Benign prostatic hyperplasia
Reading File
Finding Sources
Searching PubMed
"benign prostatic hyperplasia"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive, high-quality information from multiple authoritative textbooks. Here is a complete overview of BPH:
Benign Prostatic Hyperplasia (BPH)
Definition & Epidemiology
BPH is a benign proliferation of stromal and epithelial cells within the prostate gland, centered in the transition zone (periurethral region). It is the most common benign prostatic disease in men over 50.
-
Histologic BPH develops in ~50% of men over 50 years, rising to ~90% by the 8th decade
-
Of those with histologic BPH, approximately 50% develop notable lower urinary tract symptoms (LUTS)
-
Normal prostate volume: ~20 mL in young men; BPH is defined as volume >30 mL
-
Average volume increases from ~24 mL to ~38 mL between ages 50-80
-
Goldman-Cecil Medicine, p. 1316
-
Robbins & Kumar Basic Pathology, p. 659
Pathogenesis
The central driver is androgen-dependent overgrowth of stromal and glandular elements:
- Dihydrotestosterone (DHT) is the key mediator - it is 10 times more potent than testosterone
- Testosterone is converted to DHT in the prostate by 5α-reductase type 2
- DHT binds nuclear androgen receptors, upregulating genes that support cell growth and survival
- DHT-induced growth factors increase stromal cell proliferation and decrease epithelial cell apoptosis
- With aging, testosterone declines but estrogen levels remain elevated (due to peripheral conversion); estrogens act synergistically with DHT via estrogen receptors on both epithelial and stromal cells
- BPH does NOT occur in men castrated before puberty or in those with genetic defects in androgen activity
Obstruction occurs via two mechanisms:
-
Static component: physical compression of the urethra by enlarged gland
-
Dynamic component: increased smooth muscle tone in prostate stroma (alpha-1 adrenergic mediated)
-
Robbins & Kumar Basic Pathology, p. 659
-
Goldman-Cecil Medicine, p. 1316
Morphology
- Prostate weight increases 3- to 5-fold (60-100 g or more)
- BPH affects the transition zone, compressing the urethra to a slit-like orifice
- Cut section shows hyperplastic nodules (variable in color/consistency)
- Nodules may be solid or contain cystic spaces (dilated glands)
- Microscopically: variable proportions of glandular elements and fibromuscular stroma
- Hyperplastic glands lined by two cell layers: tall columnar inner cells + flattened basal cells (this two-layer pattern distinguishes BPH from carcinoma)
- Glandular lumina may contain corpora amylacea (laminated proteinaceous secretions)
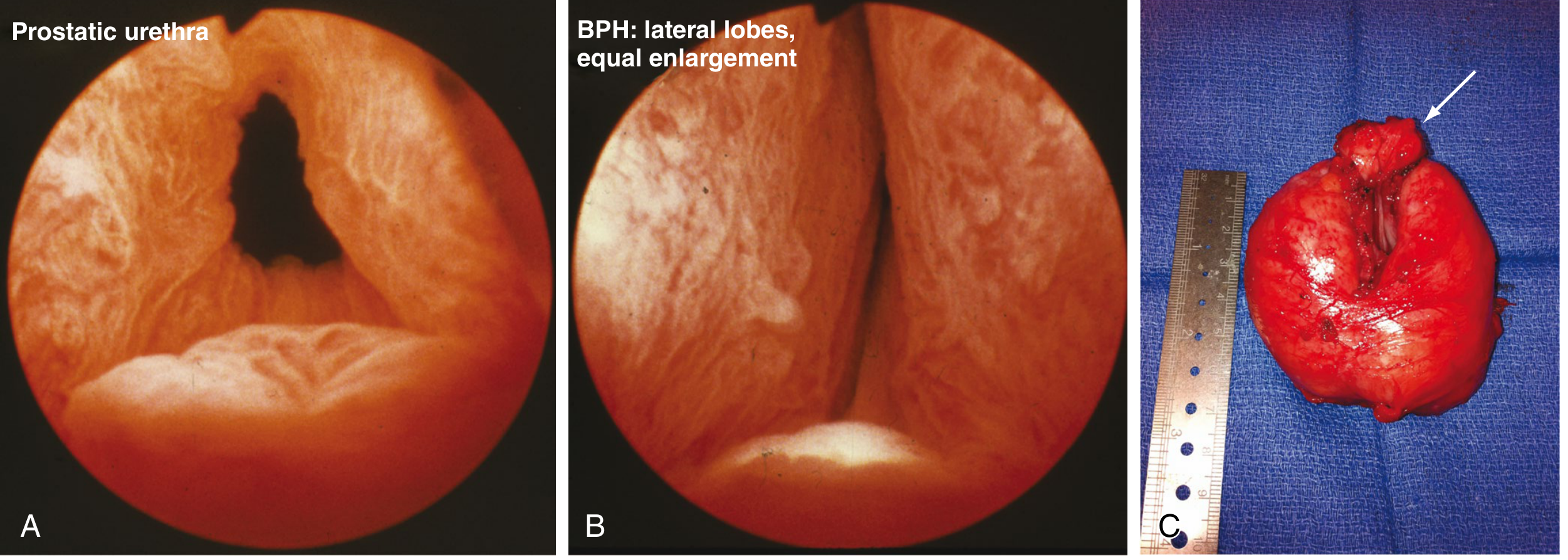
