Placental site trophoblastic tumour
Reading File
Finding Sources
Searching PubMed
"placental site trophoblastic tumor"[MeSH Terms]
Reading File
Reading File
Searching PubMed
"placental site trophoblastic tumor" treatment outcomes
Finding Sources
Reading Article
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Finding Sources
I now have comprehensive information from multiple authoritative sources. Let me compile the full, detailed answer.
Placental Site Trophoblastic Tumour (PSTT)
Overview
PSTT is a rare form of gestational trophoblastic neoplasia (GTN), comprising less than 2% of all gestational trophoblastic neoplasms. It is a neoplastic proliferation of extravillous (intermediate) trophoblasts - cells that normally migrate from the cytotrophoblast of the placenta to invade the maternal decidua and myometrium. PSTT occupies a morphological position intermediate between cytotrophoblasts and syncytiotrophoblasts.
- Robbins & Kumar Basic Pathology, p. 620
- Berek & Novak's Gynecology, p. 2507
Cell of Origin
The tumour arises from intermediate trophoblasts (extravillous trophoblasts), which are the same cells responsible for normal implantation. They have features of both cytotrophoblasts and syncytiotrophoblasts but are functionally distinct:
- They produce human placental lactogen (hPL) rather than hCG
- They invade maternal vessels and decidua without the tissue destruction characteristic of choriocarcinoma
- They are typically diploid, often with an XX karyotype
Antecedent Pregnancy
PSTT can follow any type of pregnancy:
- Normal full-term pregnancy (~50% of cases; in the systematic review, 41.3% of fertility-sparing cases)
- Spontaneous abortion (~30%)
- Hydatidiform mole
- Usually presents months to years after the preceding pregnancy
Clinical Features
| Feature | Detail |
|---|---|
| Presentation | Abnormal uterine bleeding, amenorrhea |
| Uterine mass | Polypoid/infiltrative endometrial/myometrial mass |
| hCG level | Low to moderately elevated (not as high as choriocarcinoma) |
| hPL level | Elevated (useful marker) |
| Behaviour | Indolent; tends to remain confined to uterus, metastasises late |
| Metastatic sites | Lungs most common; also liver, brain |
Pathology
Gross
- Presents as a uterine mass, often intramural, infiltrating the myometrium
Histology
The hallmark is infiltration of the myometrium by polygonal mononuclear or binucleated intermediate trophoblasts with abundant cytoplasm. Key histological features:
- Cells splay apart (rather than destroy) smooth muscle fibres as they invade the myometrium
- No chorionic villi
- No biphasic pattern of cytotrophoblast + syncytiotrophoblast (distinguishing it from choriocarcinoma)
- Tumour cells show tropism for maternal vessels, replacing vessel walls
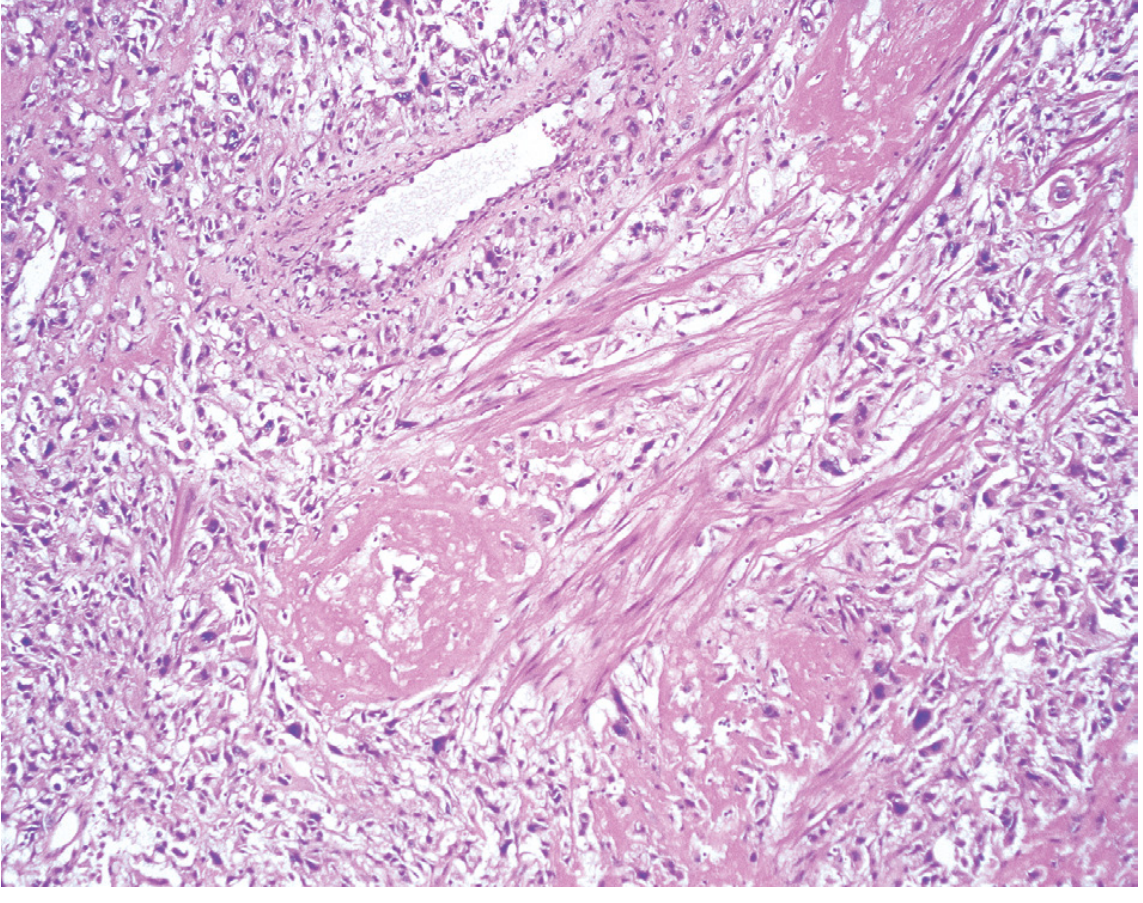
Fig. 22.57 from Robbins, Cotran & Kumar - Placental site trophoblastic tumour. Markedly atypical trophoblasts are seen splaying apart smooth muscle fibres as they invade the myometrium.
