Teach me diffuse axonal injury
Reading File
Finding Sources
Searching PubMed
"diffuse axonal injury"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
Loading Image
I now have rich, comprehensive content from multiple authoritative sources. Let me compose the full teaching answer.
Diffuse Axonal Injury (DAI)
Definition
Diffuse axonal injury (DAI) - also called traumatic axonal injury (TAI) or shear injury - is the widespread disruption of axonal fibers in the white matter tracts of the brain caused by angular acceleration-deceleration forces. It is one of the most common and devastating forms of traumatic brain injury (TBI).
- Harrison's Principles of Internal Medicine 22E, p. 3616
- Sabiston Textbook of Surgery, p. 1329
Mechanism & Pathophysiology
The key force is rotational (angular) acceleration-deceleration rather than direct impact. The brain and skull rotate at different rates, generating shearing and stretching forces on axons. This is why DAI is classically seen after:
- High-velocity motor vehicle collisions (restrained or unrestrained)
- Falls from height
- Blast injuries (even without skull impact)
- Shaken baby syndrome in infants
Two-phase axonal injury
- Primary axotomy - immediate mechanical stretching and tearing of axonal fibers at the moment of impact, causing functional or anatomic disruption of white matter pathways
- Secondary axotomy - over the subsequent 6-12 hours, apoptosis and wallerian degeneration propagate the injury further. Disruption of axoplasmic flow causes axonal swelling (retraction bulbs), ionic dysregulation, and calcium influx
Notably, even in blast injuries, sufficient angular acceleration can cause DAI without the skull being struck.
Sabiston Textbook of Surgery; Robbins Pathologic Basis of Disease, p. 3913
Neuropathology (Microscopic)
- Axonal swellings (retraction bulbs) appear within hours of injury - best seen on silver impregnation stains
- Immunoperoxidase stains for axonally transported proteins are most sensitive:
- Amyloid beta precursor protein (APP) - most widely used marker
- Alpha-synuclein
- Later: increased microglia in damaged cortex, then degeneration of involved fiber tracts
- Macroscopic: focal hemorrhagic lesions in deep white matter, corpus callosum, and brainstem
Robbins, Cotran & Kumar Pathologic Basis of Disease
Grading (Adams Classification)
Lesion distribution correlates with severity:
| Grade | Location of lesions | Clinical severity |
|---|---|---|
| I | Lobar white matter / centrum semiovale | Mild-moderate TBI |
| II | + Corpus callosum (splenium or body) | Moderate-severe |
| III | + Brainstem (dorsolateral quadrant, superior peduncle) | Severe TBI, deep coma |
Severity of consciousness impairment and brain swelling are generally proportional to grade.
Fischer's Mastery of Surgery 8e, p. 2962; Grainger & Allison's Diagnostic Radiology, p. 1395
Clinical Features
- Immediate loss of consciousness - up to 50% of patients who develop coma after TBI without contusions have DAI
- Neurological impairment disproportionately severe relative to CT findings - this mismatch is the classic clinical clue
- Spectrum from mild (concussion-like, transient dysfunction) to severe (persistent coma, vegetative state)
- Coma is explained by damage to the ascending arousal system connecting the brainstem to the forebrain (the reticular activating system)
- In severe cases, neurons of the dorsal pons - which sits just under the tentorium - are directly sheared
Plum & Posner's Diagnosis and Treatment of Stupor and Coma; Robbins p. 3913
Key red flag
A patient who fails to wake up after evacuation of a subdural or epidural hematoma, or who is unconscious despite a negative CT, should prompt consideration of DAI.
