Juvenile onset recurrent respiratory papillomatosis in detail
Reading File
Finding Sources
Finding Sources
Searching PubMed
"recurrent respiratory papillomatosis" juvenile onset
Searching the Web
juvenile onset recurrent respiratory papillomatosis HPV treatment management 2024 2025
Reading File
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC11088349
Searching Images
recurrent respiratory papillomatosis laryngeal papilloma
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have comprehensive information from all sources. Let me compile the detailed answer.
Juvenile-Onset Recurrent Respiratory Papillomatosis (JORRP)
Definition
Juvenile-onset recurrent respiratory papillomatosis (JORRP) — also called juvenile laryngeal papillomatosis — is a chronic, recurrent benign neoplastic disease of the aerodigestive tract caused by Human Papillomavirus (HPV), predominantly types 6 and 11. It is characterized by the recurrent growth of exophytic squamous papillomas predominantly at epithelial junction zones throughout the respiratory tract, most severely in the larynx. It represents the most common benign laryngeal tumor in children.
Epidemiology
| Parameter | Value |
|---|---|
| Incidence (children) | 0.24–4.3 per 100,000 children |
| Prevalence (children) | ~1.11 per 100,000 |
| Median age at diagnosis | 4.4 years |
| Sex ratio | Approximately 1:1 |
| Disease course | Bimodal — juvenile peak (<5 years), adult peak (20–40 years) |
-
Two distinct age peaks exist: the juvenile form (onset <5 years) and the adult form (20–40 years). The juvenile form is more aggressive.
-
Rare but impactful: although uncommon, the disease burden per patient is immense — over 100 surgical procedures may be required during a child's lifetime.
-
Following widespread HPV vaccination, a significant decline in JORRP incidence has been documented in countries with national vaccination programs (2025 systematic review, PMID 39611396).
-
Cummings Otolaryngology Head and Neck Surgery, p. 1131
Etiology and Virology
- HPV subtypes 6 and 11 account for the vast majority of cases.
- HPV-11 is associated with:
- More aggressive disease
- More frequent surgical interventions
- Higher risk of tracheopulmonary spread
- HPV-16 and -18 are occasionally found and carry higher risk of malignant transformation to squamous cell carcinoma.
- Transmission occurs via the birth canal from a mother with genital condylomata; however:
- Only ~1 in 400 exposed children actually develop RRP (low infectivity)
- 7 per 1,000 births to genitally infected mothers develop RRP
- Cesarean section is NOT reliably protective — its use in this context remains controversial.
- Germline transmission from parents with RRP to children appears rare.
Pathology and Histology
Papillomas arise preferentially at squamociliary junctions — zones where respiratory columnar epithelium transitions to squamous epithelium:
| Site | Frequency |
|---|---|
| Larynx | 97.9% (primary site) |
| Trachea | 10.9% |
| Soft palate | 10.3% |
| Bronchi | Variable (distal spread) |
Histologic features:
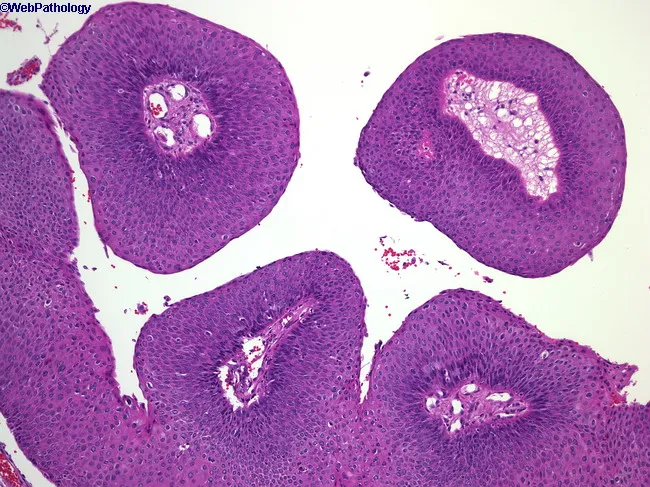
- Exophytic, papillary fronds with fibrovascular cores
- Acanthosis — thickened stratified squamous epithelium
- Koilocytes — pathognomonic HPV-infected cells with perinuclear halos and irregular nuclei in the superficial layers
- No invasion of the underlying basement membrane (distinguishes from carcinoma)
- Focal parakeratosis
Clinical Presentation
Primary symptoms in children:
- Hoarseness — most common initial symptom (voice change)
- Stridor — inspiratory, from laryngeal obstruction
- Dyspnea, respiratory distress
- Recurrent croup-like episodes — leading to frequent misdiagnosis as asthma or reflux
- Chronic cough, feeding difficulties
Important distinction: Adults present primarily with dysphonia; children are more likely to present with dyspnea due to the smaller airway diameter and greater risk of critical obstruction.
