Aortic stenosis for anaesthesiologist explain in detail
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Searching PubMed
"aortic stenosis" AND "noncardiac surgery" AND anesthesia
I now have all the content I need to write a comprehensive, well-structured answer. Let me compile it.
Aortic Stenosis for the Anaesthesiologist - A Comprehensive Guide
1. Overview and Epidemiology
Aortic stenosis (AS) is the most common valvular heart disease diagnosed in adults in high-income countries. Approximately 3% of people over the age of 75 have AS, and 12% of these have moderate or severe disease. The prevalence is rising due to an aging population.
Causes by age:
- Congenital bicuspid aortic valve - stenosis typically manifests in the 4th-5th decade of life; occurs in 1-2% of the population
- Senile/calcific degenerative AS - most common cause overall; calcium deposits on normal cusps in patients aged 60+
- Rheumatic AS - less common in developed countries; rarely isolated and usually associated with aortic regurgitation or mitral valve disease
2. Pathophysiology - What the Anaesthesiologist Must Understand
The Fixed Obstruction
Normal aortic valve area (AVA): 2.5-3.5 cm²
| Severity | AVA | Mean Gradient |
|---|---|---|
| Mild | 1.5 - 2.0 cm² | < 20 mmHg |
| Moderate | 1.0 - 1.5 cm² | 20-40 mmHg |
| Severe | < 1.0 cm² | > 40 mmHg |
| Critical | 0.5 - 0.7 cm² | ~50 mmHg at rest |
Pressure-Volume Loop in AS
The blue loop (below) is AS vs the orange normal loop - note the markedly elevated LV systolic pressure required to maintain stroke volume across the narrowed valve:
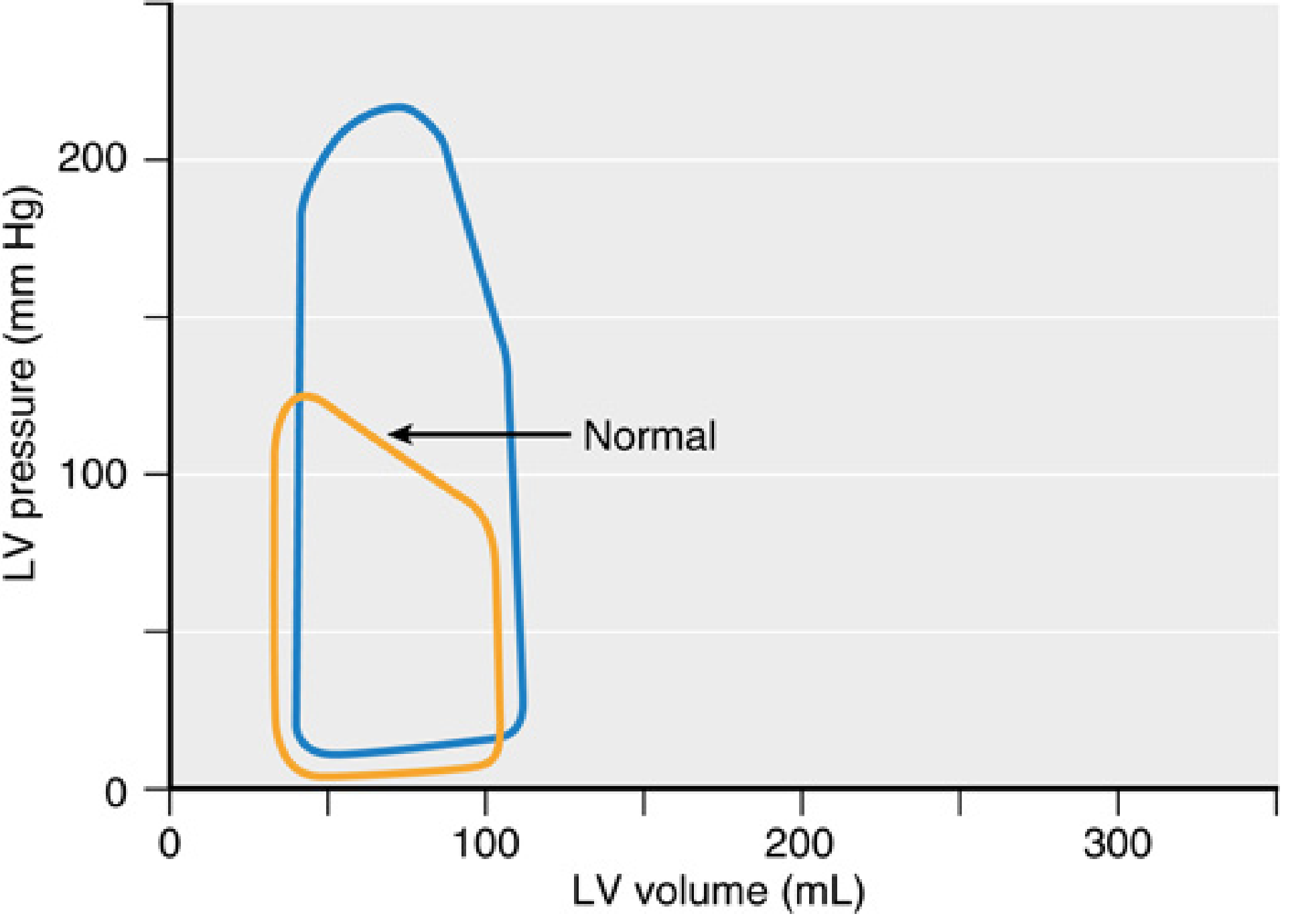
Fig. Pressure-volume loop in AS (blue) vs normal (orange). Note the much higher peak systolic LV pressure with preserved LV volume. - Miller's Anesthesia, 10e
Compensatory Mechanisms and Their Limits
- Concentric LV hypertrophy - parallel replication of sarcomeres maintains stroke volume by generating the needed transvalvular pressure gradient. LV can generate systolic pressures up to 300 mmHg.
- Increased LVEDP - despite normal LVEDV until late disease, end-diastolic pressure is elevated early due to reduced compliance from hypertrophy and fibrosis.
- Diastolic dysfunction - impaired LV filling; ventricular filling becomes critically dependent on atrial systole (the "atrial kick" may contribute up to 40% of total cardiac output in AS).
The Pathophysiologic Triad (End-Stage)
