Describe In Detail About Brachial Plexus Along With Its Clinical Anatomy. 10 mark
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the content needed for a comprehensive, 10-mark answer. Let me compile the full response.
Brachial Plexus — Detailed Description with Clinical Anatomy
1. Introduction
The brachial plexus is a somatic nerve plexus formed by the anterior rami of spinal nerves C5, C6, C7, C8, and most of T1. It originates in the neck, passes laterally and inferiorly over the first rib, and enters the axilla to provide the entire motor and sensory innervation of the upper limb.
— Gray's Anatomy for Students, p. 858
2. Formation and Components
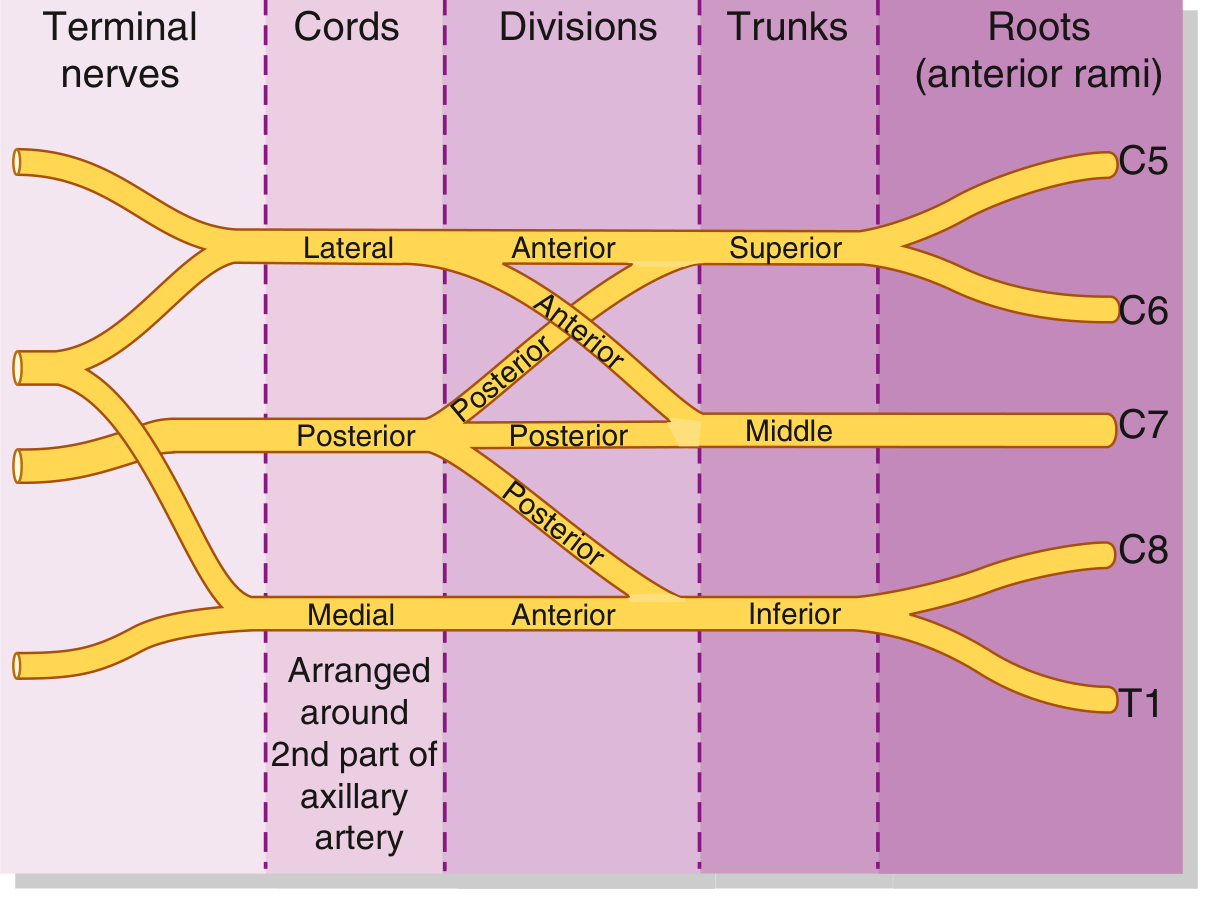
The plexus is organized into five sequential levels: Roots → Trunks → Divisions → Cords → Branches
A useful mnemonic: "Robert Taylor Drinks Cold Beer"

2.1 Roots (Anterior Rami)
- Formed by the anterior rami of C5–C8 and T1
- Emerge between the anterior and middle scalene muscles (interscalene space)
- Receive gray rami communicantes from the cervical sympathetic trunk carrying postganglionic sympathetic fibers
- Lie posterior and superior to the subclavian artery in the posterior triangle of the neck
- Prefixed plexus: C4 contributes; Postfixed plexus: T2 contributes (anatomical variants)
— THIEME Atlas of Anatomy, p. 381
2.2 Trunks
Three trunks cross the base of the posterior triangle above the clavicle:
| Trunk | Root Contributions | Position |
|---|---|---|
| Superior (Upper) | C5 + C6 | Superior in the neck |
| Middle | C7 alone | Intermediate position |