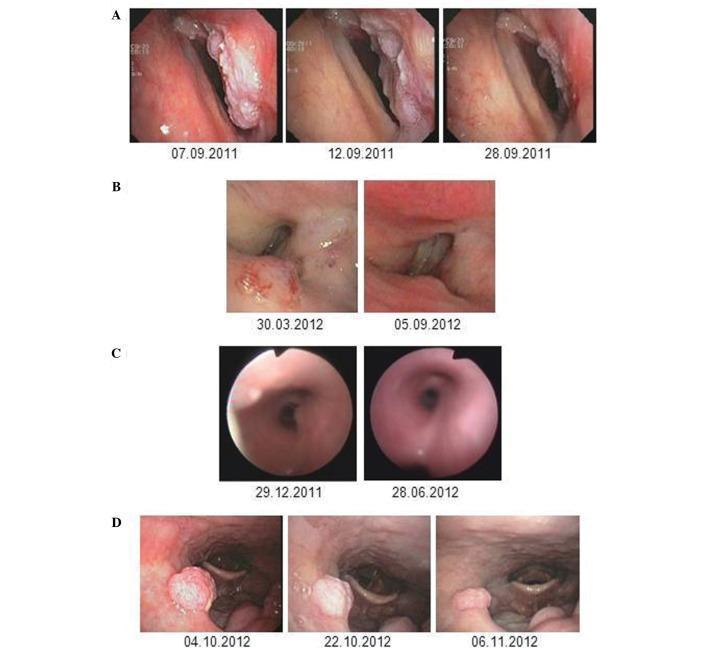
Endoscopic Appearance

Fig. A: Papilloma at posterior vocal fold. B: Normal appearance 2 weeks post-removal with cidofovir injection. — Cummings Otolaryngology, p. 1131
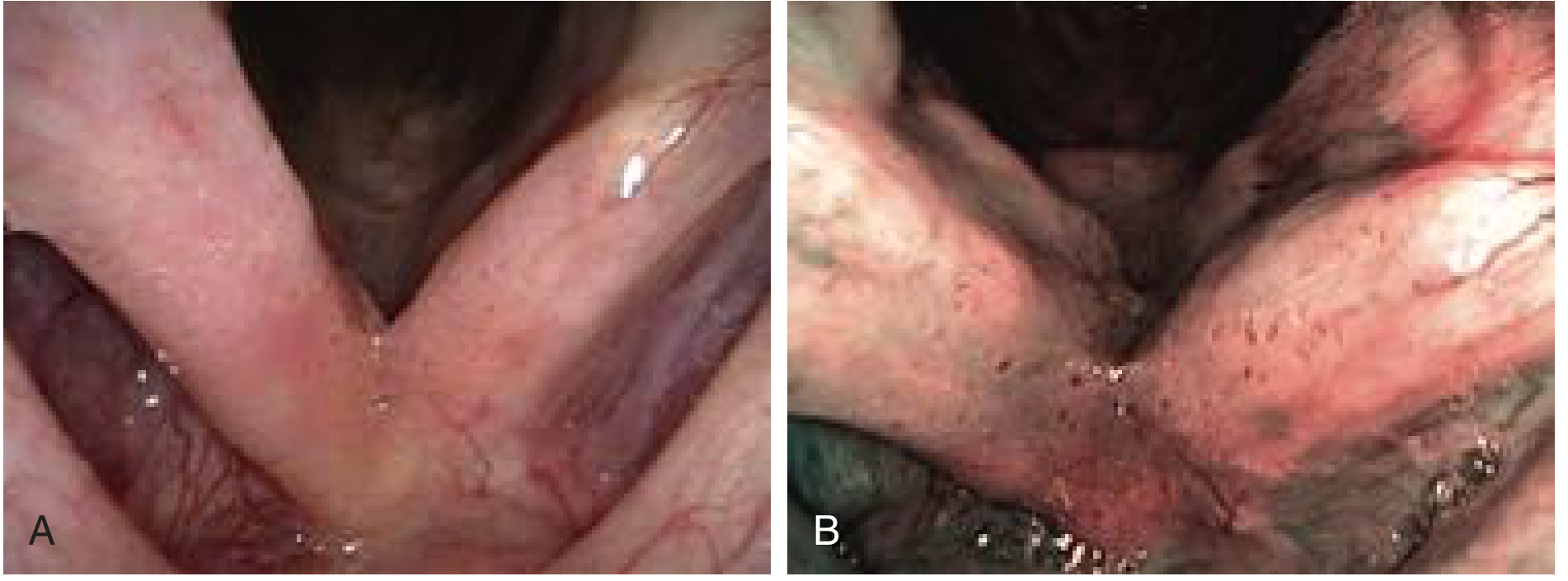
Fig. Carpet variant RRP under standard (A) and narrow-band (B) light. — Cummings Otolaryngology, p. 1131
Morphologic patterns:
- Classic exophytic — cauliflower-like, friable, white-pink irregular masses, sessile or pedunculated
- Carpet variant — velvety, flat growth with stippled red dots (fibrovascular cores); frequently misdiagnosed as acid reflux; more common in adults

Staging and Severity Assessment
Derkay–Coltrera Scoring System — the standard clinical staging tool:
- Grades extent of papillomatosis at defined anatomic subsites throughout the aerodigestive tract
- Enables objective monitoring of disease progression over time
- Guides surgical planning and communication between clinicians
Aggressive disease (Derkay definition): >4 surgical interventions per year
Risk factors for aggressive course:
- Early age at onset (strongest predictor — more important than HPV type alone)
- HPV-11 positivity
- Low socioeconomic status
- Maternal condyloma history during pregnancy
- High number of prior surgeries (positively correlated with tracheal spread)
Distal Spread
Tracheopulmonary extension is a feared complication, seen particularly with HPV-11:
- Correlated with: tracheotomy history, high surgical frequency, long disease duration
- Chest CT at diagnosis is recommended; repeat every 5 years if initial scan is normal and no bronchial progression
- Pulmonary involvement can cause cystic changes, pneumonia, respiratory failure
Management
1. Surgical — Gold Standard
The cornerstone of JORRP management is repeated endoscopic surgical debulking under general anesthesia. The goal is disease control, not cure, preserving airway patency and voice quality.
| Technique | Features |
|---|---|
| CO₂ laser | Most widely accepted; hemostatic; precise plane-by-plane vaporization; protects underlying vocal fold |
| Microdebrider (laryngeal shaver) | Increasingly preferred; reduces OR time, mucosal injury, cost; improves voice outcomes; avoids laser risks |
| Cold steel instruments | Used in some centers based on preference |
| Radiofrequency/coblation | Alternative option |
Key principles:
- Do NOT strip both vocal folds simultaneously — avoids anterior commissure scarring
- Tracheotomy is discouraged: promotes distal spread, should be avoided if possible
- Children may require >100 surgeries over childhood; some require procedures every few weeks
2. Adjuvant Medical Therapies
No adjuvant therapy is curative; all are used to reduce surgical frequency.
Cidofovir (intralesional)
- Cytosine nucleoside analogue antiviral
- Most strongly supported by systematic reviews of English literature
