Deatiled note on varicose veins with diagram
Reading File
Finding Sources
Finding Sources
Searching the Web
varicose veins pathophysiology anatomy treatment detailed medical notes diagram
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Detailed anatomy of varicose veins with diagram
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching the Web
varicose veins detailed anatomy saphenous veins perforators valves diagram medical
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Loading Image
I now have all the anatomy diagrams and comprehensive textbook content needed. Let me compose the detailed anatomical note.
Detailed Anatomy of Varicose Veins
1. Definition
Varicose veins are dilated, bulging, tortuous superficial veins measuring at least 3 mm in diameter. They occur when sustained elevated intraluminal pressure causes venous wall dilation and subsequent incompetence of the venous valves. - Harrison's Principles of Internal Medicine 22E, p. 2223
Related spectrum of venous dilatation:
| Type | Diameter | Appearance |
|---|---|---|
| Telangiectasias (spider veins) | < 1 mm | Blue, purple or red linear/branching patterns near skin surface |
| Reticular veins | 1-3 mm | Dilated intradermal veins, blue-green, do not protrude |
| Varicose veins | ≥ 3 mm | Dilated, bulging, tortuous, protrude above skin surface |
2. Normal Venous Anatomy of the Lower Limb (The Essential Background)
Understanding varicose veins requires a thorough knowledge of normal lower limb venous anatomy. The system is divided into three compartments: superficial, deep, and perforating. - Mulholland & Greenfield's Surgery 7e, p. 5214
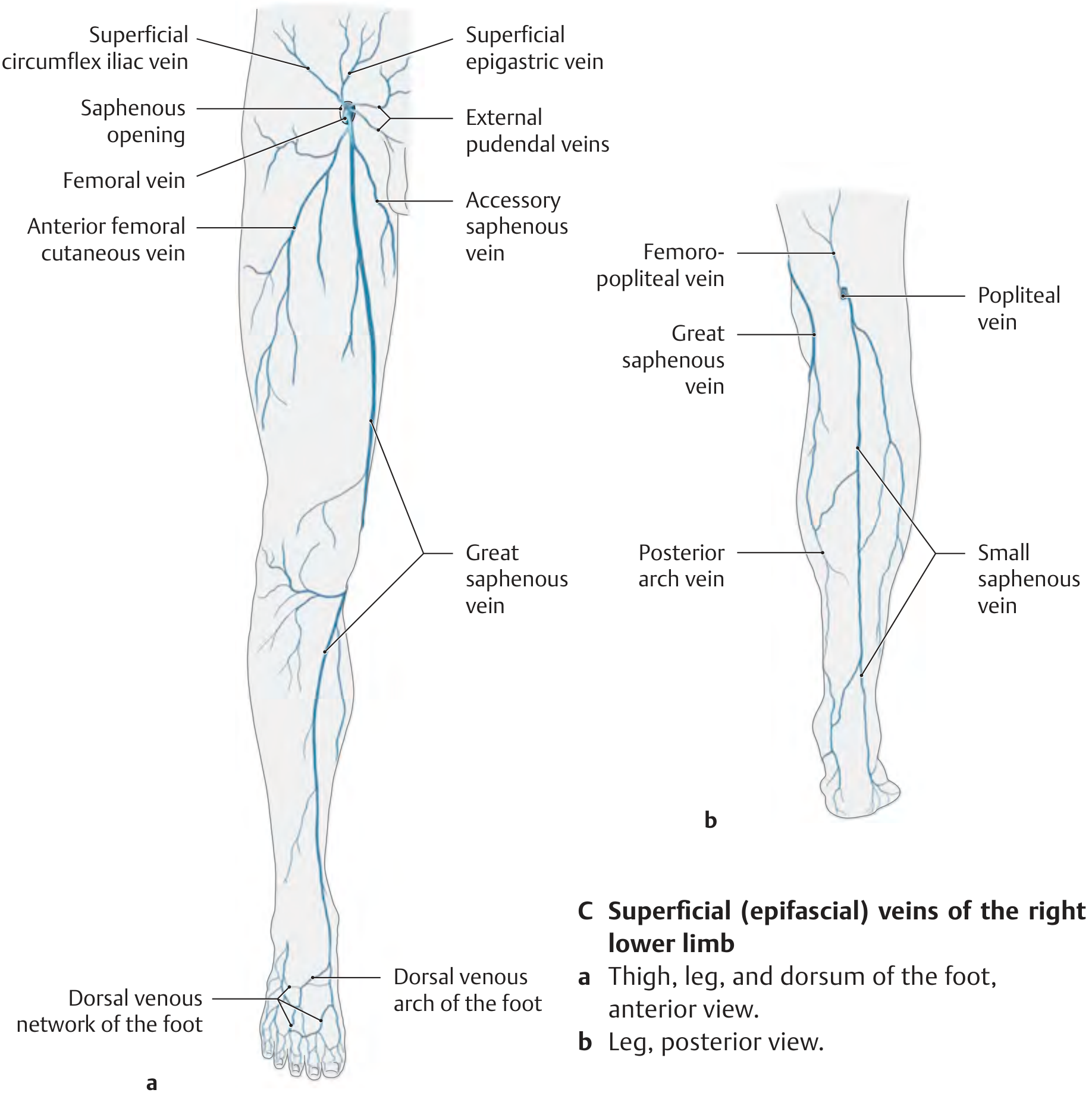
2.1 Superficial Venous System
The superficial veins lie above the deep (muscular) fascia, within the subcutaneous tissue. They are surrounded by a distinct saphenous fascial compartment - with the muscular fascia below and the saphenous fascia above. - Mulholland & Greenfield's Surgery 7e, p. 5214
Great Saphenous Vein (GSV)
- The longest vein in the body
- Originates from the medial end of the dorsal venous arch of the foot
- Passes anterior to the medial malleolus
- Ascends along the medial aspect of the calf and thigh
- Drains into the common femoral vein at the saphenofemoral junction (SFJ) in the groin, passing through the saphenous opening (fossa ovalis) in the deep fascia
- Contains 4-25 valves (commonly >6), with at least one valve within a few centimeters of the SFJ
- The SFJ typically has at least four named tributaries: superficial epigastric vein, superficial circumflex iliac vein, superficial external pudendal veins, and the accessory saphenous vein
- The saphenous nerve runs within the GSV compartment below the knee and is at risk during surgery