Cystoscopic and gross appearance of BPH (Sabiston Textbook of Surgery):
Clinical Features / LUTS
LUTS from BPH are categorized into three groups:
| Category | Symptoms |
|---|---|
| Voiding (obstructive) | Hesitancy, weak/intermittent stream, straining, prolonged voiding |
| Storage (irritative) | Frequency, urgency, nocturia, urge incontinence |
| Post-void | Incomplete emptying, dribbling, high post-void residual |
Important: There is little correlation between prostate volume and symptom severity, and bladder outlet obstruction severity does not necessarily correlate with LUTS severity.
Chronic obstruction can lead to:
- Recurrent UTIs
- Bladder calculi
- Hydronephrosis / azotemia (renal impairment)
- Acute urinary retention
- Bladder detrusor dysfunction (overactive or underactive bladder)
Diagnosis / Evaluation
| Test | Purpose |
|---|---|
| History + IPSS (International Prostate Symptom Score) | Quantify symptom burden |
| Digital rectal examination (DRE) | Estimate prostate size; assess for nodules (to rule out cancer) |
| Urinalysis | Rule out infection, hematuria |
| PSA | If life expectancy >10 years (controversial for screening) |
| Post-void residual (PVR) | Assess bladder emptying |
| Uroflowmetry | Measure flow rate |
| Cystoscopy / urodynamic studies | Selected cases with diagnostic uncertainty |
Management
Behavioral & Dietary Modifications (First-line for all patients)
- Reduce evening fluid intake, caffeine, alcohol
- Timed voiding, bladder training
- Treat contributing medications (e.g., anticholinergics, diuretics)
Medical Therapy
| Drug Class | Mechanism | Examples | Key Side Effects |
|---|---|---|---|
| Alpha-1 blockers | Relax smooth muscle in bladder neck and prostate; reduce outflow resistance | Tamsulosin, silodosin, alfuzosin, terazosin | Orthostatic hypotension, retrograde ejaculation, rhinitis |
| 5α-reductase inhibitors (5-ARIs) | Block testosterone → DHT conversion; reduce prostate volume (~20-30% reduction) | Finasteride, dutasteride | Reduced libido, erectile dysfunction; reduce serum PSA ~50% |
| Combination therapy | Alpha-blocker + 5-ARI | Tamsulosin + dutasteride | Superior outcomes vs. monotherapy; greater side effects |
| Anticholinergics / Beta-3 agonists | Target overactive bladder component | Solifenacin, mirabegron | Used when storage symptoms predominate |
| PDE-5 inhibitors | Also relax prostate smooth muscle | Tadalafil | Erectile dysfunction concurrently treated |
Note on 5-ARIs and PSA: These drugs reduce serum PSA by approximately 50%, which must be accounted for when using PSA to screen for prostate cancer (double the measured PSA value as a correction).