| Inferior (Lower) | C8 + T1 | Lies on rib I, posterior to subclavian artery |
— Gray's Anatomy for Students, p. 858
2.3 Divisions
Each trunk divides into an anterior and posterior division behind the clavicle — giving 6 divisions total.
- Anterior divisions → supply anterior (flexor) compartments
- Posterior divisions → supply posterior (extensor) compartments
- No peripheral nerves arise directly from the divisions
2.4 Cords
The divisions reunite to form three cords, named by their relationship to the second part of the axillary artery:
| Cord | Composition | Position |
|---|---|---|
| Lateral cord | Anterior divisions of upper + middle trunks (C5–C7) | Lateral to axillary artery |
| Medial cord | Anterior division of inferior trunk (C8–T1) | Medial to axillary artery |
| Posterior cord | All three posterior divisions (C5–T1) | Posterior to axillary artery |
— Gray's Anatomy for Students, p. 859
3. Branches of the Brachial Plexus
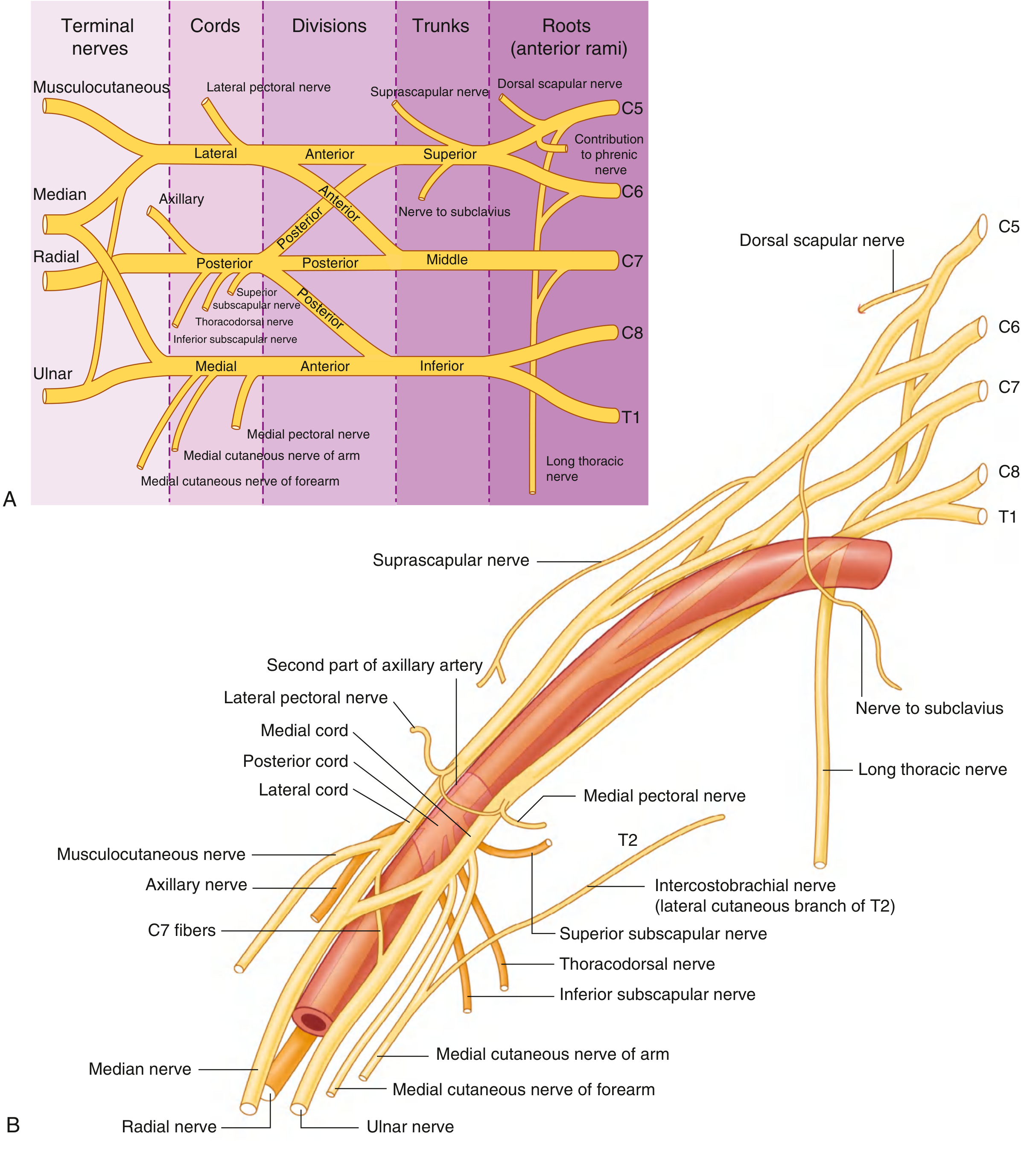
3.1 Branches from the Roots (Supraclavicular)
| Nerve | Origin | Segments | Supplies |
|---|---|---|---|
| Dorsal scapular nerve | C5 root | C4, C5 | Rhomboid major, rhomboid minor, levator scapulae |
| Long thoracic nerve | C5–C7 roots | C5–C7 | Serratus anterior |
| Small muscular branches to neck | C5–C8 | — | Scalenes, longus colli |
| Contribution to phrenic nerve | C5 root | C5 | Diaphragm (partial) |
3.2 Branches from the Trunks (Supraclavicular)
Only the superior trunk gives branches:
| Nerve | Segments | Supplies |
|---|---|---|
| Suprascapular nerve | C5, C6 | Supraspinatus, infraspinatus |