- Complete duplication of the GSV in the thigh occurs in ~8% of cases, with partial duplication in a further 25% - Mulholland & Greenfield's Surgery 7e, p. 5215
Small Saphenous Vein (SSV)
- Originates from the dorsolateral aspect of the foot
- Passes posterior to the lateral malleolus
- Ascends along the posterolateral calf
- Drains into the popliteal vein at the saphenopopliteal junction (SPJ), usually at the popliteal crease
- Contains an average of 7-10 valves (range 4-13)
- The sural nerve lies in close proximity within the SSV compartment and is at risk during surgery
- The SSV drains into the popliteal vein in fewer than two-thirds of cases - it can travel well above the knee before diving to meet the deep system (the Giacomini vein is a thigh extension of the SSV)
- Mulholland & Greenfield's Surgery 7e, p. 5215
Diagram - Superficial (epifascial) veins of the lower limb:
2.2 Deep Venous System
The deep veins lie beneath the muscular fascia, accompanying the major arteries:
| Level | Veins |
|---|---|
| Calf | Paired peroneal, anterior tibial, and posterior tibial veins; soleal sinuses; gastrocnemius veins |
| Knee | Popliteal vein (convergence of calf veins) |
| Thigh | Femoral vein (continuation of popliteal vein) |
| Groin | Common femoral vein (femoral + deep femoral vein) |
| Pelvis | External iliac → Common iliac → IVC |
Key facts:
- Tibial and peroneal veins contain 7-19 valves each