- Sabiston Textbook of Surgery, p. 1337
Imaging
CT scan
- Often normal or near-normal - CT misses most DAI
- When positive: punctate hemorrhagic foci at the gray-white matter junction, in the deep white matter, corpus callosum, or brainstem
- Only hemorrhagic lesions large enough to be hyperdense are visible; CT represents "the tip of the iceberg"
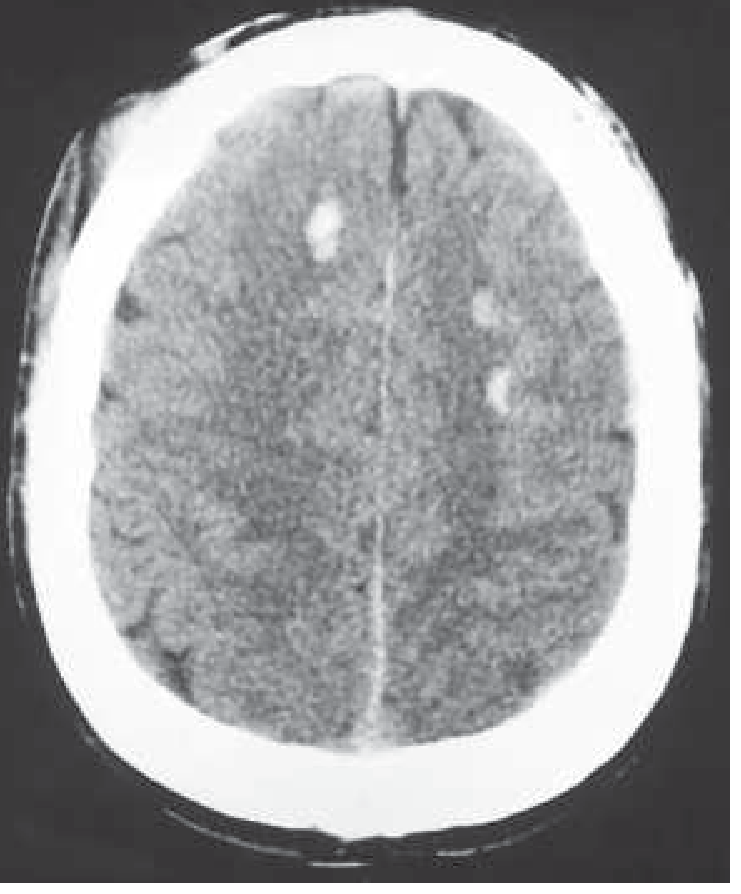
CT showing multiple small areas of hemorrhage in frontal white matter typical of diffuse axonal shearing - Harrison's Principles of Internal Medicine
MRI - gold standard for DAI detection
MRI is far more sensitive than CT. Key sequences:
| Sequence | What it shows |
|---|---|
| SWI (susceptibility-weighted imaging) | Most sensitive - detects microbleeds as hypointense foci even when CT is normal |
| GRE (gradient-recalled echo / T2*) | Detects hemosiderin/blood products |
| DWI / DTI (diffusion tensor imaging) | Best for white matter tract damage; useful in subacute phase |
| FLAIR | Edema and non-hemorrhagic axonal damage |
The SWI sequence typically reveals the full extent of injury, showing many more lesions than CT - this gap between CT and SWI findings is diagnostically important.
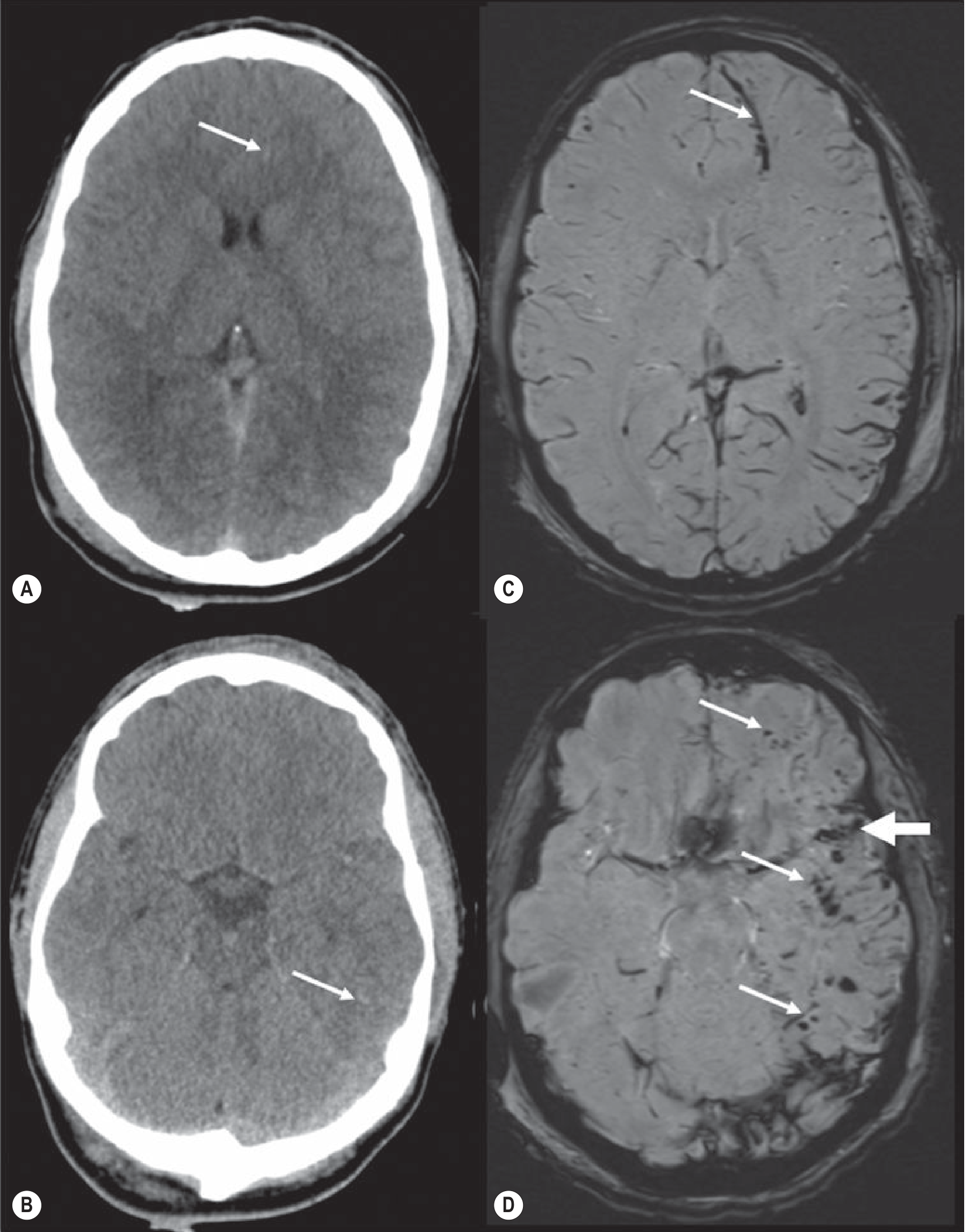
CT (A,B) vs SWI (C,D) in the same patient - SWI reveals far more DAI lesions. Grade II injury with corpus callosum involvement confirmed - Grainger & Allison's Diagnostic Radiology
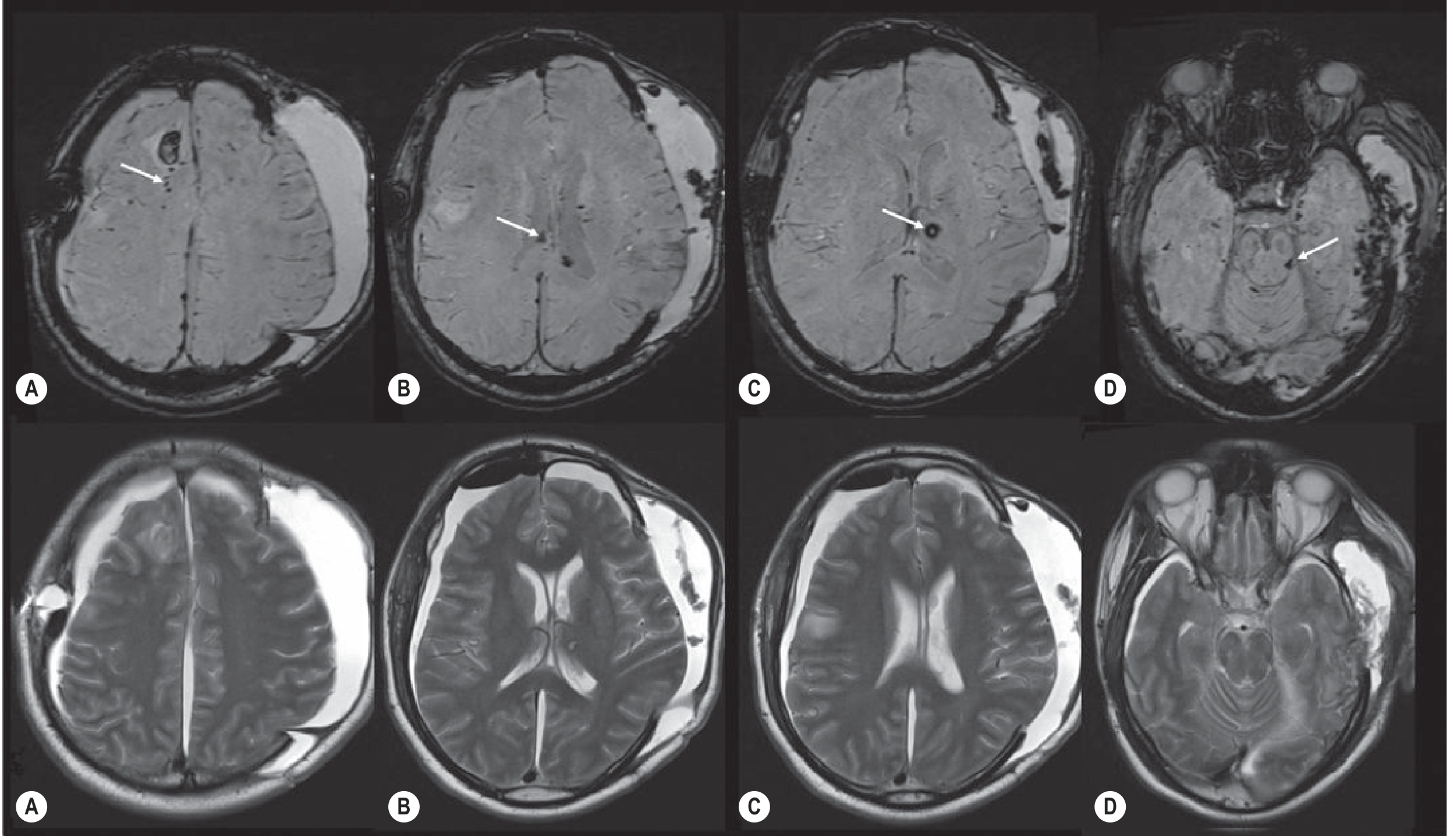