Surgical Indications (Absolute / Objective)
Surgery is indicated when medical therapy fails OR when the following arise:
- Acute urinary retention
- Bladder calculi
- Azotemia (obstructive renal failure)
- Recurrent UTIs
- Recurrent hematuria
Surgical Options
| Procedure | Notes |
|---|---|
| TURP (transurethral resection of the prostate) | Gold standard; bipolar/laser versions reduce risk of dilutional hyponatremia and bleeding |
| HoLEP (Holmium Laser Enucleation) | Effective for large glands; excellent long-term outcomes |
| ThuLEP (Thulium Laser Enucleation) | Similar to HoLEP |
| PVP (Photoselective Vaporization) | Laser vaporization; good for anticoagulated patients |
| Open simple prostatectomy | For very large adenomas (>80-100 g); enucleation of adenoma |
| Minimally invasive (microwave thermotherapy, radiofrequency ablation) | Office-based; inferior long-term outcomes vs. TURP |
TURP complications: Persistent bleeding, dilutional hyponatremia (from glycine irrigation - eliminated with bipolar/laser), UTI, urinary incontinence, urethral stricture.
- Sabiston Textbook of Surgery, p. 2824-2825
- Goldman-Cecil Medicine, p. 1316
Key Distinguishing Points
| Feature | BPH | Prostate Carcinoma |
|---|---|---|
| Zone of origin | Transition zone | Peripheral zone |
| Gland histology | Two cell layers (columnar + basal) | Single cell layer (no basal layer) |
| Obstruction | Common (periurethral location) | Less likely unless advanced |
| Palpation (DRE) | Smooth, firm enlargement | Hard, irregular nodule |
| Metastasis | Never | Common (bone, lymph nodes) |
Sources: Robbins & Kumar Basic Pathology (Robbins Pathology), p. 659; Goldman-Cecil Medicine, p. 1316; Sabiston Textbook of Surgery, p. 2824-2825
Simple language
Benign Prostatic Hyperplasia (BPH) - Simple Explanation
What is it?
BPH means the prostate gland gets bigger as men age. It is not cancer - just extra cells growing in the gland.
The prostate sits just below the bladder and wraps around the urine tube (urethra). When it grows, it squeezes that tube and makes urination difficult.
Who gets it?
- Very common in older men
- 1 in 2 men over age 50 have it
- 9 in 10 men in their 80s have it
Why does it happen?
As men age, a hormone called DHT (made from testosterone) builds up in the prostate and makes cells grow too much. Estrogen levels also rise with age and add to this growth.
Think of it like a donut squeezing a straw - the bigger the donut, the harder it is for urine to flow through.
Symptoms
Trouble urinating (voiding):
- Weak urine stream
- Difficulty starting to urinate
- Stream that stops and starts
Bladder irritation (storage):
- Needing to urinate frequently
- Waking up at night to urinate (nocturia)
- Sudden, urgent need to go
After urinating:
- Feeling like the bladder is never fully empty
- Dribbling at the end
Complications (if untreated)
- Bladder infections (recurring UTIs)
- Bladder stones
- Complete inability to urinate (urinary retention)
- Kidney damage over time
Diagnosis
| Test | Why it's done |
|---|---|
| Symptom score (IPSS questionnaire) | Measures how bad symptoms are |
| Rectal exam (DRE) | Doctor feels the prostate size |
| Urine test | Rules out infection |
| PSA blood test | Rules out prostate cancer |
| Urine flow test | Measures how fast urine flows |
| Post-void residual scan | Checks how much urine is left after urinating |
Treatment
Step 1 - Lifestyle changes (always first)
- Drink less fluid in the evening
- Cut down on coffee and alcohol
- Go to the toilet on a schedule
- Avoid medications that worsen symptoms
Step 2 - Medicines
| Medicine Type | What it does | Common Examples |
|---|---|---|
| Alpha-blockers | Relax the muscle around the prostate - urine flows more easily | Tamsulosin, Alfuzosin |
| 5-alpha reductase inhibitors | Shrink the prostate over several months | Finasteride, Dutasteride |
| Combination | Both medicines together - works better for large prostates | Tamsulosin + Dutasteride |
Step 3 - Surgery (when medicines don't work)
Surgery is also done urgently if the man cannot urinate at all, has repeated infections, or kidney damage.
| Procedure | Simple Explanation |
|---|---|
| TURP (most common) | A telescope is passed through the urine tube; excess prostate tissue is shaved away |
| Laser surgery (HoLEP) | Same idea but uses a laser - less bleeding, good for very large glands |
| Open surgery | Only for very large prostates; gland is removed through a cut in the abdomen |
Key Point to Remember
BPH is not cancer and does not turn into cancer. But both BPH and prostate cancer can exist at the same time, which is why the doctor checks for cancer separately.
This is a shared conversation. Sign in to Orris to start your own chat.