- Injected intralesionally at time of surgery
- Reduces recurrence interval; well-studied in pediatric series
- Concerns regarding potential carcinogenicity at high doses
Interferon (alpha)
- Dramatic responses in some patients; limited long-term role
- Papillomas tend to regrow on cessation
- Higher doses/longer duration → higher response rate (Leventhal criteria)
- ~25% achieve long-term remission; most have reduced growth rate
- Used when disease is severe and refractory to surgical control alone
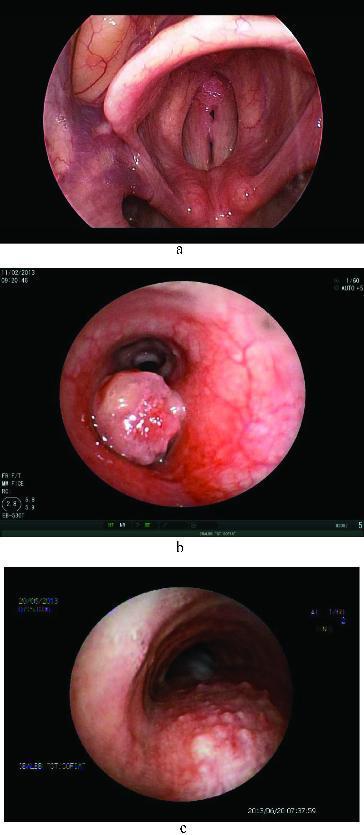
Bevacizumab (systemic)
- Anti-VEGF (vascular endothelial growth factor) monoclonal antibody
- Shown promise in aggressive cases, particularly with tracheopulmonary spread
- Image below shows regression of laryngeal and endobronchial papillomas after systemic bevacizumab therapy
Indole-3-Carbinol
- Natural derivative from cruciferous vegetables (broccoli, cabbage)
- Anecdotal evidence of benefit; likely more effective in rapidly growing disease
- Some authors report disappointing results
Methotrexate
- Used in refractory cases not responding to interferon or cis-retinoic acid
- Prolonged inter-surgical interval and reduced disease severity reported; no complete regression
HPV Vaccine (Gardasil / Gardasil 9) — Adjuvant Use
- Multiple studies support HPV vaccination as adjuvant treatment in JORRP
- Mechanism unclear (prophylactic vaccine used therapeutically) — likely prevents reinfection after surgical removal
- 2022 systematic review supports potential benefit in reducing recurrence
- 2024 retrospective cohort (19-year data) continues to show benefit in prolonging surgical intervals
- Recommended by international IPOG (International Pediatric Otolaryngology Group) consensus
Photodynamic therapy / Cryotherapy / Irradiation
- Not validated; some are rejected; remain experimental
3. Emerging Therapies (2025)
Zopapogene imadenovec (Papzimeos) — FDA approved August 2025:
- First FDA-approved treatment specifically for RRP
- Off-the-shelf AdenoVerse gene therapy designed to elicit HPV-6/11-specific immune responses
- ~50% of treated adults required no additional surgeries over the following year with durable benefit
INO-3107 (INOVIO):
- DNA immunotherapy (DNA medicine) targeting HPV-6/11
- BLA rolling submission completed November 2025; under FDA Accelerated Approval review
Tracheotomy — Special Consideration
- Strongly discouraged in JORRP
- History of tracheotomy correlates with: more frequent surgeries, increased tracheal involvement, and worse outcome
- If unavoidable (critical airway obstruction not manageable otherwise), it becomes a last resort
- Promotes distal papilloma seeding along the tracheobronchial tree
Malignant Transformation
- Rare but recognized — occurs in ~1–4% of RRP cases
- Risk factors:
- HPV-16 or HPV-18 (vs. 6/11)
