RA with cardiac and pulmonary involvement dig and dd ?
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Searching PubMed
rheumatoid arthritis cardiac pulmonary manifestations
Loading Image
Loading Image
Loading Image
I now have all the information needed for a thorough answer. Here is the comprehensive response:
Rheumatoid Arthritis: Cardiac & Pulmonary Involvement
Diagnosis (Dig) and Differential Diagnosis (DD)
CARDIAC INVOLVEMENT
Spectrum of Direct Cardiac Manifestations
| Structure | Manifestation | Notes |
|---|---|---|
| Pericardium | Pericardial effusion, fibrinous pericarditis, constrictive pericarditis | Most common direct cardiac complication; 50% prevalence on echo but usually asymptomatic |
| Myocardium | Myocarditis, rheumatoid nodule infiltration, amyloid deposition | Often subclinical; detected by echo or cardiac MRI |
| Valves | Fibrosis, nodule on valve ring, aortic regurgitation | Less common |
| Coronary arteries | Coronary arteritis; accelerated atherosclerosis | Inflammation + conventional CV risk factors |
| Conduction system | Conduction defects, arrhythmias | From inflammation or nodules |
| Vasculature | Pulmonary hypertension, venous thromboembolism | Increased VTE incidence |
Key points:
- Pericardial effusions occur in up to 50% by echocardiography but are usually asymptomatic. Long-standing disease can progress to fibrinous or constrictive pericarditis.
- The most common cause of death in RA is cardiovascular disease. Patients have significantly increased coronary artery disease and heart failure (approximately 2x the general population rate), even after controlling for traditional risk factors like smoking, hypertension, and obesity. Chronic inflammation is the primary driver, compounded by glucocorticoid use and physical inactivity.
- Congestive heart failure (both systolic and diastolic dysfunction) occurs at ~2x the background rate.
- Cardiac MRI is sensitive for subclinical myocardial involvement.
(Goldman-Cecil Medicine, p. 2792; Harrison's 22E, p. 2885; Morgan & Mikhail Clinical Anesthesiology, p. 1511)
Differential Diagnosis of RA Cardiac Findings
For pericardial effusion/pericarditis:
- Other CTD: SLE (most common CTD-pericarditis), systemic sclerosis, MCTD
- Viral/idiopathic pericarditis
- Tuberculous pericarditis (especially important in endemic areas; low pleural/pericardial glucose can mimic RA)
- Malignant pericardial effusion
- Hypothyroid pericardial effusion
- Uremic pericarditis
- Dressler syndrome (post-MI)
For coronary artery disease:
- Primary atherosclerosis (shared risk factors)
- Coronary vasculitis (PAN, Kawasaki disease)
- Other inflammatory arthropathies (AS, psoriatic arthritis - also have elevated CV risk)
For valvular disease:
- Rheumatic heart disease (mitral > aortic)
- Libman-Sacks endocarditis (SLE)
- Infective endocarditis
For conduction defects:
- Cardiac sarcoidosis
- Systemic sclerosis
- Cardiac amyloidosis
- SLE
PULMONARY INVOLVEMENT