| Nerve to subclavius | C5, C6 | Subclavius |
3.3 Branches from the Lateral Cord (Infraclavicular)
| Nerve | Segments | Motor Supply | Sensory Supply |
|---|---|---|---|
| Lateral pectoral nerve | C5–C7 | Pectoralis major | — |
| Musculocutaneous nerve | C5–C7 | Coracobrachialis, biceps brachii, brachialis | Lateral cutaneous nerve of forearm |
| Lateral root of median nerve | C5–C7 | (contributes to median nerve) | — |
3.4 Branches from the Medial Cord (Infraclavicular)
| Nerve | Segments | Motor / Sensory Supply |
|---|---|---|
| Medial pectoral nerve | C8, T1 | Pectoralis major and minor |
| Medial cutaneous nerve of arm | C8, T1 | Skin of medial arm |
| Medial cutaneous nerve of forearm | C8, T1 | Skin of medial forearm |
| Ulnar nerve | C7–T1 | Intrinsic hand muscles, flexor carpi ulnaris, medial FDP; medial 1½ digits |
| Medial root of median nerve | C8, T1 | (contributes to median nerve) |
3.5 Branches from the Posterior Cord (Infraclavicular)
| Nerve | Segments | Motor / Sensory Supply |
|---|---|---|
| Upper subscapular nerve | C5, C6 | Subscapularis (upper) |
| Thoracodorsal nerve | C6–C8 | Latissimus dorsi |
| Lower subscapular nerve | C5, C6 | Subscapularis (lower), teres major |
| Axillary nerve | C5, C6 | Deltoid, teres minor; skin over deltoid (upper lateral arm) |
| Radial nerve | C5–T1 | All posterior compartment muscles of arm and forearm; skin on posterior arm, forearm, dorsum of hand |
The median nerve is formed by union of the lateral root (from lateral cord) and medial root (from medial cord) — these form an "M" shape over the third part of the axillary artery.
