Comparative table of genito ulcerative disease
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the data needed. Let me build the comprehensive comparative table.
Comparative Table of Genital Ulcerative Diseases
The image below (from Berek & Novak's Gynecology) shows the cross-sectional ulcer morphology: (A) Chancroid - wide, deep, undermined; (B) Herpes - shallow, superficial; (C) Syphilis - narrow, deep, clean base.
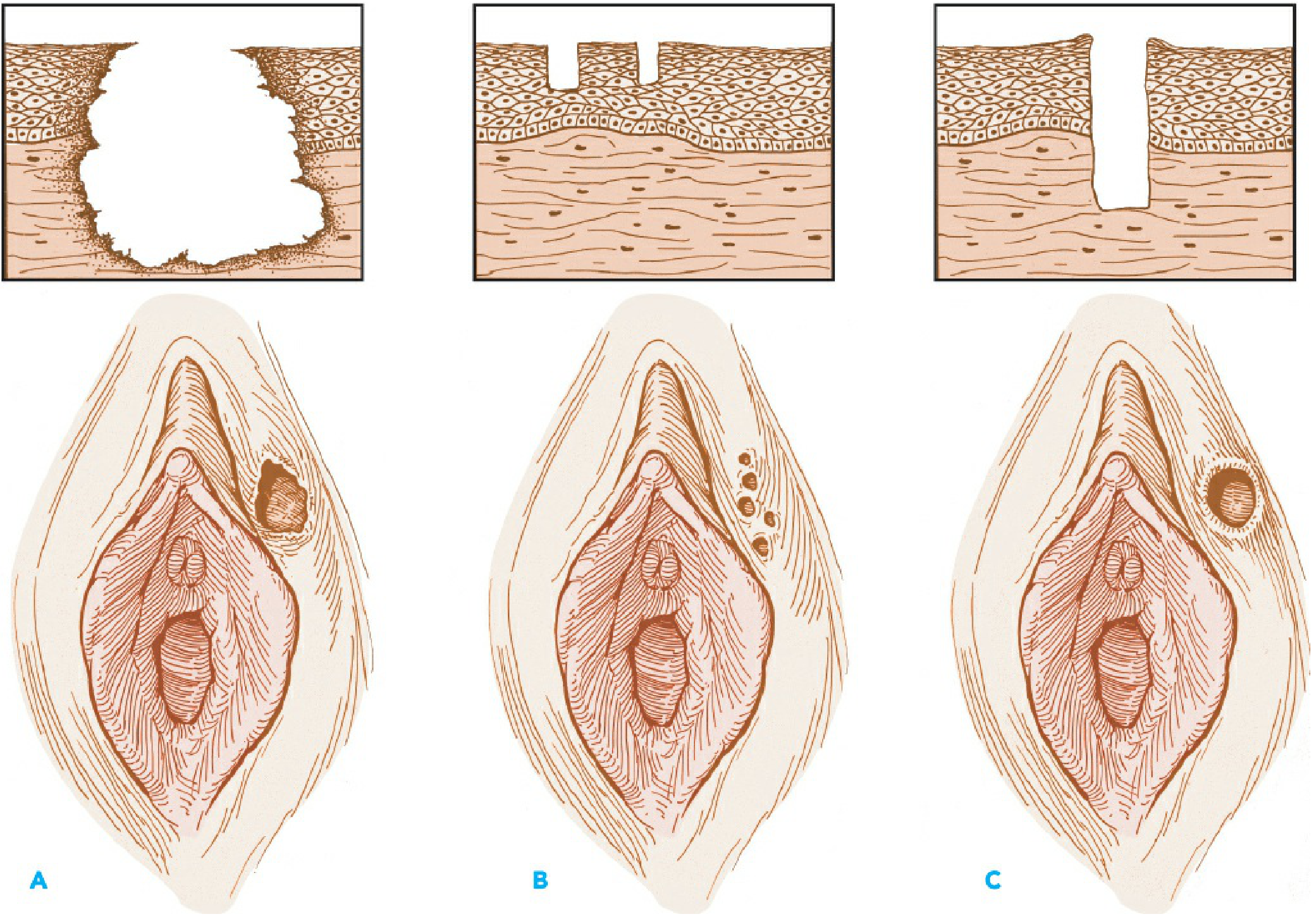
Table: Clinical Features of Genital Ulcer Diseases
(Based on Harrison's Table 141-7, Tintinalli's Table 153-3, and Jawetz Table 48-6)
| Feature | Syphilis | Genital Herpes (HSV) | Chancroid | Lymphogranuloma Venereum (LGV) | Donovanosis (Granuloma Inguinale) |
|---|---|---|---|---|---|
| Causative organism | Treponema pallidum (spirochete) | HSV-2 (mainly); HSV-1 | Haemophilus ducreyi (gram-negative rod) | Chlamydia trachomatis serovars L1, L2, L3 | Klebsiella granulomatis (formerly Calymmatobacterium) |
| Incubation period | 9-90 days (avg. 3 weeks) | 2-7 days | 1-14 days (avg. 3-5 days) | 3 days - 6 weeks | 1-4 weeks (up to 6 months) |
| Primary lesion | Papule → ulcer (chancre) | Vesicle → pustule → ulcer | Pustule → ulcer | Papule, pustule, or vesicle (often transient, missed) | Papule → nodule → ulcer |
| Number of lesions | Usually one | Multiple, clustered | Usually multiple, may coalesce | Usually one; often undetected | Variable |
| Diameter | 5-15 mm | 1-2 mm each | Variable | 2-10 mm | Variable |
| Edges | Sharply demarcated, elevated, round/oval | Erythematous, irregular | Undermined, ragged, irregular | Elevated, round, or oval | Elevated, irregular |
| Base | Smooth, clean, nonpurulent, relatively avascular | Serous, erythematous, nonvascular | Purulent, bleeds easily | Variable, nonvascular | Red, velvety ("beefy"), bleeds readily |
| Depth | Superficial or deep | Superficial | Excavated (deep) | Superficial or deep | Elevated/hypertrophic |
| Induration | Firm (indurated) | None | Soft | Occasionally firm | Firm |
| Pain | Uncommon (painless) | Frequently tender | Usually very tender | Variable | Uncommon (painless) |
| Inguinal lymphadenopathy | Firm, nontender, bilateral (rubbery nodes) | Firm, tender, often bilateral (initial episode) | Tender, may suppurate ("bubo"), loculated, usually unilateral | Tender, may suppurate, loculated, unilateral - "groove sign" | None; pseudobuboes (subcutaneous granulomas) |
| Systemic features | Secondary: rash, mucous patches, lymphadenopathy. Tertiary: cardiac, CNS, gummas | Fever, headache, malaise (primary episode) | Usually localized | Systemic: fever, malaise, proctocolitis, fistulas, strictures | Usually localized; may spread via autoinoculation |