Intrathoracic Manifestations of RA
(Grainger & Allison's Diagnostic Radiology, Table 9.5)
| Manifestation | Frequency / Key Features |
|---|---|
| Pleural effusion / thickening | Most common manifestation; up to 20% of patients; 80% in men |
| Interstitial lung disease (ILD) | UIP most common, then NSIP; prevalence up to 12-45% |
| Obliterative (constrictive) bronchiolitis | Air trapping on HRCT; may require lung transplantation |
| Bronchiectasis | Up to 30% of RA patients |
| Organising pneumonia (COP/BOOP) | Less common |
| Follicular bronchiolitis | Centrilobular nodules; part of lymphoproliferative spectrum |
| Necrobiotic (rheumatoid) nodules | Well-circumscribed; may cavitate; may cause pneumothorax |
| Caplan syndrome | Nodules + pneumoconiosis (coal/silica exposure) |
| Drug-induced lung disease | Methotrexate pneumonitis |
| Pulmonary hypertension | Via vasculitis |
| Pulmonary vasculitis | Rare |
(Harrison's 22E; Fishman's Pulmonary Diseases; Grainger & Allison's)
1. Pleural Effusion
- Exudate; very low glucose (<30 mg/dL) - this is virtually pathognomonic of RA or empyema
- Elevated LDH, elevated RF, low complement
- Variably serous, purulent, milky, or hemorrhagic appearance
- May progress to pseudochylothorax (cholesterol effusion) in chronic disease
- Trapped lung / fibrothorax can result from untreated chronic effusion
Pleural fluid profile:
| Parameter | RA Pleural Fluid |
|---|---|
| Glucose | Often <30 mg/dL |
| Protein | High (exudate) |
| LDH | High |
| Complement | Low |
| RF | Elevated |
| Leukocytes | Usually <10,000/μL |
(Fishman's Pulmonary Diseases, p. 1359)
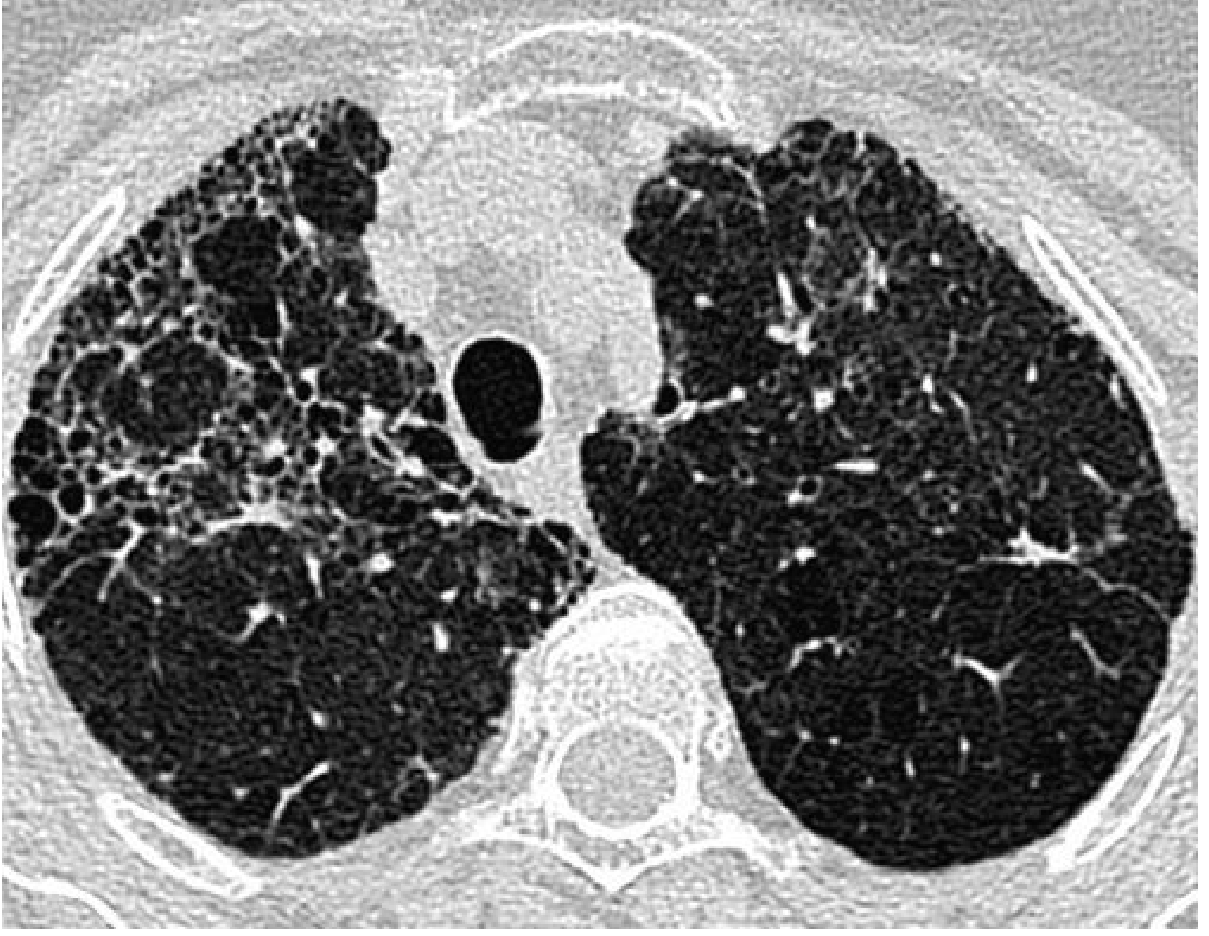
2. Interstitial Lung Disease (ILD)
- UIP pattern is the most frequent histopathological type (honeycomb changes, peripheral/lower lobe basal predominance)
- NSIP is second most common (bilateral ground-glass opacities, fine reticulations, traction bronchiectasis)
- More common in men, seropositive patients, smokers, high disease activity
- May precede joint symptoms in up to 3.5% of patients
- Pulmonary function: restrictive pattern + reduced DLCO
- Prognosis better than idiopathic UIP/IPF; responds better to immunosuppression
HRCT RA-ILD (UIP pattern) - peripheral honeycombing bilateral:
3. Necrobiotic (Rheumatoid) Pulmonary Nodules
- Associated with subcutaneous nodules; wax and wane
- Single or multiple, 2mm to several cm, well-circumscribed
- May cavitate; subpleural location can cause pneumothorax
- Show increased FDG uptake on PET - do NOT misinterpret as metastatic disease
- May occur in association with pulmonary fibrosis and pleural changes

CXR demonstrating bilateral lower zone changes in RA:

4. Caplan Syndrome
- RA + pneumoconiosis (coal workers' pneumoconiosis or silicosis)
- Discrete nodules predominantly in upper lobes; appear suddenly
- Histologically identical to necrobiotic nodules
- (Harrison's 22E; Fishman's; Goldman-Cecil)
Classical HRCT Summary for RA Pulmonary Disease
