4yr old patients come to opd the complaint is jaundice ,how to take complete history according to oldcaarts what are possible to ask the patients and complete physical examination what have to do
OLDCAARTS history taking jaundice pediatric child clinical examination
https://clinipedia.wordpress.com/2013/08/04/jaundice-how-to-…
History & Physical Examination: 4-Year-Old with Jaundice
HISTORY TAKING — OLDCAARTS Framework
Note on OLDCAARTS vs OLDCARTS: OLDCAARTS = Onset, Location, Duration, Character, Associated symptoms, Aggravating factors, Relieving factors, Temporal pattern, Severity. Applied below to jaundice in a 4-year-old child.
Patient Identification (Before OLDCAARTS)
- Name, age (4 years), sex, address
- Informant: mother/father/guardian — reliability
- Chief complaint: "Yellow discoloration of skin/eyes since ___"
O — Onset
- When did the yellow color first appear? (exact date or approximate)
- Was onset sudden or gradual?
- Was the child well before this, or was there a prodrome (fever, malaise, anorexia)?
- Did the jaundice start from the face downward or all over at once?
- Any triggering event: infection, new medication, food intake (e.g., fava beans in G6PD), blood transfusion?
L — Location
- Where is the yellowness most noticeable — eyes (sclera), skin, palms, nails?
- Is it generalized or localized?
- Is the yellowness also seen inside the mouth (soft palate, undersurface of tongue)?
Clinical tip: Jaundice appears first in the sclera (serum bilirubin >35–50 µmol/L), then skin. Carotenemia (from excess carrots/papaya) turns the skin yellow but spares the sclera — always check the eyes.
D — Duration
- How long has the jaundice been present?
- Is it getting worse, better, or the same since onset?
- Has this happened before? (recurrent episodes suggest hemolytic or hereditary cause)
- Duration helps distinguish: acute hepatitis A (days–weeks) vs. biliary obstruction (progressive) vs. chronic liver disease (months)
C — Character
- Color: pale lemon yellow → yellow-orange → deep yellow-green (deepening suggests biliary obstruction)
- Urine color: Dark (cola/tea-colored)? → conjugated hyperbilirubinemia (bilirubinuria)
- Stool color: Pale/clay-colored/acholic? → obstructive jaundice (biliary atresia, choledochal cyst, stone)
- Is the stool normal yellow/brown? → hemolytic or hepatocellular more likely
- Any itching (pruritus)? → cholestasis
A — Associated Symptoms
GI symptoms:
- Fever (hepatitis A, leptospirosis, malaria, enteric fever)
- Nausea, vomiting, loss of appetite (anorexia)
- Abdominal pain — location, severity, colicky vs. constant (RUQ pain → hepatitis/choledochal cyst)
- Abdominal distension, bloating
- Pale stools / dark urine (cholestasis)
- Diarrhea
Hematological symptoms:
- Pallor (anemia from hemolysis)
- Passage of dark urine (hemoglobinuria in hemolysis)
- Easy bruising, bleeding from gums/skin (coagulopathy in liver failure)
General:
- Weight loss, failure to thrive
- Rash, skin lesions (viral exanthem, purpura)
- Swelling of limbs or abdomen (ascites from portal hypertension)
- Change in behavior/altered sensorium → hepatic encephalopathy
Neurological (in 4-year-old):
- Regression of milestones (Wilson disease, metabolic disorders)
- Tremors, behavioral changes (Wilson)
A — Aggravating Factors
- Does eating fatty foods worsen the pain/symptoms?
- Does exposure to certain foods trigger episodes? (fava beans in G6PD deficiency)
- Any medications taken (drugs causing cholestatic or hepatocellular jaundice)?
- Physical exertion worsening pallor or jaundice (hemolytic crisis)?
R — Relieving Factors
- Is the jaundice improving with rest or hydration?
- Has any treatment been started (traditional/herbal medicines, antibiotics)?
- Any visit to a doctor before this? If yes, what was given and did it help?
T — Temporal Pattern / Time Course
- Is it continuous or intermittent/episodic?
- Does it come and go with illness (e.g., intercurrent infections triggering hemolytic crisis in G6PD)?
- Time of day variation?
- Relationship to meals?
- Progressive worsening over weeks → obstructive cause more likely
S — Severity
- How yellow is the child? Just eyes, or whole body?