The classic clinical triad of advanced AS:
- Angina - myocardial oxygen demand increases (hypertrophy) while supply decreases (compressed intramyocardial vessels from high intracavitary pressures)
- Syncope - inability to increase CO during exertion + vasodilation in exercising muscle; arrhythmias
- Heart failure / dyspnoea - elevated LVEDP backs up into pulmonary vasculature
Prognosis once symptomatic (without valve replacement):
- Angina: ~5 years survival
- Syncope: ~3 years survival
- Heart failure: ~1-2 years survival
Key Anaesthetic Implications of Pathophysiology
| Pathophysiologic Feature | Anaesthetic Consequence |
|---|---|
| Fixed LVOT obstruction | Cannot increase CO across the valve - output is rate-dependent |
| Concentric hypertrophy + diastolic dysfunction | Extremely preload-sensitive; intolerant of volume shifts |
| Dependent on atrial contraction | AF or junctional rhythm = precipitous drop in CO |
| Impaired coronary perfusion | Myocardial ischaemia possible even without CAD; coronary perfusion pressure must be protected |
| Reduced LV compliance | Small changes in filling pressure cause large changes in CO |
3. Preoperative Assessment
Clinical Evaluation
- Symptoms: exertional dyspnoea, angina, syncope, or near-syncope
- Signs: slow-rising, low-amplitude (pulsus parvus et tardus) carotid pulse; harsh late-peaking systolic ejection murmur best heard at right upper sternal border, radiating to carotids; absent A2; paradoxically split S2
- ECG: LV hypertrophy with strain pattern, left axis deviation, left bundle branch block
- Echocardiography: mandatory - confirms AVA, mean gradient, peak jet velocity, LV function, concurrent valve lesions
Risk Stratification for Non-Cardiac Surgery
Per current guidelines (ACC/AHA):
- Asymptomatic severe AS + preserved EF: noncardiac surgery can proceed with acceptable risk with appropriate haemodynamic monitoring
- Symptomatic severe AS: aortic valve replacement (surgical or TAVR) should be considered before elective noncardiac surgery
- Asymptomatic AS + EF < 50% undergoing high-risk surgery: European guidelines recommend prior valve replacement
- High-risk patients ineligible for replacement: percutaneous balloon aortic valvuloplasty may be considered as a bridge
A 2026 systematic review and meta-analysis in Anaesthesia (PMID: 41388337) provides the most current evidence on peri-operative risk in AS patients undergoing non-cardiac surgery.