SWI (upper row) vs T2 (lower row) in severe DAI. SWI shows hemorrhagic hypointense foci in frontal white matter (A), corpus callosum (B), thalamus (C), and brainstem (D), confirming Grade I-III DAI. T2 misses most lesions - Grainger & Allison's Diagnostic Radiology
Management
There is no specific treatment for DAI - management is entirely supportive and preventive, aimed at limiting secondary brain injury.
Goals
- Prevent secondary brain injury - the main modifiable target
- Avoid hypoxia (SaO₂ < 90%) and hypotension (SBP < 90 mmHg)
- ICP monitoring and control
- Maintain cerebral perfusion pressure (CPP)
ICP management strategies (stepwise)
- Sedation and analgesia
- Head-of-bed elevation 30°
- Osmotic therapy (mannitol or hypertonic saline)
- External ventricular drain (EVD) for CSF drainage
- Decompressive craniectomy in refractory cases (~10% of severe DAI patients require this)
What NOT to do
- No role for steroids (CRASH trial showed harm)
- No proven neuroprotective agent to date (glibenclamide and xenon gas are under investigation)
Fischer's Mastery of Surgery 8e; Sabiston Textbook of Surgery; Tintinalli's Emergency Medicine
Prognosis
DAI carries a serious prognosis, especially at higher grades. Key prognostic factors include:
- GCS motor score - the single most important prognosticator
- Grade of DAI (I/II/III)
- CT findings (basal cistern effacement, midline shift)
- Pupillary responses
- Associated injuries
A 2025 systematic review and meta-analysis (PMID: 40485292) specifically examining DAI frequency and outcomes in severe TBI provides the most current evidence - this is worth noting as outcomes data continues to evolve.