- Is the child still eating and active, or listless/lethargic?
- Any signs that alarm the parents (bleeding, unconsciousness)?
- How is it affecting the child's daily activities?
Additional Pediatric-Specific History (Beyond OLDCAARTS)
Birth & Neonatal History
- Was there jaundice at birth or in the neonatal period?
- Was phototherapy or exchange transfusion needed?
- Birth weight, gestational age
Immunization History
- Hepatitis A and B vaccination status
Nutritional History
- Diet: vegetarian/non-vegetarian, intake of raw shellfish (hepatitis A risk)
- Any recent ingestion of mushrooms (Amanita — hepatotoxic)
Drug & Toxin History
- Medications: anti-TB drugs (INH, rifampicin), antibiotics (erythromycin), anticonvulsants (valproate, carbamazepine), acetaminophen overdose
- Herbal/traditional medicines (common in children in many settings)
Infectious Contact History
- Contact with a jaundiced person (hepatitis A outbreak — spread feco-orally)
- Animal contact (leptospirosis: rats, dogs, muddy water)
- Recent travel to endemic areas (hepatitis, malaria, dengue)
Family History
- Hereditary hemolytic anemias: G6PD deficiency, hereditary spherocytosis, thalassemia
- Metabolic liver diseases: Wilson disease, galactosemia, tyrosinemia
- Gilbert syndrome, Dubin-Johnson syndrome, Rotor syndrome
- Similar illness in siblings or parents
Socioeconomic & Environmental
- Source of drinking water (unsafe water → hepatitis A/E)
- Living conditions, sanitation
PHYSICAL EXAMINATION
1. General Examination (Opening Remarks)
Vitals (PICCLE)
- Pulse — tachycardia (fever, anemia, heart failure)
- Infection (temperature) — fever suggests infective hepatitis
- Capillary refill time
- Color (pallor, cyanosis, jaundice)
- Level of consciousness
- Edema
Anthropometry
- Height, weight — plot on growth chart (percentile)
- Grade of malnutrition (SAM/MAM)
- Head circumference if indicated
2. Jaundice Assessment
| Site | Significance |
|---|---|
| Sclera (conjunctiva) | First and most reliable site |
| Skin (face, chest, abdomen, palms, soles) | Deepness correlates with severity |
| Soft palate and undersurface of tongue | Mucosal jaundice |
| Nail beds | |
| Nasal tip |
- Depth: Lemon-yellow (mild/hemolytic) → yellow-orange (hepatocellular) → green-yellow or bronze (cholestatic/prolonged)
3. Skin Signs
| Sign | Suggests |
|---|---|
| Pallor | Hemolytic anemia |
| Petechiae / purpura | Coagulopathy, thrombocytopenia |
| Spider angiomata | Chronic liver disease (portal hypertension) |
| Caput medusae | Portal hypertension |
| Scratch marks | Pruritus (cholestasis) |
