Foetal circulation physiology detailed explanation in simple way
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the information needed for a comprehensive, well-illustrated answer. Let me compile the full response.
Foetal Circulation - A Simple, Detailed Explanation
Here is a complete walkthrough of how blood circulates in a foetus, why it differs from adult circulation, and what happens at birth.
Why Is Foetal Circulation Different?
In a foetus, the lungs do not work - they are filled with fluid and cannot provide oxygen. The placenta does the job of the lungs. So the entire circulatory system is designed to:
- Bring oxygen-rich blood from the placenta to the foetal body
- Bypass the lungs (since they are non-functional)
- Partially bypass the liver (to reduce resistance and speed up circulation)
To achieve this, the foetus has 3 special shunts (shortcuts) that do not exist in adults.
The 3 Special Shunts
| Shunt | Location | What It Does |
|---|---|---|
| Ductus Venosus | Liver | Bypasses the liver |
| Foramen Ovale | Heart (between atria) | Bypasses the lungs (right → left atrium shortcut) |
| Ductus Arteriosus | Between pulmonary artery & aorta | Bypasses the lungs (pulmonary artery → aorta shortcut) |
Step-by-Step Blood Flow (Follow the Journey)
Here is the diagram of foetal circulation from The Developing Human (Moore & Persaud):
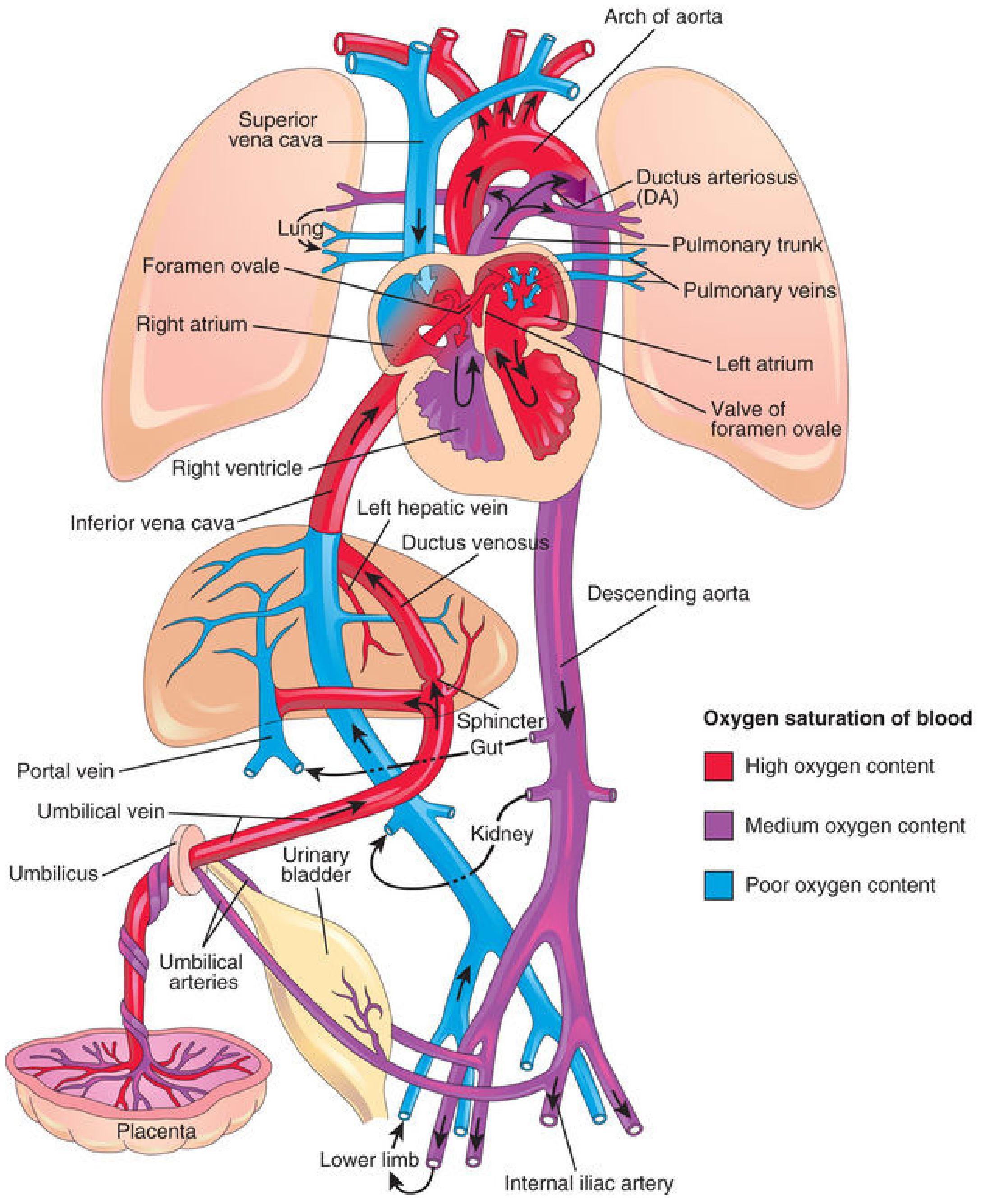
Step 1 - Oxygenated Blood Leaves the Placenta
- The placenta (not the lungs) oxygenates the foetal blood
- Blood leaving the placenta travels via the umbilical vein - this is the only vein in the body that carries oxygenated blood (the opposite of adult anatomy!)
- Oxygen saturation here: ~80% (Ganong's, p.614)
Step 2 - Ductus Venosus (Liver Bypass)
- As the umbilical vein approaches the liver, the blood splits:
- ~50% goes through the ductus venosus - a direct shortcut into the inferior vena cava (IVC), bypassing the liver
- ~50% enters the liver sinusoids and then joins the IVC via hepatic veins