- Popliteal vein has 1-2 valves; femoral vein has ~3 valves
- ~70% of common femoral veins have a valve within 1 cm of the inguinal ligament
- Common iliac veins are generally valveless
- The soleal sinuses act as the primary blood reservoir and pump during calf muscle contraction - Harrison's 22E, p. 2223; Mulholland & Greenfield's, p. 5215
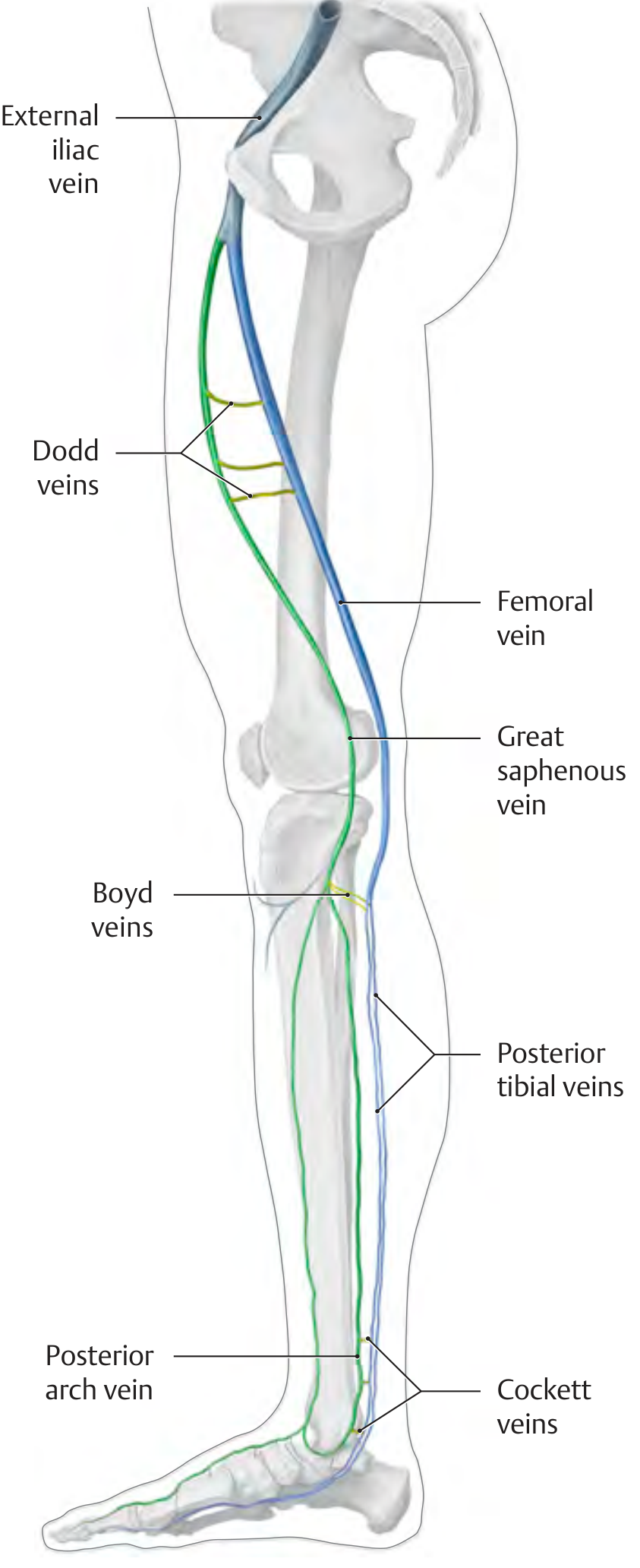
2.3 Perforating (Communicating) Veins
Perforating veins penetrate the deep muscular fascia to connect the superficial and deep systems. Normally, their valves direct blood flow from superficial → deep (inward flow). When these valves become incompetent, blood flows outward (from deep → superficial), causing increased pressure and dilation of the superficial veins. - THIEME Atlas of Anatomy, p. 551
The four clinically important perforating vein groups (medial aspect of the leg):
| Group | Location | Connects |
|---|---|---|
| Hunterian perforators | Upper-middle thigh | GSV ↔ Femoral vein |
| Dodd (Hunter) perforators | Medial thigh, middle third / adductor canal level | GSV ↔ Femoral vein |
| Boyd perforators | Medial leg, just below the knee | GSV ↔ Posterior tibial veins |
| Cockett perforators (I, II, III) | Medial distal leg, 5, 10, 15 cm above medial malleolus | Posterior arch vein ↔ Posterior tibial veins |
| Inframallleolar perforators | Medial ankle | Ankle veins ↔ Deep system |