| Xanthomata | Chronic cholestasis |
| Cutaneous hemangiomata | Hepatic hemangioma |
| Kayser-Fleischer rings (eye) | Wilson disease |
| Dysmorphic features | Down syndrome (trisomy 21), Alagille syndrome |
4. Eye Examination
- Scleral icterus (jaundice)
- Pallor of conjunctiva (anemia)
- Kayser-Fleischer rings (slit-lamp: Wilson disease)
- Cataracts (galactosemia, hypoparathyroidism)
- Chorioretinitis (congenital infection)
5. Abdominal Examination (Central to Jaundice Workup)
Inspection
- Distension (ascites, organomegaly)
- Visible veins / caput medusae (portal hypertension)
- Umbilical hernia (chronic liver disease with ascites)
- Scars from prior surgery
Palpation
- Tender vs. non-tender
- Surface: smooth (hepatitis, congestion) vs. nodular (cirrhosis, storage disorders)
- Consistency: soft / firm / hard
- Liver span (percuss + palpate upper and lower borders)
- Sharp vs. rounded edge
- Size (Hackett grading I–V)
- Consistency
- Splenic notch (confirms it's spleen)
- Splenomegaly + hepatomegaly = hepatosplenomegaly → think hemolytic anemia, portal hypertension, storage disorders, infections
- Gallbladder (Courvoisier sign — not usually palpable in benign disease)
- Cystic mass in RUQ → choledochal cyst
- Kidneys
- Hernial orifices
Percussion
- Shifting dullness, fluid thrill → ascites
- Horseshoe dullness (massive ascites)
- Hepatic dullness span
Auscultation
- Renal / hepatic bruit
- Venous hum (portal hypertension)
- Absent bowel sounds (paralytic ileus in severe hepatitis)
6. Cardiovascular Examination
- Hemic murmur (hemolytic anemia)
- Signs of congestive cardiac failure (hepatomegaly can be cardiac)
- Systolic murmur + abnormal facies + embryotoxon (butterfly vertebrae) → Alagille syndrome
7. Respiratory Examination
- Pleural effusion (from hypoalbuminemia)
- Secondary pulmonary infection (hepatopulmonary syndrome)
8. CNS Examination
- Level of consciousness (hepatic encephalopathy)
- Tone, tremors (Wilson disease: wing-beating tremor)
- Developmental milestones (regression in metabolic disorders)
9. Lymph Nodes
- Generalized lymphadenopathy → infectious mononucleosis (EBV), CMV, malignancy
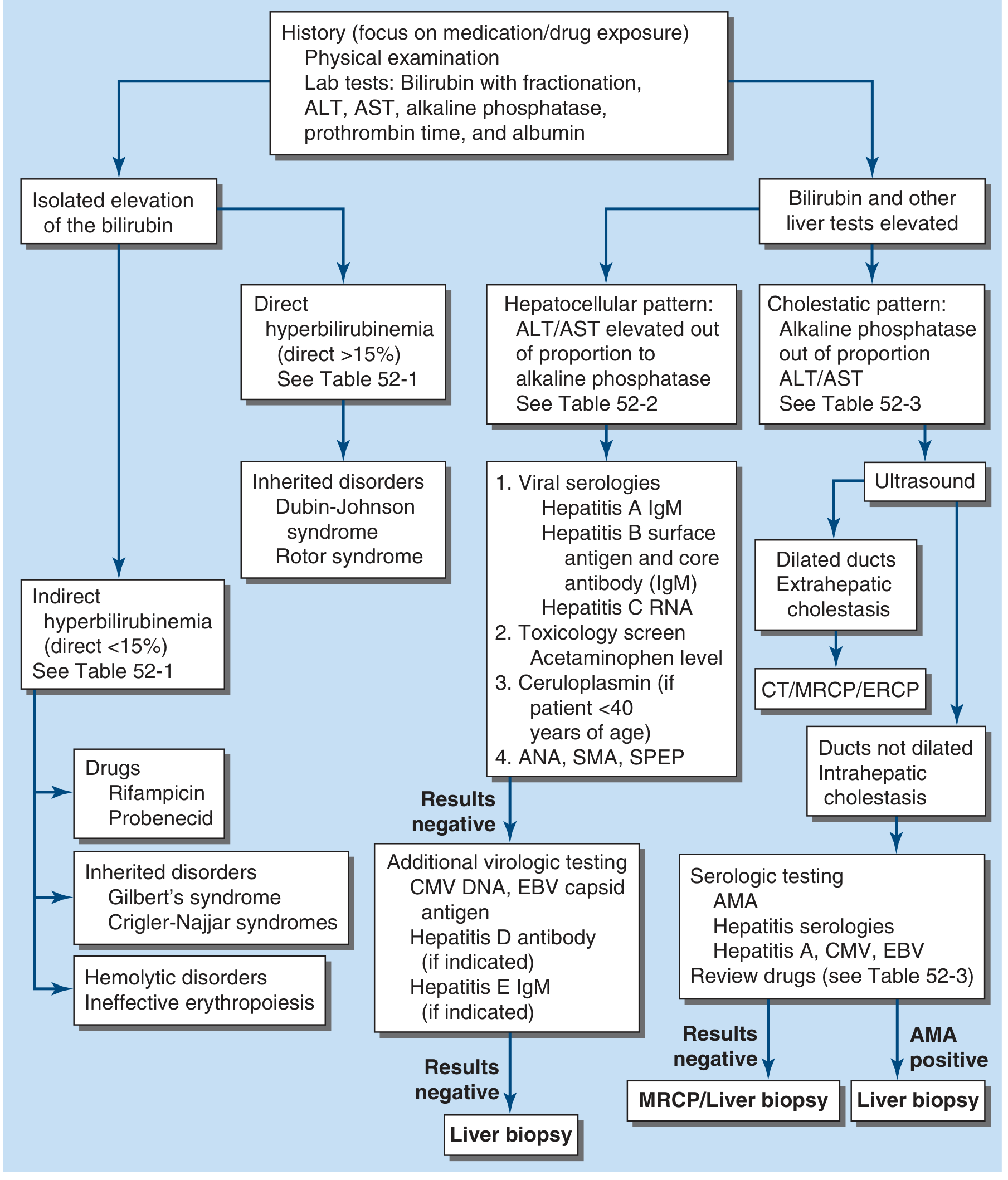
Diagnostic Flowchart (Harrison's, 2025)
Key Differentials in a 4-Year-Old with Jaundice
| Type | Causes |
|---|---|
| Prehepatic (unconjugated) | G6PD deficiency, hereditary spherocytosis, thalassemia, sickle cell disease, malaria |
| Hepatic (hepatocellular) | Hepatitis A (most common in this age), EBV, CMV, autoimmune hepatitis, Wilson disease, metabolic liver disease |