- A physiological sphincter near the umbilical vein regulates this flow - it prevents the heart from being overloaded during uterine contractions
- After mixing in the IVC with deoxygenated blood from the lower limbs and abdomen, the saturation drops to about ~67%
(The Developing Human, p.873)
Step 3 - Blood Enters the Right Atrium
- The IVC blood (mixed, but still relatively well-oxygenated) enters the right atrium
- The crista dividens (lower border of the septum secundum) acts like a traffic director:
- It guides most of the IVC blood through the foramen ovale directly into the left atrium (the better-oxygenated blood is preferentially sent to the left side)
- A small amount stays in the right atrium and mixes with poorly oxygenated blood from the superior vena cava (SVC) - blood returning from the head and arms
Step 4 - Foramen Ovale (Right-to-Left Atrial Shunt)
- The foramen ovale is a hole in the wall between the two atria
- It allows blood to jump from the right atrium → left atrium, completely bypassing the lungs
- This is kept open in foetal life because right atrial pressure > left atrial pressure (the lungs are collapsed, so very little blood returns from them to the left atrium)
Step 5 - Left Atrium → Left Ventricle → Ascending Aorta
- Blood in the left atrium mixes with the tiny amount returning from the (non-functioning) lungs
- It passes to the left ventricle, then pumps into the ascending aorta
- The first branches off the ascending aorta are the coronary arteries (heart muscle) and the carotid arteries (brain) - so the heart and brain receive the best-oxygenated blood in the foetus. Very smart design!
Step 6 - The Right Side: SVC Blood → Right Ventricle → Pulmonary Artery
- The deoxygenated blood from the SVC (head and arms) enters the right atrium, goes to the right ventricle, and is pumped into the pulmonary artery
- In a foetus, the pulmonary vascular resistance is very HIGH (lungs are fluid-filled and collapsed), so the pressure in the pulmonary artery is actually higher than in the aorta
- Result: most blood cannot enter the lungs and instead takes the shortcut...