| Key mnemonic | Painless, indurated, "clean" | Painful vesicles, recurrent | Painful, purulent, soft | "Groove sign"; inguinal bubo dominates | Painless, beefy-red, bleeds |
| Diagnostic tests | Dark-field microscopy; RPR/VDRL (non-treponemal); FTA-ABS / MHA-TP (treponemal); PCR | Viral culture, direct FA, PCR; type-specific serology | Culture on enriched vancomycin medium at 33°C; PCR | NAAT (PCR); serology; culture of bubo aspirate | Tissue biopsy: Donovan bodies (intracellular gram-negative rods in macrophages) |
| Treatment (1st line) | Benzathine penicillin G 2.4 MU IM single dose (primary/secondary) | Acyclovir / Valacyclovir / Famciclovir (episodic or suppressive) | Azithromycin 1 g PO single dose OR Ceftriaxone 250 mg IM single dose | Doxycycline 100 mg PO BD x 21 days | Azithromycin 1 g PO weekly OR Doxycycline 100 mg BD x ≥3 weeks |
| Treatment (alternative) | Doxycycline 100 mg BD x 14 days (if penicillin allergy) | Topical antivirals less effective; suppressive therapy for recurrences | Ciprofloxacin 500 mg BD x 3 days; Erythromycin 500 mg TID x 7 days | Erythromycin 500 mg QID x 21 days | Erythromycin, trimethoprim-sulfamethoxazole, or ciprofloxacin |
| Recurrence | No (each stage is progressive) | Yes (latent in dorsal root ganglia; HSV-2 recurs more than HSV-1) | No | No | No |
| HIV risk | Increased (disrupted mucosal barrier) | Increased | High cofactor (10% coinfection with HSV or syphilis) | Increased | Increased |
| Epidemiology | Worldwide; resurgent in MSM | Most common cause of genital ulcer in developed countries | Prevalent in Africa, Asia, Caribbean; rare in USA | Developing countries; outbreaks in MSM (Europe, North America, Australia) | Endemic in Africa, India, Papua New Guinea, Australia; rare in USA/Europe |
Quick Clinical Memory Aid
| Disease | Pain? | Lesion feel | Nodes | Organism type |
|---|---|---|---|---|
| Syphilis | No | Hard (indurated) | Rubbery, non-tender | Spirochete |
| Herpes | Yes | Soft (vesicles/shallow) | Tender, bilateral | Virus |
| Chancroid | Yes (very) | Soft, deep, purulent | Tender, bubo | Gram-negative rod |
| LGV | Variable | Transient ulcer; nodes dominate | Tender bubo (groove sign) | Intracellular bacteria |
| Donovanosis | No | Firm, beefy-red | None (pseudobuboes) | Intracellular gram-negative |
Sources:
- Harrison's Principles of Internal Medicine 22E (2025), Table 141-7 - Clinical Features of Genital Ulcer
- Tintinalli's Emergency Medicine, Table 153-3 - Clinical Features of Genital Ulcerative Infections
- Jawetz, Melnick & Adelberg's Medical Microbiology 28E, Table 48-6 - Major Genital Sore Diseases
- Berek & Novak's Gynecology - Genital Ulcer Disease section
This is a shared conversation. Sign in to Orris to start your own chat.