(Grainger & Allison's Diagnostic Radiology)
- Pleural effusions are common
- UIP is more frequent than NSIP (opposite to systemic sclerosis)
- Bronchiectasis in up to 30%
- Obliterative bronchiolitis causes extensive air trapping
- Necrobiotic nodules: well-circumscribed, may cavitate, may be subpleural
DIFFERENTIAL DIAGNOSIS OF RA PULMONARY MANIFESTATIONS
For ILD / Pulmonary Fibrosis:
| Condition | Distinguishing Features |
|---|---|
| Idiopathic Pulmonary Fibrosis (IPF) | No synovitis, no RF/ACPA, UIP pattern identical on HRCT - requires clinical context; RA-ILD has better prognosis |
| SLE-ILD | ANA+, anti-dsDNA; NSIP more common than UIP |
| Systemic Sclerosis ILD | Sclerodactyly, Raynaud's, NSIP >> UIP, dilated esophagus on HRCT |
| Polymyositis/DM-ILD | Elevated CK, anti-Jo-1; rapid onset possible |
| Hypersensitivity pneumonitis | Exposure history, upper/mid lobe predominance, mosaic attenuation |
| Sarcoidosis | Perihilar lymphadenopathy, upper lobe predominance, non-caseating granulomas |
| Drug-induced (MTX pneumonitis) | Temporal link to drug; eosinophilia; partially reversible |
For Pleural Effusion in RA:
- SLE pleuritis (glucose normal, ANA +ve)
- Tuberculous pleuritis (lymphocytic; low glucose can overlap - always exclude)
- Malignant effusion (cytology)
- Heart failure (transudatate)
- Empyema (glucose <30 also - key overlap with RA; culture mandatory)
For Pulmonary Nodules in RA:
- Primary lung carcinoma (FDG-avid - PET not diagnostic alone)
- Metastatic disease
- Pulmonary carcinoid
- Granulomatous infections (TB, fungal - especially in immunosuppressed RA patients)
- Wegener's/GPA nodules (cavitating; c-ANCA, PR3)
- Sarcoid nodules
Key Clinical Pearls
- Pleuro-pulmonary disease may precede arthritis in a significant minority of RA patients - maintain suspicion even without established RA diagnosis.
- Glucose <30 mg/dL in pleural fluid = RA or empyema only - always culture to exclude infection.
- RA-ILD has a better prognosis than IPF and responds better to immunosuppression, but the HRCT UIP pattern is radiologically identical - clinical context (RF, ACPA, joint disease) is essential.
- Cardiovascular disease is the leading cause of death in RA - the 2x excess risk of IHD and heart failure cannot be explained by traditional risk factors alone.
- MTX-related lung toxicity can mimic RA-ILD - temporal drug relationship and eosinophilia are clues.
- FDG-PET: necrobiotic nodules are FDG-avid and must not be mistaken for malignancy.
- In immunosuppressed RA patients, opportunistic infections (PCP, CMV, aspergillus) must always enter the DD for acute pulmonary deterioration.
Sources: Harrison's Principles of Internal Medicine 22E (2025); Goldman-Cecil Medicine 2-Vol Set; Fishman's Pulmonary Diseases and Disorders; Grainger & Allison's Diagnostic Radiology; Morgan & Mikhail's Clinical Anesthesiology 7e; Fuster & Hurst's The Heart 15E
This is a shared conversation. Sign in to Orris to start your own chat.