Step 7 - Ductus Arteriosus (Lung Bypass)
- The ductus arteriosus connects the pulmonary artery to the descending aorta
- Most of the blood from the right ventricle flows through this duct into the descending aorta, completely bypassing the lungs
- This relatively desaturated blood now supplies the lower body and trunk of the foetus
- O2 saturation here: ~60%
(Ganong's Review of Medical Physiology, p.614)
Step 8 - Blood Returns to the Placenta
- From the descending aorta, blood flows into the two umbilical arteries (note: these are arteries but they carry deoxygenated blood - another reversal from adult anatomy!)
- The umbilical arteries wrap around the bladder and travel through the umbilical cord back to the placenta to be re-oxygenated
Where Does Mixing of Oxygenated and Deoxygenated Blood Occur?
Blood is never 100% pure at any point in the foetal circulation - mixing happens at 5 key places (Langman's Medical Embryology, p.236-237):
| Point | What Mixes |
|---|---|
| I. Liver | Umbilical vein mixes with portal blood |
| II. IVC | Oxygenated blood mixes with deoxygenated blood from lower limbs |
| III. Right atrium | IVC blood mixes with SVC blood |
| IV. Left atrium | Blood from foramen ovale mixes with small pulmonary return |
| V. Descending aorta | Blood from aorta mixes with blood from ductus arteriosus |
Summary Schematic (Fetus vs Newborn vs Adult)
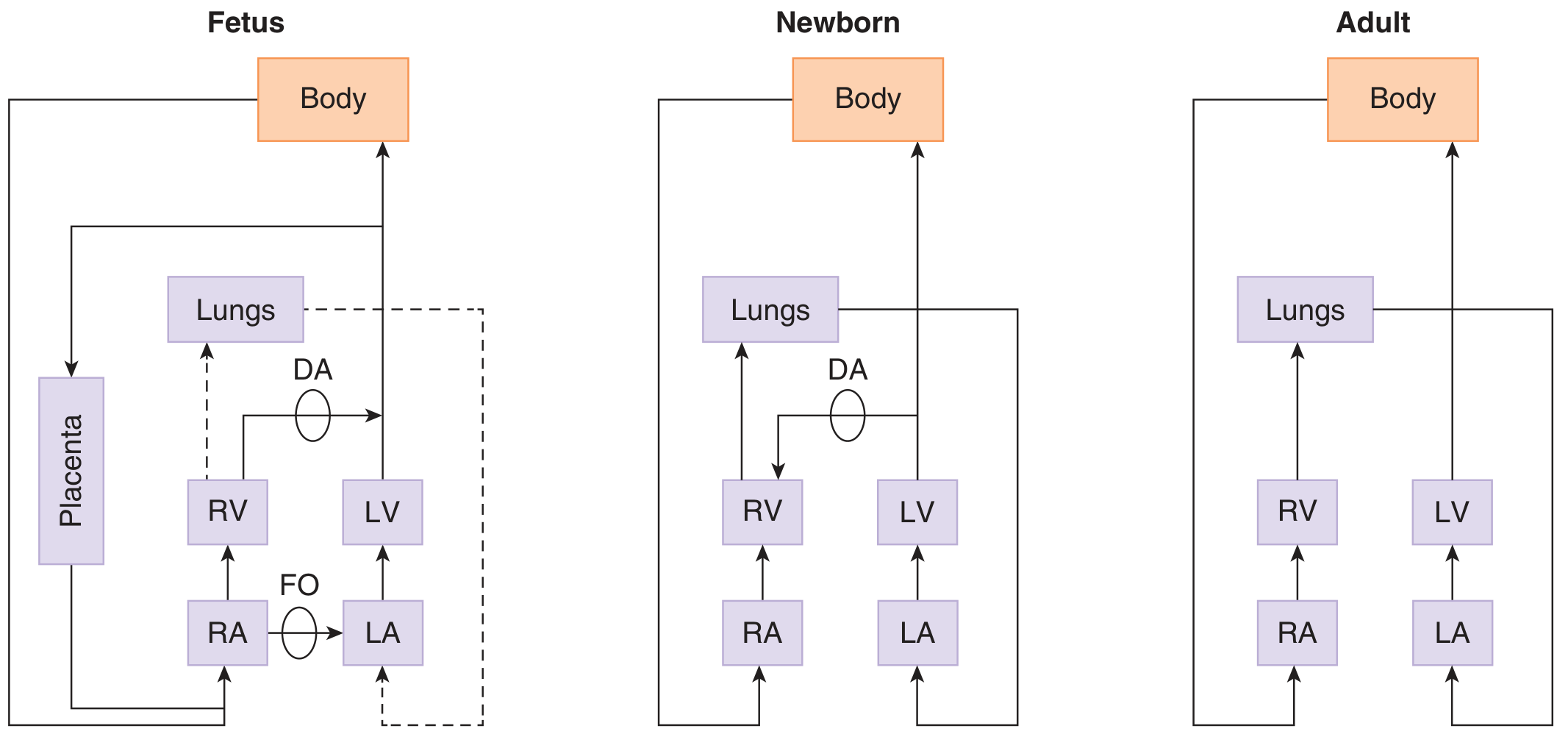
