
Comparison Table: Atropine vs. Scopolamine
| Feature | Atropine | Scopolamine |
|---|
| Chemical | Tertiary amine (racemate of hyoscyamine) | Tertiary amine |
| CNS penetration | Moderate | Greater |
| CNS effect | Stimulation (at doses above 5 mg) then sedation | Sedation/amnesia at low doses |
| Heart rate | Increases (more) | Less tachycardia than atropine |
| Uses | Bradycardia; organophosphate antidote; pre-anesthetic; eye exam; antisecretory | Motion sickness (transdermal); pre-anesthetic (amnesia); nausea/vomiting |
| Motion sickness | Less effective | More effective |
| Amnesia | Less | More - used in pre-anesthetic |
Drug Classification Summary Table
CHOLINERGIC (ACh-like) DRUGS
│
├── DIRECT AGONISTS (Muscarinic)
│ ├── Bethanechol → Bladder, GI
│ ├── Pilocarpine → Eye, dry mouth
│ ├── Carbachol → Eye (both M and N)
│ └── Methacholine → Diagnostic (asthma)
│
└── INDIRECT (Anticholinesterases)
├── Reversible
│ ├── Edrophonium → Diagnosis of MG
│ ├── Neostigmine → MG treatment, reversal of NMJ block
│ ├── Pyridostigmine → MG (preferred)
│ ├── Physostigmine → Antidote atropine poisoning
│ └── Donepezil/Rivastigmine/Galantamine → Alzheimer's
└── Irreversible (Organophosphates)
├── Echothiophate → Glaucoma
└── Parathion, Malathion, Sarin → Poisoning
ANTICHOLINERGIC DRUGS
│
├── MUSCARINIC ANTAGONISTS
│ ├── Tertiary Amines (cross BBB)
│ │ ├── Atropine → Bradycardia, organophosphate antidote, eye
│ │ ├── Scopolamine → Motion sickness, pre-anesthetic
│ │ └── Tropicamide/Homatropine → Eye exam
│ └── Quaternary Ammonium (NO BBB crossing)
│ ├── Ipratropium → COPD (inhaled)
│ ├── Tiotropium → COPD (inhaled, M1+M3 selective, once daily)
│ ├── Oxybutynin/Tolterodine/Solifenacin → OAB
│ └── Glycopyrrolate → Pre-anesthetic, antisecretory
│
├── GANGLIONIC BLOCKERS (Nn)
│ └── Trimethaphan, Hexamethonium (obsolete)
│
└── NMJ BLOCKERS (Nm)
├── Non-depolarizing: Atracurium, Vecuronium, Rocuronium, Pancuronium
└── Depolarizing: Succinylcholine
SECTION 7: EXAMINER'S CORNER
Most Tested Facts
- Atropine is the drug of choice for: bradycardia, organophosphate poisoning (muscarinic symptoms), pre-anesthetic (reduces secretions)
- Contraindication of atropine: Narrow-angle glaucoma (absolute), BPH, paralytic ileus
- Physostigmine is the antidote for: Anticholinergic (atropine) poisoning - ONLY drug that crosses BBB to reverse CNS effects
- Pralidoxime (PAM) works only if given early (before "aging" of organophosphate-AChE complex)
- Succinylcholine is a depolarizing NMJ blocker; causes hyperkalemia (dangerous in burns, crush injury, upper motor neuron lesions, denervation)
- Pilocarpine is used for both glaucoma and xerostomia (Sjogren's, post-radiation)
- Tiotropium is M1+M3 selective; once-daily; preferred in COPD over ipratropium
- Bethanechol is used for postoperative ileus and neurogenic bladder; given orally or SC (NEVER IV)
- Neostigmine + glycopyrrolate = used together to reverse neuromuscular blockade (neostigmine causes NMJ AChE inhibition; glycopyrrolate prevents muscarinic side effects)
- M2 receptors are in the heart; M3 receptors are in smooth muscle and glands
Most Likely Essay Questions
- "Describe the synthesis, storage, release and degradation of acetylcholine. Discuss the pharmacological interventions possible at each step."
- "Classify cholinergic drugs with examples. Describe the mechanism of action, pharmacological effects, and clinical uses of neostigmine."
- "Describe the pharmacology of atropine. Include mechanism, pharmacological effects (dose-dependent), clinical uses, adverse effects, contraindications, and treatment of atropine poisoning."
- "Write an essay on organophosphate poisoning: pathophysiology, clinical features, and management."
- "Describe the classification and pharmacology of anticholinergic drugs used in COPD."