Immunohistochemistry
| Marker | PSTT | Choriocarcinoma |
|---|---|---|
| hPL | Strongly positive | Weakly positive |
| hCG | Weakly/focally positive | Strongly positive |
| Cytokeratin | Positive | Positive |
| Mel-CAM (CD146) | Positive | - |
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 958
Comparison with Epithelioid Trophoblastic Tumour (ETT)
Both PSTT and ETT are tumours of intermediate trophoblasts, but differ:
| Feature | PSTT | ETT |
|---|---|---|
| Cell type | Implantation-site intermediate trophoblast | Chorionic-type intermediate trophoblast |
| Location | Endometrium/myometrium | Often cervix or lower uterine segment |
| Growth pattern | Infiltrative, splits myometrial fibres | Discrete nodules, hyaline material |
| Cytoplasm | Abundant eosinophilic | Abundant clear cytoplasm |
| Invasiveness | Overt myometrial invasion | Less overt invasion, but can metastasise |
| Metastases | Lungs, liver | Lungs, bone |
- Berek & Novak's Gynecology, p. 2508
Tumour Markers
- hCG: Only mildly elevated - this is a diagnostic clue. High hCG should raise suspicion for choriocarcinoma instead.
- hPL: Elevated and a more useful marker for PSTT
- Free beta-hCG: Monitoring is still used but hCG levels cannot reliably predict tumour burden or response in PSTT as reliably as in other GTNs
Staging
PSTT uses the standard FIGO staging for GTN:
- Stage I: Confined to uterus
- Stage II: Extends to other genital structures
- Stage III: Lung metastases
- Stage IV: Other distant metastases
The majority of cases at diagnosis are Stage I (~73% in the 2026 systematic review, PMID 40628611).
Prognosis
- Localised disease (Stage I): Excellent prognosis with surgery
- Extrauterine spread: Poor prognosis; 10-15% of patients with disseminated disease die from it
- Interval from antecedent pregnancy to diagnosis >2 years is an adverse prognostic factor
- PSTT has a more indolent course than choriocarcinoma but is far more chemotherapy-resistant
Management
1. Surgery - Primary Treatment
Hysterectomy is the standard treatment for PSTT, especially for women who have completed childbearing:
"Hysterectomy is recommended for placental site trophoblastic tumors for which metastasis is rare." - Schwartz's Principles of Surgery
This contrasts with other GTNs (choriocarcinoma, invasive mole), which are primarily managed with chemotherapy.
2. Fertility-Sparing Treatment
A 2026 systematic review (PMID 40628611) of 63 patients with PSTT undergoing fertility-sparing management found:
- Recurrence rate: 13.8% (8/63 patients) - all treated with hysterectomy after recurrence
- Fertility rate: 36.5% per patient (23 full-term pregnancies reported)
- Mean age: 28.3 years; 73% were Stage I at diagnosis
- Conclusion: Fertility-sparing management is feasible and oncologically safe in selected patients
3. Chemotherapy
- PSTT is relatively insensitive to standard GTN chemotherapy (methotrexate, actinomycin-D)
- For metastatic/high-risk disease, combination regimens are used (EMA-CO or EP-EMA)
- Chemotherapy continues until hCG/hPL normalise, but response rates are lower than in choriocarcinoma
- Surgical resection of chemotherapy-resistant sites may be needed
4. Follow-up
- Surveillance with hCG (and hPL where available) post-treatment
- 12 months of contraception recommended after treatment to allow complete surveillance for relapse
Key Distinguishing Points (PSTT vs Other GTN)
| Feature | PSTT | Choriocarcinoma | Invasive Mole |
|---|---|---|---|
| Cell type | Intermediate trophoblast | Cyto + syncytiotrophoblast | Villous trophoblast |
| hCG | Low | Very high | High |
| hPL | High | Low | Low |
| Chorionic villi | Absent | Absent | Present |
| Chemosensitivity | Poor | Excellent | Good |
| Primary Rx | Surgery | Chemotherapy | Chemotherapy |
| Prognosis (localised) | Good | Excellent (if treated) | Excellent |
Summary Points
- PSTT arises from intermediate (extravillous) trophoblasts and comprises <2% of GTN
- It follows any type of pregnancy, usually presenting months to years later with abnormal bleeding and a mildly elevated hCG
- Histologically: mononuclear/binucleated cells splaying myometrial fibres, no chorionic villi, strong hPL positivity
- Unlike other GTNs, it is not chemosensitive - hysterectomy is the cornerstone of treatment
- Prognosis is good for localised disease, but poor once extrauterine spread occurs
- Fertility-sparing surgery is emerging as a viable option in young women with early-stage disease
Sources:
- Robbins & Kumar Basic Pathology, p. 620
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 958
- Berek & Novak's Gynecology, pp. 2507-2508
- Schwartz's Principles of Surgery, 11th ed.
- Tietz Textbook of Laboratory Medicine, 7th ed., p. 1039
- Fotiou et al. (2026), Int J Gynecol Cancer - Systematic review on fertility-sparing PSTT treatment [PMID: 40628611]
This is a shared conversation. Sign in to Orris to start your own chat.