Notice how in the foetus, both ventricles effectively work in parallel (both supply the body), while in adults they work in series (right side → lungs → left side → body).
What Happens at Birth? (Circulatory Changes)
At the moment of birth, three major events happen:
1. Lungs Expand → Pulmonary Resistance Falls
- The baby's first breath fills the lungs with air
- Pulmonary vascular resistance drops dramatically
- Blood now rushes into the lungs instead of bypassing them
2. Foramen Ovale Closes (Functionally)
- More blood now returns from the lungs to the left atrium, raising left atrial pressure
- Simultaneously, the umbilical cord is cut, removing the low-resistance placental circuit - right atrial pressure falls
- The pressure reversal (left > right) pushes the septum primum against the septum secundum, functionally closing the foramen ovale
- Permanent anatomical closure happens over weeks to months (the fused tissue becomes the fossa ovalis)
3. Ductus Arteriosus Closes
- The rise in arterial oxygen tension (PaO2) triggers muscular contraction of the ductus arteriosus wall
- Prostaglandins (especially PGE2), which kept the ductus open during foetal life, are now cleared by the lungs
- Functional closure occurs within hours; permanent fibrous closure forms the ligamentum arteriosum within weeks
4. Ductus Venosus Closes
- With cord clamping, blood flow through the umbilical vein stops
- The ductus venosus collapses and becomes the ligamentum venosum
- The umbilical vein becomes the ligamentum teres (round ligament of the liver)