Most Likely Short Notes
- Pilocarpine
- Neostigmine vs. Atropine
- Succinylcholine
- Tiotropium in COPD
- Myasthenia gravis management
- Organophosphate poisoning treatment
- Physostigmine as antidote
- Pralidoxime
- Muscarinic receptor subtypes (M1-M5)
- Donepezil in Alzheimer's disease
Most Likely Viva Questions
| Question | Expected Answer |
|---|
| Where is ACh synthesized? | In the nerve terminal (cytosol), by choline acetyltransferase (ChAT) |
| What is the rate-limiting step in ACh synthesis? | Uptake of choline into nerve terminal |
| What enzyme degrades ACh? | Acetylcholinesterase (AChE) in the synapse |
| Why is ACh not used therapeutically? | Destroyed too rapidly by AChE; no selectivity |
| What is the Tensilon test? | IV edrophonium (AChEI) → dramatic brief improvement in MG = positive test |
| Why is atropine used in organophosphate poisoning? | Blocks muscarinic receptors → reverses SLUDGE, bradycardia, bronchospasm |
| Why is atropine insufficient alone in OP poisoning? | Does not reverse nicotinic effects (muscle weakness) - need pralidoxime |
| Why is physostigmine better than neostigmine for atropine poisoning? | Physostigmine is tertiary (crosses BBB); neostigmine is quaternary (does not cross BBB) |
| What is the paradoxical bradycardia with low-dose atropine? | Very low doses block presynaptic M1 autoreceptors on vagal nerve → more ACh released → initial bradycardia before higher doses produce tachycardia |
| What is "aging" in organophosphate poisoning? | Strengthening of organophosphate-AChE covalent bond with time → pralidoxime can no longer reactivate AChE |
| Why does succinylcholine cause hyperkalemia? | Persistent membrane depolarization → K+ exits all muscle cells simultaneously → ↑ serum K+ |
| What reverses non-depolarizing NMJ blockade? | Neostigmine (+ glycopyrrolate to block muscarinic effects) |
| What reverses depolarizing block? | NOTHING pharmacologically - wait for metabolism (succinylcholine is broken down by plasma pseudocholinesterase) |
Most Likely MCQs
Q1: A patient is given a drug that causes dry mouth, urinary retention, blurred vision, and tachycardia. What is the mechanism?
A: Muscarinic receptor blockade (anticholinergic)
Q2: Physostigmine differs from neostigmine in that physostigmine:
A: Crosses the blood-brain barrier (tertiary amine)
Q3: A farmer presents with pinpoint pupils, excessive secretions, bradycardia, and muscle fasciculations. Which drug should be given FIRST?
A: Atropine (controls life-threatening muscarinic symptoms)
Q4: The drug used for diagnosis of myasthenia gravis is:
A: Edrophonium (Tensilon test)
Q5: Which drug is used for overactive bladder with selectivity for M3?
A: Darifenacin or Solifenacin
Q6: The "aging" phenomenon in organophosphate poisoning means:
A: Covalent bond between organophosphate and AChE becomes irreversible, making pralidoxime ineffective
Q7: Bethanechol should NOT be given by which route?
A: Intravenous (causes severe hypotension and cardiac arrhythmias)
Q8: Which anticholinesterase is used in Alzheimer's disease?
A: Donepezil, Rivastigmine, Galantamine
Q9: Succinylcholine is contraindicated in:
A: Burns, crush injuries, denervation injuries (risk of fatal hyperkalemia)
Q10: The paradoxical bradycardia with low doses of atropine is due to:
A: Blockade of presynaptic M1 autoreceptors on vagal nerve endings → enhanced ACh release
Common Traps Students Fall Into
Trap 1: "Atropine causes miosis"
Correction: Atropine causes MYDRIASIS (pupil dilation). Cholinergic drugs cause miosis.
Trap 2: "Neostigmine crosses the blood-brain barrier"
Correction: Neostigmine is a QUATERNARY ammonium - does NOT cross BBB. Physostigmine (tertiary) does.
Trap 3: "Pralidoxime can always reverse organophosphate poisoning"
Correction: Pralidoxime is only effective BEFORE aging occurs. Give early!
Trap 4: "Atropine is contraindicated in all types of glaucoma"
Correction: Atropine is only contraindicated in NARROW-ANGLE (closed-angle) glaucoma. Open-angle glaucoma is managed differently and is not an absolute contraindication to systemic atropine.
Trap 5: "Succinylcholine can be reversed by neostigmine"
Correction: Succinylcholine is a DEPOLARIZING blocker. Neostigmine (AChEI) would actually PROLONG its action by increasing ACh (which also depolarizes). Reversal is by waiting.