- Prior irradiation (historically used, now contraindicated)
- Tobacco use
- Immunosuppression
- Results in squamous cell carcinoma of the larynx, trachea, or lung
Prevention — HPV Vaccination
A 2025 systematic review (PMID 39611396) confirms that national HPV vaccination programs have produced significant declines in JORRP incidence. Since JORRP is acquired perinatally from maternal genital HPV infection:
- Vaccinating women of reproductive age with Gardasil 9 before first sexual exposure prevents vertical transmission
- U.S. data from 2015–2020 show meaningful reductions in new JORRP cases following vaccine introduction
- Prevention remains the most powerful intervention available
Prognosis and Natural History
| Outcome | Description |
|---|---|
| Spontaneous remission | Possible but unpredictable; more common at puberty |
| Aggressive/chronic course | Most children require repeated lifetime surgeries |
| Pulmonary spread | Worsens prognosis significantly |
| Malignant transformation | Rare; usually fatal |
| Psychological burden | Profound; impacts speech, schooling, quality of life |
The clinical course is highly variable. Early age of onset is the strongest predictor of a more aggressive, refractory course — more influential than HPV type alone. Patients with onset before age 3 typically require more frequent operations and are at higher risk for distal spread.
Summary of Key Points
| Feature | Detail |
|---|---|
| Causative agent | HPV-6 (majority), HPV-11 (aggressive), HPV-16/18 (malignant risk) |
| Primary site | Larynx (97.9%), especially vocal folds and subglottis |
| Age of onset (juvenile) | Peak < 5 years; median ~4.4 years |
| Transmission | Vertical (birth canal); cesarean not reliably protective |
| Hallmark symptom | Hoarseness + stridor in children |
| Histology | Koilocytes, papillary fronds, fibrovascular cores; no invasion |
| Staging | Derkay–Coltrera score |
| Gold standard treatment | Repeated endoscopic surgical debulking (CO₂ laser or microdebrider) |
| Best-supported adjuvant | Intralesional cidofovir |
| New FDA-approved therapy | Zopapogene imadenovec (Papzimeos) — August 2025 |
| Prevention | HPV vaccination (Gardasil 9) |
| Feared complication | Tracheopulmonary spread; malignant transformation |
Sources:
- Cummings Otolaryngology Head and Neck Surgery, Chapter 60, pp. 1131–1133
- "Juvenile onset recurrent respiratory papillomatosis: What do we know in 2024?" PMC11088349
- Chinese guideline for the diagnosis and treatment of JORRP (2024) PMC11998182
- Jacobsen et al., Acta Otolaryngol 2025 — HPV vaccination and declining JORRP incidence (PMID 39611396)
- Ovcinnikova et al., Respir Res 2024 — Systematic review of epidemiology and burden (PMID 39696284)
- RRPF Research News (FDA approval of Papzimeos, August 2025)
This is a shared conversation. Sign in to Orris to start your own chat.