— Gray's Anatomy for Students, p. 865
4. Relations & Surface Anatomy
- In the neck: Roots lie between anterior and middle scalene muscles; trunks are in the posterior triangle
- At the clavicle: Divisions pass posterior to the clavicle and subclavius muscle
- In the axilla: Cords surround the axillary artery — lateral, posterior, and medial cords named accordingly
- The musculocutaneous nerve pierces the coracobrachialis muscle — a useful landmark for cord identification in the axilla
— THIEME Atlas of Anatomy, p. 381
5. Clinical Anatomy
5.1 Erb–Duchenne Palsy (Upper Plexus Injury: C5, C6)
Mechanism: Forced separation of head and shoulder (e.g., shoulder dystocia at birth, motorcycle fall widening the cervicohumeral angle, fall on outstretched hand).
Muscles paralysed: Deltoid, supraspinatus, infraspinatus, biceps brachii, brachioradialis (C5, C6-innervated muscles).
Classic posture — "Waiter's Tip" deformity:
- Arm hangs adducted and medially rotated (deltoid, supraspinatus paralysed)
- Forearm pronated and extended (biceps, brachioradialis paralysed)
- Wrist flexed
Sensory loss: Lateral aspect of arm and forearm (C5, C6 dermatomes)
Reflex loss: Biceps and brachioradialis reflexes absent
Prognosis: Best prognosis of all brachial plexus injuries; >90% recover without surgery.
— Miller's Review of Orthopaedics 9th Ed., p. 260; Bradley & Daroff's Neurology, p. 2870
5.2 Klumpke's Palsy (Lower Plexus Injury: C8, T1)
Mechanism: Forced abduction of the arm above the head (e.g., grasping a branch during a fall, forceps delivery in breech presentation).
Muscles paralysed: Intrinsic hand muscles (interossei, lumbricals, thenar, hypothenar), flexor carpi ulnaris, medial FDP.
Classic posture — "Claw Hand":
- Hyperextension of MCPJs with flexion of IPJs — due to loss of intrinsic hand muscles
- More severe in the ring and little fingers (ulnar paradox not fully applicable here)
Associated finding: If T1 sympathetic fibers are involved → Horner syndrome (ptosis, miosis, anhidrosis, enophthalmos) due to damage to preganglionic sympathetic fibers at T1.
Prognosis: Poor; associated with Horner syndrome carries worst prognosis.
— Miller's Review of Orthopaedics 9th Ed., p. 260; The Harriet Lane Handbook, 23rd Ed.
5.3 Total Brachial Plexus Palsy (C5–T1)
- Complete flaccid paralysis of the entire upper limb ("flail arm")
- Total sensory loss below the shoulder
- Absent all upper limb reflexes
- Horner syndrome present
- Worst prognosis
5.4 Long Thoracic Nerve Injury (C5–C7 roots)
Cause: Axillary lymphadenectomy (breast cancer surgery), heavy backpack, stab wounds.
Result: Serratus anterior paralysis → Winging of scapula (medial border of scapula lifts away from chest wall on pushing against a wall).