Trap 6: "Pilocarpine is only for glaucoma"
Correction: Also used for xerostomia (dry mouth) in Sjogren's syndrome and post-radiation.
Trap 7: "Bethanechol works on both muscarinic and nicotinic receptors"
Correction: Bethanechol is muscarinic SELECTIVE. Carbachol acts on both.
Trap 8: "Anticholinesterases only work at muscarinic receptors"
Correction: They increase ACh everywhere - muscarinic AND nicotinic (NMJ + ganglia). This is why neostigmine helps MG (nicotinic NMJ) while also causing SLUDGE (muscarinic). That's why glycopyrrolate is co-administered.
SECTION 9: HIGH-YIELD REVISION SHEET
╔══════════════════════════════════════════════════════════════════╗
║ CHOLINERGIC & ANTICHOLINERGIC - ONE-PAGE REVIEW ║
╠══════════════════════════════════════════════════════════════════╣
║ ║
║ ACh LIFECYCLE: ║
║ Choline + AcCoA → [ChAT] → ACh → Vesicle → Ca²+ → Release ║
║ → Receptor → [AChE] → Choline + Acetate → Recycled ║
║ ║
║ RECEPTORS: ║
║ Muscarinic (M1-M5) = GPCR; M1,3,5=Gq; M2,4=Gi ║
║ Nicotinic (Nn, Nm) = Ligand-gated ion channel ║
║ ║
║ MUSCARINIC EFFECTS (SLUDGE/DUMBELS): ║
║ Heart: ↓HR (M2) | Eye: miosis, accommodation (M3) ║
║ Glands: ↑secretions (M3) | GI: ↑motility (M3) ║
║ Bladder: contracts (M3) | Bronchi: constrict (M3) ║
║ ║
╠══════════════════════════════════════════════════════════════════╣
║ MUST-KNOW DRUGS - CHOLINERGIC: ║
║ ║
║ Bethanechol → Ileus, urinary retention (NEVER IV) ║
║ Pilocarpine → Glaucoma, xerostomia (Sjogren's) ║
║ Methacholine → Asthma diagnosis (provocation test) ║
║ Edrophonium → MG diagnosis (Tensilon test) ║
║ Neostigmine → MG treatment, reverse NMJ block ║
║ Pyridostigmine → MG (long-term, preferred) ║
║ Physostigmine → Antidote: atropine/anticholinergic poisoning ║
║ Pralidoxime → Antidote: organophosphate poisoning (early!) ║
║ Donepezil/Rivastigmine → Alzheimer's disease ║
║ ║
╠══════════════════════════════════════════════════════════════════╣
║ MUST-KNOW DRUGS - ANTICHOLINERGIC: ║
║ ║
║ Atropine → Bradycardia, AV block, OP antidote, pre-anesthetic ║
║ Scopolamine → Motion sickness (transdermal), amnesia ║
║ Ipratropium → COPD/Asthma (inhaled) ║
║ Tiotropium → COPD (M1+M3, once-daily inhaled) ║
║ Oxybutynin/Tolterodine/Solifenacin → Overactive bladder ║
║ Glycopyrrolate → Pre-anesthetic, co-given with neostigmine ║
║ Succinylcholine → Rapid intubation (depolarizing NMJ block) ║
║ Atracurium/Vecuronium/Rocuronium → Non-depolaring NMJ block ║
║ ║
╠══════════════════════════════════════════════════════════════════╣
║ MUST-KNOW TOXICITIES: ║
║ ║
║ Anticholinergic syndrome: "Hot, Dry, Red, Blind, Mad, Full, ║
║ Fast" - Antidote = Physostigmine ║
║ ║
║ Organophosphate: DUMBELS + fasciculations/paralysis ║
║ Tx: Atropine (titrate to secretions) + Pralidoxime (early) ║
║ ║
║ Succinylcholine: Hyperkalemia (burns/crush/denervation), ║
║ Malignant hyperthermia (Rx: dantrolene) ║
║ ║
╠══════════════════════════════════════════════════════════════════╣
║ KEY CONTRAINDICATIONS: ║
║ ║
║ Antimuscarinics → Narrow-angle glaucoma (absolute!), BPH ║
║ Cholinergic agonists → Asthma, COPD, bowel obstruction ║
║ Succinylcholine → Burns, crush injury, denervation ║
║ Bethanechol IV → Contraindicated (use SC or oral only) ║
║ ║
╠══════════════════════════════════════════════════════════════════╣
║ EXAM EMERGENCY FACTS: ║
║ ║
║ 1. M2=Heart (Gi); M3=Smooth muscle/glands (Gq) ║
║ 2. Physostigmine = ONLY anticholinesterase crossing BBB ║
║ 3. Neostigmine reversal of NMJ block: ADD glycopyrrolate ║
║ 4. Pralidoxime must be given EARLY (before aging) ║
║ 5. Paradoxical bradycardia = low-dose atropine ║
║ 6. Atropine titrated to DRY SECRETIONS in OP poisoning ║
║ 7. Non-depolarizing reversed by neostigmine; depolarizing NOT ║
║ 8. Tiotropium is once-daily; ipratropium is 4x daily ║
║ 9. Nicotinic receptors are ligand-gated ion channels (FAST) ║
║ 10. Muscarinic receptors are GPCRs (SLOW, via 2nd messengers) ║
╚══════════════════════════════════════════════════════════════════╝
SECTION 10: SELF-ASSESSMENT
Q1: A 55-year-old man undergoes abdominal surgery. On day 2 post-operation, he has not passed stool or flatus. Bowel sounds are absent. Which drug would help, and why?