- THIEME Atlas of Anatomy - General Anatomy & Musculoskeletal System, p. 551
- Gray's Anatomy for Students, p. [varicose veins section]
Diagram - Named perforating veins (medial view):
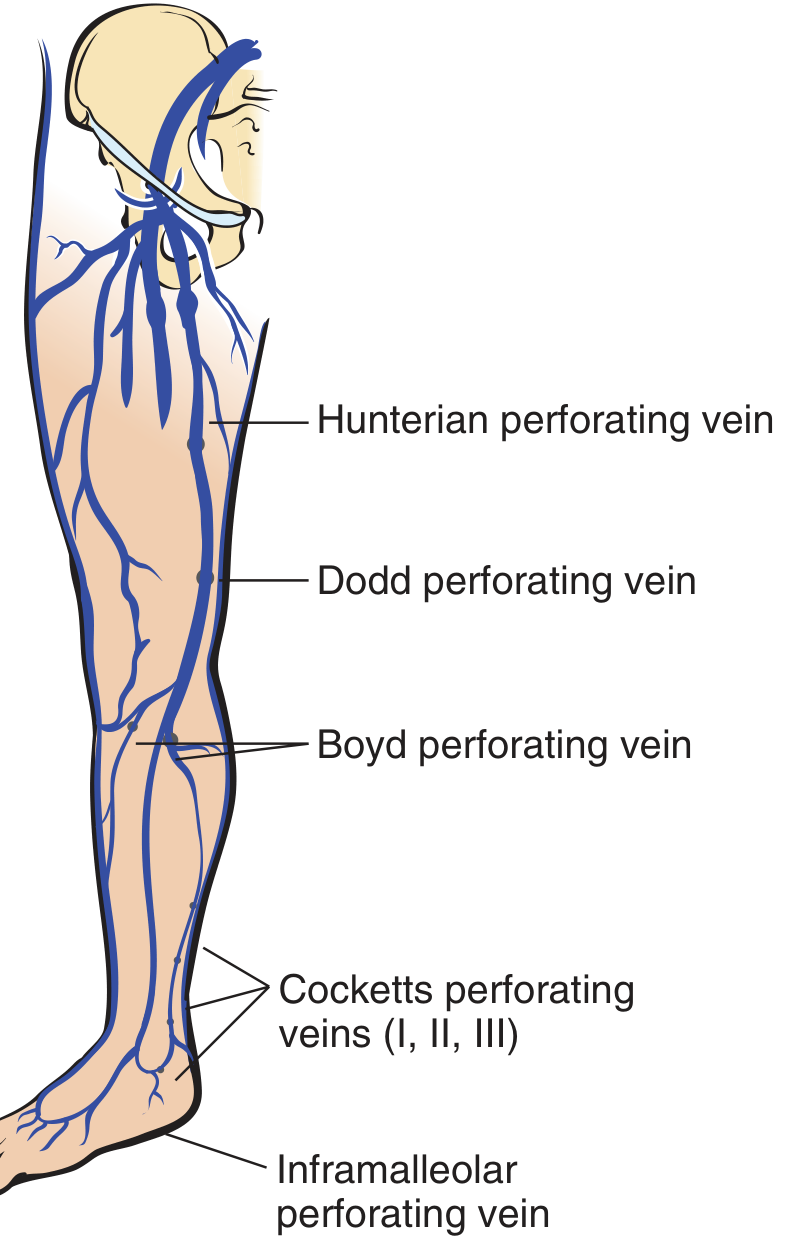
Diagram - Deep vs. superficial system with perforators (3D cross-section):
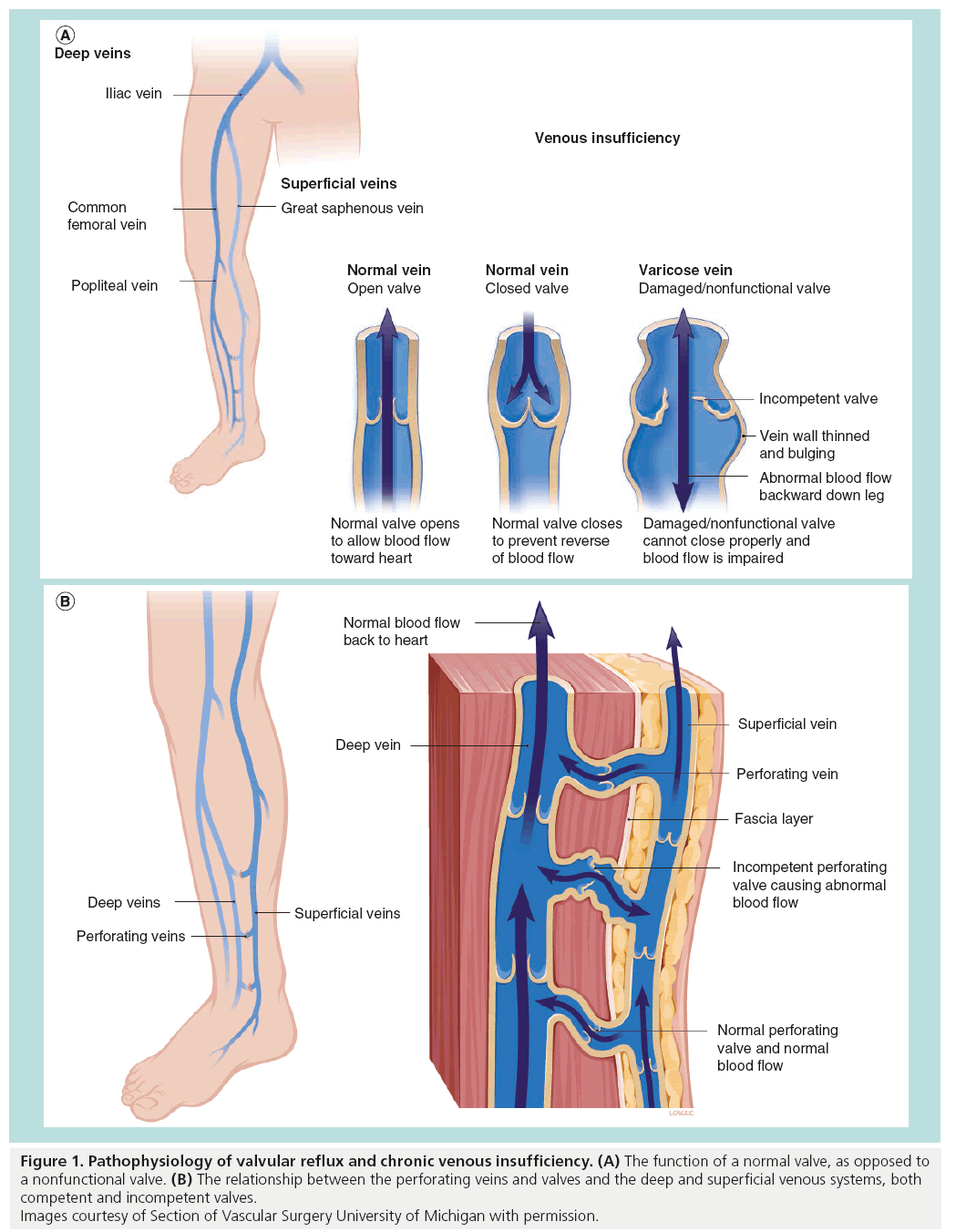
3. Venous Valves - The Anatomical Key
The bicuspid venous valves are the central anatomical feature whose failure produces varicose veins.
- Valves are composed of a fine connective tissue skeleton covered by endothelium
- They are bicuspid (two cusps), delicate yet extremely strong
- They direct blood flow: superficial → deep and caudad → cephalad (against gravity)
- With exception of the foot veins (where flow can be reversed during muscle relaxation)
- The common iliac vein is generally valveless; only 10% of internal iliac and 25% of external iliac veins have valves
Normal vs. Varicose Valve Function:

4. The Calf Muscle Pump - Functional Anatomy
The calf muscle pump is the primary anatomical mechanism for venous return:
-
Systolic phase (muscle contraction): The soleal sinuses and deep calf veins are compressed within their fascial envelope, generating pressures up to 300 cmH₂O. Blood is forced proximally through competent valves into the valveless veins of the abdomen. Perforator valves close to prevent escape into the superficial system.