- The umbilical arteries become the medial umbilical ligaments
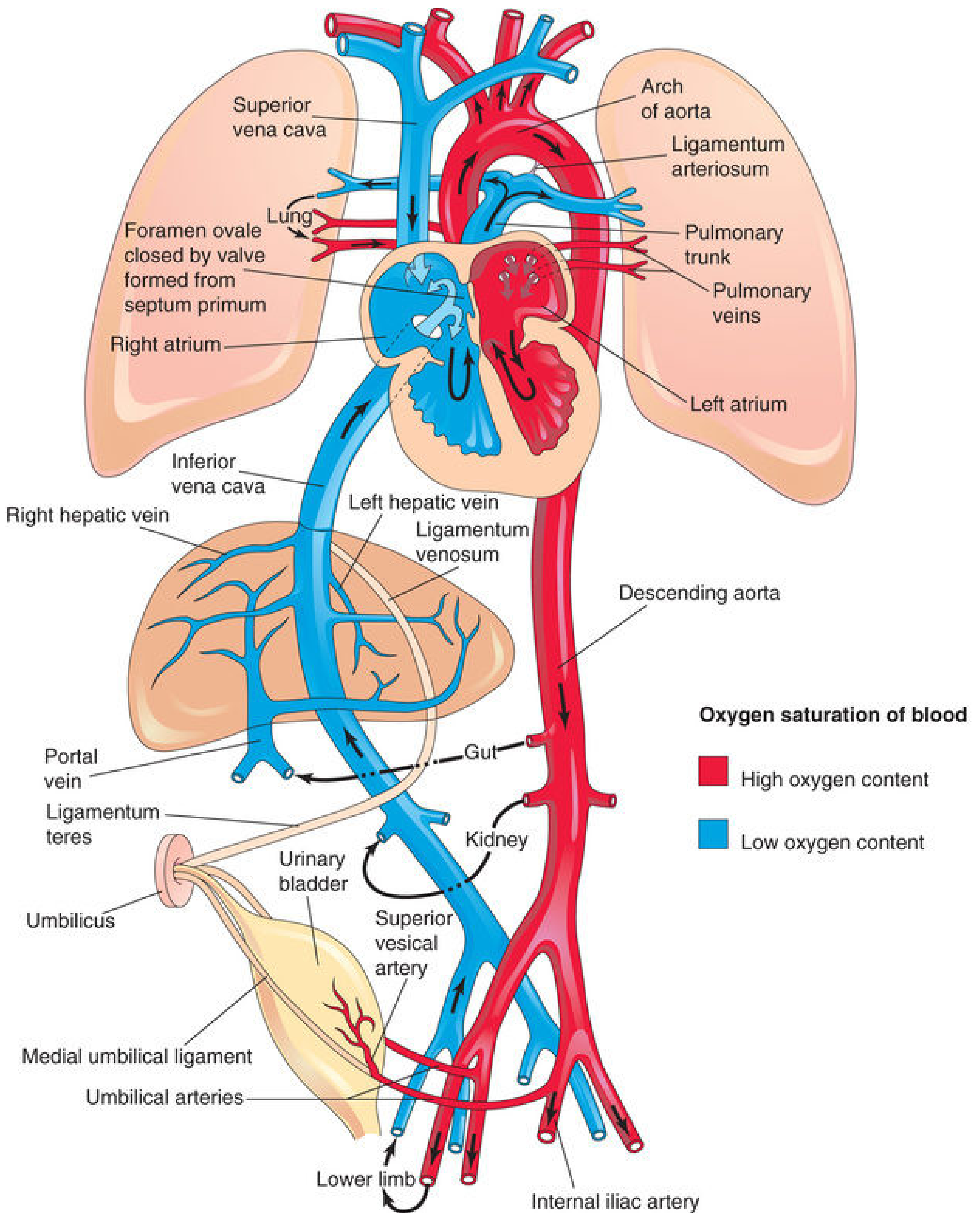
Adult Remnants of Foetal Structures
| Foetal Structure | Adult Remnant |
|---|---|
| Foramen ovale | Fossa ovalis |
| Ductus arteriosus | Ligamentum arteriosum |
| Ductus venosus | Ligamentum venosum |
| Umbilical vein | Ligamentum teres (round ligament) |
| Umbilical arteries | Medial umbilical ligaments |
Key Oxygen Saturation Values to Remember
| Location | O2 Saturation |
|---|---|
| Umbilical vein (from placenta) | ~80% |
| IVC (after mixing) | ~67% |
| Umbilical arteries (returning to placenta) | ~58-60% |
| Adult arterial blood | ~98% |
Why Does the Foetus Tolerate Such Low O2 Saturations?
Foetal tissues tolerate this because:
- Foetal haemoglobin (HbF) has a higher affinity for oxygen than adult HbG - it picks up oxygen more readily at the placental level
- The Bohr effect: maternal blood has higher CO2 (and thus lower pH), which causes maternal Hb to release oxygen more readily - this oxygen is then picked up by HbF
- Foetal tissues have a remarkable but poorly understood resistance to hypoxia (Ganong's, p.615)
Sources: The Developing Human: Clinically Oriented Embryology (Moore & Persaud), 10th ed., pp. 869-875 | Langman's Medical Embryology, 14th ed., pp. 236-238 | Ganong's Review of Medical Physiology, 26th ed., pp. 613-615
This is a shared conversation. Sign in to Orris to start your own chat.