| Posthepatic (conjugated/obstructive) | Choledochal cyst, biliary stricture, gallstones, biliary atresia (late presentation) |
Initial Investigations to Order After History & Exam
- Serum bilirubin — total, direct (conjugated), indirect
- LFT: AST, ALT, ALP, GGT, albumin, PT/INR
- CBC with peripheral smear (hemolysis? spherocytes? reticulocyte count)
- Urine: bilirubin, urobilinogen, color
- Stool: color inspection
- Hepatitis A IgM (most common viral cause in 4-year-olds)
- USG abdomen (liver size, echogenicity, biliary tree, choledochal cyst)
Pathological and physiological jaundice
physiological vs pathological jaundice neonatal differences criteria clinical features
Physiological vs Pathological Jaundice
Background: Bilirubin Metabolism (Brief)
- Red blood cell breakdown releases heme → bilirubin (unconjugated/indirect — lipophilic, albumin-bound)
- Liver conjugates it via UGT1A1 enzyme → conjugated/direct bilirubin (water-soluble) → excreted in bile
- Jaundice becomes visible when serum bilirubin rises to >1.5–3 mg/dL (>35–50 µmol/L)
- In the neonate, bilirubin previously cleared by the maternal liver across the placenta; after birth, the baby's own immature liver must take over
PHYSIOLOGICAL JAUNDICE
Definition
Mechanism (Why It Happens)
| Factor | Explanation |
|---|---|
| ↑ Bilirubin production | Neonates have higher RBC mass (Hb ~17–19 g/dL at birth) + shorter RBC lifespan (~70–90 days vs. 120 days in adults) → more heme breakdown |
| Immature UGT1A1 (glucuronosyltransferase) | Liver conjugation capacity is low at birth; matures over 1–2 weeks |
| Immature intestinal flora | Bacteria that convert bilirubin → urobilinogen are absent → increased enterohepatic circulation of unconjugated bilirubin |
| Low albumin binding capacity | Less transport protein available in neonates |
| Alternative excretory pathways | Unconjugated bilirubin passes into gut before conjugation is complete |
Clinical Features
| Feature | Term Infant | Preterm Infant |
|---|---|---|
| Onset | After 24 hours of life (usually day 2–3) | Day 2–5 |
| Peak | Day 3–5 | Day 5–7 |
| Peak bilirubin level | <12–15 mg/dL (<200–255 µmol/L) | <15–17 mg/dL |
| Resolution | By 1 week (7 days) | By 2 weeks |
| Type | Unconjugated (indirect) only | Unconjugated |
| Stool/urine color | Normal yellow stool, normal urine | Normal |
| Child's behavior | Well, feeding normally, active | — |
| Scleral icterus | Mild | Mild |
| No signs of illness | No fever, no pallor, no hepatosplenomegaly | — |
Why More Severe in Premature Infants?
PATHOLOGICAL JAUNDICE
Definition
Key Rule: Any jaundice in the first 24 hours of life = PATHOLOGICAL until proven otherwise.