Acquired von Willebrand Syndrome
An often-overlooked association: moderate-severe AS is associated with acquired von Willebrand syndrome in 67-92% of patients. The mechanism is mechanical disruption of high-molecular-weight von Willebrand multimers by turbulent flow through the narrowed valve. This increases bleeding risk and is relevant before neuraxial or invasive techniques.
4. Haemodynamic Goals - The Core of AS Anaesthesia
This is the most important table for any anaesthesiologist managing AS:
| Parameter | Goal | Rationale |
|---|---|---|
| Preload | Maintain or increase | Hypertrophied, stiff LV needs adequate filling pressure; any reduction in preload = precipitous fall in CO |
| Afterload | Maintain or increase | Vasodilation decreases coronary perfusion pressure and cannot be compensated by increased flow across the fixed valve |
| Heart Rate | 60-90 bpm (normal) | Tachycardia shortens diastolic filling and increases myocardial O₂ demand; extreme bradycardia (<50) reduces CO in a rate-dependent ventricle |
| Rhythm | Sinus rhythm | Loss of atrial kick can precipitate acute decompensation; AF with rapid ventricular response is an emergency - cardiovert immediately |
| Contractility | Maintain | Preserved early; depressed in late/end-stage AS; avoid myocardial depressants where possible |
| MVO₂ | Minimise | Avoid tachycardia; treat hypotension immediately to maintain subendocardial perfusion |
5. Monitoring
Minimum Monitoring
- Standard ASA/international monitors (SpO₂, ECG, NIBP)
- Note: ST-segment and T-wave changes on ECG may be baseline abnormalities from LV hypertrophy, complicating ischaemia detection
Strongly Recommended / Often Mandatory
- Pre-induction invasive arterial line (radial): essential in severe AS. Pulse pressure is typically narrowed (may be ≤50 mmHg despite normal LVEF). Even brief hypotension is poorly tolerated. Allows beat-to-beat monitoring and facilitates vasopressor titration.
- Transesophageal echocardiography (TEE): gold standard for intraoperative monitoring. Assesses:
- LV preload (LVEDA)
- LV contractility and wall motion abnormalities
- Valvular function and gradient
- Haemodynamic response to interventions
- Best views: midesophageal aortic valve short-axis and transgastric long-axis for Doppler gradients
TEE Views for Aortic Valve Assessment
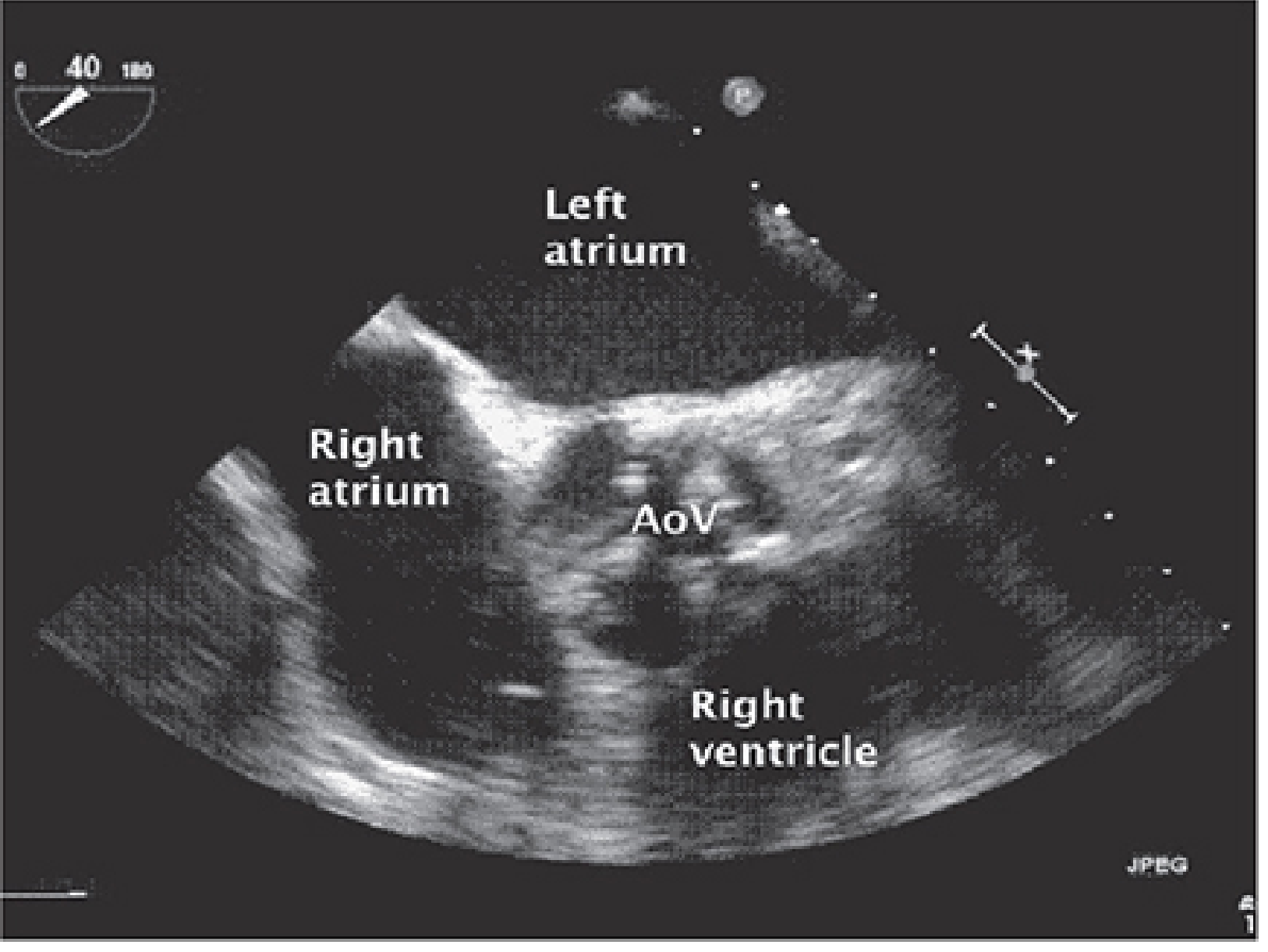
Fig. Midesophageal short-axis aortic valve TEE view showing LA, RA, RV, and the AoV - Morgan & Mikhail's Clinical Anesthesiology, 7e
PA Catheter
- Rarely required in patients with preserved ventricular function
- Risk: arrhythmias during insertion can severely compromise coronary perfusion in AS; CPR is ineffective across a stenotic valve
- Consider only in selected patients with severely impaired LV function
6. Anaesthetic Technique
General Anaesthesia
Induction:
- Use dose-reduced agents - virtually all induction agents produce vasodilation and hypotension
- Preferred agents: etomidate (minimal haemodynamic effects) or a carefully titrated ketamine (maintains SVR)
- Slow, controlled induction with vasopressor (phenylephrine) immediately available
- Phenylephrine is the vasopressor of choice for acute hypotension in AS:
- Pure alpha-agonist increases SVR/diastolic BP without increasing heart rate (unlike ephedrine, which causes tachycardia)
- Restores coronary perfusion pressure across the fixed obstruction
- Vasopressin and norepinephrine are alternative options
Maintenance:
- Volatile agents: use with caution - concentration-dependent vasodilation, myocardial depression, and potential loss of sinus rhythm
- Keep concentrations low; supplement with opioids/neuraxial techniques where appropriate
- Tachycardia (e.g., from laryngoscopy) should be treated immediately with beta-blockade (esmolol) or deepening anaesthesia
- Significant hypertension should also be treated promptly as it increases myocardial O₂ demand
- SVT with haemodynamic compromise: immediate synchronised cardioversion
Vasopressors:
- Norepinephrine, vasopressin, and phenylephrine are preferred over ephedrine (which causes tachycardia)
- Vasodilators (GTN, SNP) should be used with extreme caution or avoided - these patients are very sensitive to afterload reduction
Regional Anaesthesia (Neuraxial)
- Mild-moderate AS (generally asymptomatic): may tolerate spinal or epidural anaesthesia
- Severe AS: neuraxial blockade is a relative contraindication but not absolute - decision must be individualised based on disease severity, LV function, and case urgency
- Epidural preferred over single-shot spinal because:
- Slower, more titratable onset of sympatholysis
- Allows more timely correction of hypotension
- Continuous spinal catheters offer a similar advantage
- A vasopressor must be immediately available for any neuraxial technique in AS
- The acquired von Willebrand syndrome in these patients should be excluded/managed before neuraxial blockade
7. Specific Perioperative Scenarios
Cardiac Surgery - Aortic Valve Replacement (AVR)
Premedication: anxiolysis to avoid tachycardia and reduce sympathetic stress (carefully titrated benzodiazepine)
Pre-induction: place arterial line before induction in severe AS
TEE: mandatory for:
- Baseline valve assessment and LV function
- Annulus measurement for valve sizing (critical to avoid patient-prosthesis mismatch)
- Post-bypass assessment of valve function, paravalvular regurgitation, and biventricular function
Post-bypass considerations:
- After relieving the obstruction, LV may develop "suicide ventricle" (LVOTO from hypertrophy becoming dynamic) - diagnose with TEE and treat with volume and vasoconstrictors
- Watch for new conduction defects post-AVR
TAVR (Transcatheter Aortic Valve Replacement)