— THIEME Atlas of Anatomy, p. 382
5.5 Axillary Nerve Injury (C5, C6 — Posterior cord)
Cause: Fracture of surgical neck of humerus, anterior shoulder dislocation, improper use of crutches.
Result:
- Deltoid paralysis → inability to abduct arm beyond 15° (first 15° by supraspinatus)
- Loss of sensation over the "regimental badge" area (skin over deltoid)
- Quadrangular space syndrome (compression in quadrilateral space)
5.6 Radial Nerve Injury (C5–T1 — Posterior cord)
Cause: Fracture of mid-shaft of humerus ("Saturday night palsy"), axillary compression.
Result: Wrist drop — inability to extend the wrist and fingers (posterior compartment muscles paralysed); sensory loss over anatomical snuffbox and dorsum of hand (C7 territory).
5.7 Musculocutaneous Nerve Injury (C5–C7 — Lateral cord)
Cause: Coracobrachialis piercing, anterior shoulder dislocation.
Result: Weak flexion and supination of forearm; sensory loss over lateral forearm.
5.8 Thoracic Outlet Syndrome (TOS)
The brachial plexus must traverse several anatomically narrow passages where it is vulnerable to compression:
| Type | Site of Compression | Cause |
|---|---|---|
| Scalene syndrome (Cervical rib syndrome) | Interscalene space | Cervical rib or fibrous band; present in ~1% of population |
| Costoclavicular syndrome | Space between 1st rib and clavicle | Drooping shoulders, clavicular fracture |
| Hyperabduction syndrome | Under pectoralis minor / coracoid process | Arm raised above head |
| Backpack paralysis | Direct plexus compression | Chronic heavy shoulder loads |
Clinical features: Pain radiating down the arm (ulnar side predominant), paresthesias, circulatory impairment.
— THIEME Atlas of Anatomy, p. 382
5.9 Brachial Plexus Injury in Adults — Classification by Level
| Level of Injury | Structure Affected | Typical Cause |
|---|---|---|
| Preganglionic (avulsion) | Root avulsed from spinal cord | High-speed trauma (motorcycle); poorest prognosis; no Tinel sign |
| Postganglionic (rupture) | Root or trunk torn outside cord | Blunt trauma, traction |
| Cord/division level | Glenohumeral dislocation | Shoulder dislocation |
- Preganglionic avulsion: no possibility of spontaneous recovery; requires nerve grafting/transfer
- Electrodiagnostic studies (EMG/NCS) + MRI/CT myelography used to map extent
— Gray's Anatomy for Students, p. 867
5.10 Neonatal Brachial Plexus Palsy — Summary
| Type | Roots | Deformity | Prognosis |
|---|---|---|---|
| Erb–Duchenne | C5–C6 | Waiter's tip | Best (~90% resolve) |
| Klumpke | C8–T1 | Claw hand + Horner | Poor |
| Total palsy | C5–T1 | Flail arm | Worst |
Causes: Large neonate, shoulder dystocia, forceps delivery, breech position.
Management: Passive ROM exercises; surgical reconstruction considered if no recovery by 3–6 months.
6. Summary Table — The Brachial Plexus at a Glance
| Component | No. | Location | Nerve Roots |
|---|---|---|---|
| Roots | 5 | Interscalene space | C5–T1 |
| Trunks | 3 | Posterior triangle (above clavicle) | C5–T1 |
| Divisions | 6 | Behind clavicle | C5–T1 |
| Cords | 3 | In axilla (around 2nd part of axillary artery) | Lateral (C5–C7), Medial (C8–T1), Posterior (C5–T1) |
| Terminal branches | 5 major | Axilla and arm | Musculocutaneous, Median, Ulnar, Radial, Axillary |
Sources: Gray's Anatomy for Students (pp. 858–867) | THIEME Atlas of General Anatomy and Musculoskeletal System (pp. 381–382) | Miller's Review of Orthopaedics 9th Ed. | Bradley and Daroff's Neurology in Clinical Practice | The Harriet Lane Handbook 23rd Ed.
This is a shared conversation. Sign in to Orris to start your own chat.