-
Diastolic phase (muscle relaxation): Calf compartment pressure falls. Blood flows from the superficial veins through competent perforators into the deep system (superficial system acts like an "atrium"; deep veins like a "ventricle").
-
Standing still: Foot vein pressure = hydrostatic column from foot to right heart ≈ 70-80 cmH₂O. - Pfenninger & Fowler's Procedures for Primary Care, p. 636
When venous walls dilate (from any cause), valves fail → blood refluxes downward with gravity → further pressure rise → further dilation. This self-perpetuating cycle produces varicose veins.
5. Sites of Valvular Incompetence in Varicose Veins
The typical anatomical sites where valvular incompetence occurs, producing clinically significant varicosities: - Gray's Anatomy for Students
- Saphenofemoral junction (SFJ) - the saphena varix; GSV meets femoral vein in the groin
- Midthigh Hunterian/Dodd perforators - between GSV and femoral vein
- Calf Cockett perforators - 5, 10, and 15 cm above the medial malleolus
- Saphenopopliteal junction (SPJ) - SSV meets popliteal vein in the popliteal fossa
Clinical correlation:
- Medial thigh and calf varicosities → incompetent GSV/SFJ
- Posterolateral calf varicosities → incompetent SSV/SPJ
- Anterolateral thigh/calf varicosities → isolated anterior accessory GSV incompetence
- Bailey and Love's Short Practice of Surgery 28th Edition, p. 1051
6. Classification by Anatomical System
Primary varicose veins (~75%) - arise from intrinsic weakness and degeneration of the vein wall leading to valve incompetence, beginning in the superficial system. Familial in ~50% of cases.
Secondary varicose veins (~25%) - result from venous hypertension due to:
- Deep venous insufficiency or post-thrombotic limb (DVT sequelae)
- Incompetent perforating veins causing outward "blow-out" pressure
- Congenital conditions (e.g., Klippel-Trenaunay syndrome)
- Arteriovenous fistulas
- Harrison's 22E; Robbins Pathologic Basis of Disease
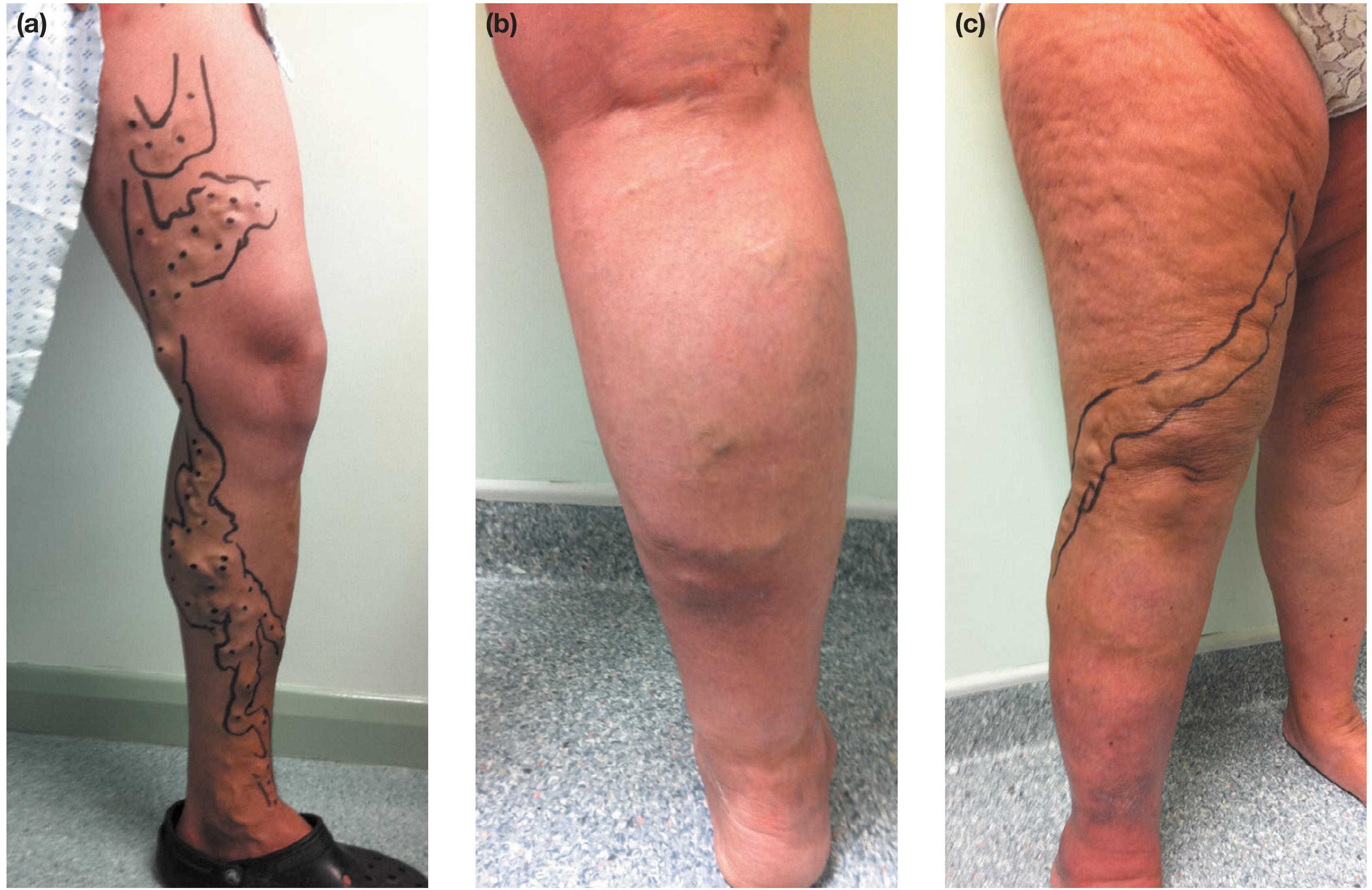
7. Clinical Anatomy - Distribution Patterns
8. Surgical Anatomy - Key Danger Points