Answer: Bethanechol (or neostigmine). Post-operative ileus is caused by reduced GI motility following abdominal surgery and general anesthesia. Bethanechol is a direct muscarinic agonist (M3) that stimulates GI smooth muscle contraction, increases motility, and restores bowel function. Neostigmine (anticholinesterase) is also effective and actually preferred for acute colonic pseudo-obstruction (Ogilvie's syndrome). Route: Bethanechol given SC or orally - NEVER IV (risks severe hypotension and cardiac events).
Q2: Explain why atropine is used in organophosphate poisoning, and why it is not the complete treatment.
Answer: Atropine is a muscarinic receptor blocker. In organophosphate poisoning, irreversible AChE inhibition causes massive ACh accumulation at all synapses. Atropine blocks the muscarinic effects (bradycardia, bronchospasm, excessive secretions, GI symptoms, miosis) - these are life-threatening and atropine is titrated to dry the secretions. However, ACh also accumulates at nicotinic receptors (NMJ and ganglia) - causing fasciculations and then paralysis (including respiratory muscle paralysis), which atropine CANNOT reverse because nicotinic receptors are structurally different from muscarinic receptors. Pralidoxime (PAM) is needed to regenerate AChE and reverse both muscarinic AND nicotinic effects, but must be given early before "aging."
Q3: What is the paradoxical bradycardia seen with low doses of atropine? Why does it occur?
Answer: At very low doses (< 0.5 mg), atropine can cause initial bradycardia (slowing of heart rate) before its expected tachycardia effect. This occurs because at low concentrations, atropine preferentially blocks presynaptic M1 autoreceptors on vagal nerve endings (these receptors normally provide negative feedback to reduce ACh release). By blocking M1, atropine removes this inhibition → MORE ACh is released from the vagus → MORE M2 receptor activation → bradycardia. At higher doses, atropine blocks M2 receptors on the SA node directly → tachycardia.
Q4: A patient is given succinylcholine for intubation. An hour later, the patient has still not recovered muscle function. What is the most likely cause, and what should be done?
Answer: Pseudocholinesterase (plasma cholinesterase) deficiency. Succinylcholine is normally hydrolyzed rapidly by plasma pseudocholinesterase (also called butyrylcholinesterase) to terminate its action. In patients with a genetic deficiency of this enzyme (autosomal recessive), succinylcholine cannot be broken down → prolonged paralysis (up to several hours). Management: Continue mechanical ventilation and supportive care. NEVER give neostigmine (it would increase ACh, potentiating the depolarizing block). Wait for drug to be eventually metabolized.
Q5: Why does anticholinergic poisoning cause hyperthermia, and how is this particularly dangerous in children?
Answer: Sweat glands have muscarinic receptors (M3), despite being innervated by sympathetic nerves (an exception to the rule). Anticholinergic drugs block these M3 receptors → sweating ceases. Sweating is the body's main mechanism of heat dissipation (evaporative cooling). Without sweating, body temperature rises unchecked → hyperthermia, potentially reaching 40-41°C or higher. Children are more susceptible because: (1) they have a higher metabolic rate relative to body size generating more heat, (2) they have a larger body surface area relative to weight increasing ambient heat absorption, (3) they are less able to regulate body temperature. High-dose atropine in children can be fatal from hyperthermia alone. Treatment includes ice packs, sponging, and physostigmine.
Q6: Compare the mechanisms of action of pilocarpine and timolol in treating glaucoma.