Long-term sequelae include cognitive decline, persistent vegetative state, chronic disability, and dementia (TBI accounts for at least 3% of all dementia cases).
Mulholland and Greenfield's Surgery 7e; Sabiston Textbook of Surgery
Quick Summary
| Feature | DAI |
|---|---|
| Mechanism | Angular acceleration-deceleration |
| Pathology | Axonal shearing → retraction bulbs, APP staining |
| Classic site | White matter, corpus callosum, brainstem |
| CT | Often normal; punctate hemorrhages if present |
| Best imaging | MRI-SWI |
| Grading | I (WM) → II (+ corpus callosum) → III (+ brainstem) |
| Coma cause | Disruption of ascending arousal system |
| Treatment | Supportive; ICP control; no specific therapy |
| Key clue | Neurological deficit disproportionate to CT findings |
Sources: Robbins Pathologic Basis of Disease | Grainger & Allison's Diagnostic Radiology | Harrison's Principles of Internal Medicine 22E | Sabiston Textbook of Surgery | Tintinalli's Emergency Medicine | Plum & Posner's Diagnosis and Treatment of Stupor and Coma | Fischer's Mastery of Surgery 8e | Mulholland and Greenfield's Surgery 7e
Recent evidence note: A 2025 meta-analysis (Sanker et al., J Neurotrauma, PMID: 40485292) on DAI frequency and outcomes in severe TBI is the latest systematic review - check it for updated incidence and mortality figures.
This is a shared conversation. Sign in to Orris to start your own chat.