TAVR was first approved in Europe in 2007 and the US in 2011. It has expanded from extreme/high-risk to intermediate-risk patients.
Anaesthesia for TAVR:
- Originally performed under GA with TEE guidance
- Trend toward monitored anaesthesia care (MAC) or moderate sedation with TTE monitoring, which improves efficiency without compromising safety
- GA with TEE is still preferred for:
- High risk of coronary occlusion
- Risk of annular rupture
- Reducing contrast load in high-risk patients
- Secondary valve sizing measurements
- Valve sizing: multidetector CT (MDCT) is the preferred modality; 2D TEE/TTE underestimates annular size due to the elliptical shape of the aortic valve complex; 3D TEE is more accurate
- Intraprocedural TEE monitoring: baseline biventricular function, wire and device positioning, post-deployment assessment of transvalvular gradients and paravalvular regurgitation, and immediate recognition of complications (coronary obstruction, pericardial effusion, new RWMA, aortic injury)
8. Critical Intraoperative Events and Management
| Event | Management |
|---|---|
| Acute hypotension | Phenylephrine/vasopressin bolus; volume if preload reduced; identify and treat cause |
| AF with rapid ventricular response | Immediate synchronised cardioversion (DO NOT rate-control first - loss of atrial kick is too dangerous) |
| Other SVT with haemodynamic compromise | Immediate synchronised cardioversion |
| Bradycardia < 50 bpm | Atropine/pacing; this is poorly tolerated as CO becomes rate-dependent |
| Frequent VEAs / VT | Usually reflects ischaemia; treat haemodynamically (vasopressors to restore CPP) and pharmacologically |
| Ischaemia | Restore CPP with vasopressors; consider GTN with extreme caution; consult immediately |
| Cardiac arrest | Extremely high mortality; CPR does not generate effective CO across the stenotic valve |
9. Summary: The "4 DON'Ts" in AS Anaesthesia
- Don't vasodilate - drop in SVR cannot be compensated; immediate coronary underperfusion
- Don't allow tachycardia - reduces diastolic filling time and increases MVO₂ in an already oxygen-starved myocardium
- Don't lose sinus rhythm - atrial kick contributes up to 40% of CO; loss is an emergency
- Don't hypovolaemia - stiff, non-compliant LV requires adequate preload; small volume changes cause large haemodynamic shifts
Sources
- Morgan & Mikhail's Clinical Anesthesiology, 7e, Ch. 21 (Valvular Heart Disease), pp. 768-771
- Miller's Anesthesia, 10e, Ch. 50 (Valvular Heart Disease) and Ch. 28 (Preoperative Assessment), pp. 3907-3909, 7649-7656
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e, Ch. 39 (Valvular Heart Disease), pp. 3307-3310
- Place A et al. "Peri-operative risk of non-cardiac surgery in patients with aortic stenosis: a systematic review and meta-analysis." Anaesthesia. 2026 Apr. PMID: 41388337
This is a shared conversation. Sign in to Orris to start your own chat.