Answer: Both drugs lower intraocular pressure (IOP) but by completely different mechanisms. Pilocarpine is a direct muscarinic (M3) agonist. It contracts the ciliary muscle, which pulls the scleral spur open → widens the trabecular meshwork → increases aqueous humor outflow. It also constricts the pupil (miosis), which opens the drainage angle (useful in narrow-angle glaucoma). Timolol is a beta-2 adrenergic blocker. The ciliary epithelium uses beta-2 receptors to drive active secretion of aqueous humor. Timolol blocks these receptors → reduces aqueous humor PRODUCTION. Net effect: both lower IOP, but pilocarpine increases outflow while timolol decreases inflow.
Q7: Why is glycopyrrolate combined with neostigmine when reversing neuromuscular blockade after surgery?
Answer: Neostigmine is an anticholinesterase - it increases ACh at ALL cholinergic synapses. At the NMJ (nicotinic), this is the desired effect: accumulated ACh competes with the non-depolarizing blocker and restores muscle contraction. However, ACh also accumulates at muscarinic junctions simultaneously: causing bradycardia, increased salivation, bronchospasm, and gut cramps. Glycopyrrolate is a quaternary ammonium muscarinic blocker that selectively blocks these unwanted muscarinic side effects. It is quaternary (does not cross BBB) and does not affect the NMJ (nicotinic) action of neostigmine. The combination provides NMJ reversal without cardiovascular or GI side effects.
Q8: Describe the clinical features that distinguish cholinergic crisis from myasthenic crisis, and how the Tensilon test helps.
Answer: Both crises cause severe muscle weakness in a myasthenia gravis patient, which can be life-threatening.
| Feature | Myasthenic Crisis | Cholinergic Crisis |
|---|
| Cause | Insufficient anticholinesterase (underdosing) or disease worsening | Excess anticholinesterase (overdosing) |
| Muscarinic signs | Absent | SLUDGE present (sweating, salivation, miosis, bradycardia) |
| Pupils | Normal/large | Pinpoint (miosis) |
| Secretions | Normal | Increased |
| Heart rate | Normal/fast | Slow (bradycardia) |
Tensilon (edrophonium) test: Give 2 mg IV edrophonium, then 8 mg if no reaction.
- Myasthenic crisis: Improves dramatically (more ACh helps)
- Cholinergic crisis: Worsens (even more ACh makes it worse)
Q9: A 70-year-old woman with overactive bladder is prescribed oxybutynin. She develops worsening confusion and falls. Explain the pharmacological basis and suggest an alternative.
Answer: Oxybutynin is a muscarinic (M3) blocker that relaxes the bladder detrusor muscle to treat OAB. However, oxybutynin is a tertiary amine - it crosses the blood-brain barrier. In elderly patients, blockade of central muscarinic receptors (especially M1 in the hippocampus and cortex) causes anticholinergic CNS effects: confusion, cognitive impairment (anticholinergic delirium), worsening of any pre-existing dementia, and sedation contributing to falls. Elderly patients are particularly vulnerable (less cholinergic reserve in the brain, altered pharmacokinetics). Alternative: Trospium (quaternary ammonium, does not cross BBB); or Solifenacin/Darifenacin (M3-selective with less CNS penetration). Darifenacin has high M3 selectivity and minimal CNS effects.
Q10: Explain the mechanism of action of botulinum toxin and its therapeutic applications.
Answer: Botulinum toxin (BoTox) is produced by Clostridium botulinum. It is a zinc-dependent metalloprotease that cleaves SNARE proteins (specifically SNAP-25, syntaxin, synaptobrevin) - these are the proteins required for synaptic vesicle fusion with the presynaptic membrane. Without vesicle fusion, acetylcholine cannot be released from cholinergic nerve terminals.
Effects:
- NMJ (Nm): Muscle paralysis (flaccid)
- Autonomic: Reduced secretions, reduced smooth muscle contraction
Therapeutic uses:
- Ophthalmology: Strabismus (squint), blepharospasm (eyelid spasm)
- Neurology: Focal dystonia (cervical dystonia/torticollis), writer's cramp, hemifacial spasm, chronic migraine
- Cosmetics: Wrinkle treatment (temporary facial muscle relaxation)
- Urology: Overactive bladder (injection into detrusor)
- Hyperhidrosis: Injection into sweat glands
- GI: Achalasia (injection into lower esophageal sphincter)
Duration: Effect lasts 3-4 months (until new nerve sprouting and new ACh release mechanism develops). Does NOT "age" like organophosphates; the block eventually reverses through axon regeneration.
End of Complete Learning Note
Sources: Goodman & Gilman's The Pharmacological Basis of Therapeutics (14th ed); Lippincott Illustrated Reviews: Pharmacology (7th ed); Guyton & Hall Textbook of Medical Physiology (14th ed); Katzung's Basic and Clinical Pharmacology (16th ed)