| Structure | Location | At-Risk Procedure |
|---|---|---|
| Saphenous nerve | Within GSV compartment, below knee | GSV stripping - causes medial leg numbness |
| Femoral vein | Immediately adjacent to SFJ | High GSV ligation - risk of DVT if injured |
| Common peroneal nerve | Near fibular head/popliteal fossa | SSV surgery - causes foot drop |
| Sural nerve | Within SSV compartment | SSV stripping - causes lateral foot numbness |
The Gray's Anatomy for Students case illustrates exactly this: a surgeon ligating the SSV mistakenly injured the common peroneal nerve in the popliteal fossa, causing foot drop, sensory loss over the lateral leg/foot, and fibular muscle wasting. - Gray's Anatomy for Students
The SSV's variable termination - it joins the popliteal vein in fewer than two-thirds of cases - makes it particularly prone to surgical misidentification. Duplex ultrasound pre-marking is now mandatory before SSV surgery. - Mulholland & Greenfield's Surgery 7e
9. Key Anatomical Summary
LOWER LIMB VENOUS ANATOMY RELEVANT TO VARICOSE VEINS
IVC
|
Common iliac vein (no valves)
|
External iliac vein
|
Common femoral vein ←—[SFJ]—— Great Saphenous Vein (GSV)
| |
| medial thigh ← Hunterian/Dodd
| perforators perforating veins
| |
Femoral vein ←——————————————————— GSV calf
| |
| Cockett perforators
| (5, 10, 15 cm above
| medial malleolus)
|
Popliteal vein ←—[SPJ]———— Small Saphenous Vein (SSV)
| |
| posterolateral calf
|
Tibial/peroneal veins (deep)
Key principle: Valves fail → reflux (downward flow) → increased pressure → wall dilation → further valve failure → the varicose vein cycle continues. - Bailey and Love's 28th Edition; Harrison's 22E; Robbins Pathology
Sources: Harrison's Principles of Internal Medicine 22E | Bailey and Love's Short Practice of Surgery 28th Edition | Mulholland & Greenfield's Surgery 7e | THIEME Atlas of General Anatomy & Musculoskeletal System | Gray's Anatomy for Students | Pfenninger & Fowler's Procedures for Primary Care | Robbins, Cotran & Kumar Pathologic Basis of Disease
This is a shared conversation. Sign in to Orris to start your own chat.