Causes of Pathological Jaundice
A. Unconjugated (Indirect) Hyperbilirubinemia
| Mechanism | Causes |
|---|---|
| ↑ Bilirubin production (hemolysis) | Rh incompatibility (erythroblastosis fetalis), ABO incompatibility, G6PD deficiency, hereditary spherocytosis, pyruvate kinase deficiency, sickle cell disease, thalassemia, sepsis |
| Isoimmunization | Rh/ABO blood group antibodies from mother destroy fetal RBCs |
| Extravasated blood | Cephalhematoma, bruising, internal hemorrhage |
| ↓ Conjugation (UGT1A1 deficiency) | Crigler-Najjar syndrome type I & II, Gilbert syndrome |
| Drug inhibition of UGT1A1 | Chloramphenicol, gentamicin, novobiocin |
| Breast milk jaundice | Fatty acids in breast milk inhibit UGT1A1; starts day 4–7, can last 3–12 weeks |
| Hypothyroidism | Delayed maturation of conjugation pathways |
| Pyloric stenosis | Increased enterohepatic circulation |
| Sepsis | Multifactorial — hemolysis + impaired conjugation |
| Metabolic | Galactosemia, tyrosinemia |
B. Conjugated (Direct) Hyperbilirubinemia
| Mechanism | Causes |
|---|---|
| Biliary obstruction (extrahepatic) | Biliary atresia, choledochal cyst, biliary stricture, inspissated bile syndrome |
| Hepatocellular disease | Neonatal hepatitis (viral — CMV, rubella, HSV, HBV), TORCH infections |
| Metabolic / genetic | Alpha-1 antitrypsin deficiency, Alagille syndrome, Zellweger syndrome, Niemann-Pick |
| Total parenteral nutrition (TPN) | Cholestasis in premature infants on prolonged TPN |
Golden rule: Conjugated bilirubin >20% of total bilirubin = pathological; always investigate.
COMPARISON TABLE: Physiological vs Pathological Jaundice
| Feature | Physiological | Pathological |
|---|---|---|
| Onset | After 24 hours | Within 24 hours (or any time) |
| Duration | <7 days (term); <14 days (preterm) | >2 weeks in term; >3 weeks in preterm |
| Peak bilirubin (term) | <12–15 mg/dL | >15 mg/dL in term (>17 in preterm) |
| Rate of rise | <5 mg/dL/day | >5 mg/dL/day (>0.5 mg/dL/hr) |
| Type of bilirubin | Unconjugated only | Unconjugated AND/OR conjugated |
| Conjugated fraction | <15% of total | >20% of total = pathological |
| Stool color | Normal (yellow) | Pale/acholic (biliary obstruction) |
| Urine color | Normal | Dark/cola-colored (bilirubinuria) |
| Pallor | Absent | May be present (hemolysis, anemia) |
| Hepatosplenomegaly | Absent | May be present |
| Signs of illness | None | Fever, lethargy, poor feeding, vomiting |
| Baby's general condition | Well, active, feeding | Unwell, lethargic |
| Family history | Negative | Positive (hemolytic anemia, metabolic) |
| Treatment needed | Usually none (reassurance) | Yes (phototherapy, exchange transfusion, surgery) |
SPECIAL TYPES OF PATHOLOGICAL JAUNDICE
1. Breast Milk Jaundice
- Onset: Day 4–7; can persist 3–12 weeks
- Cause: Fatty acids and other factors in breast milk inhibit UGT1A1 conjugation + increased enterohepatic recirculation
- Bilirubin: unconjugated, rarely exceeds 20 mg/dL
- Diagnosis: jaundice clears in 24–72 hrs if breastfeeding temporarily stopped → confirms diagnosis
- Management: reassurance; rarely needs phototherapy; do NOT stop breastfeeding unless bilirubin very high
2. Breastfeeding Jaundice (Starvation Jaundice)
- Onset: Day 2–5 (early)
- Cause: Inadequate breast milk intake → dehydration → increased enterohepatic recirculation
- Different from breast milk jaundice — this is a feeding problem, not a milk composition problem
- Management: improve feeding technique, supplement if needed
3. Erythroblastosis Fetalis (Rh Incompatibility)
- Most important abnormal cause of serious neonatal jaundice (Guyton & Hall)
- Rh-positive fetus + Rh-negative mother → maternal anti-D IgG antibodies cross placenta → destroy fetal RBCs → extreme unconjugated hyperbilirubinemia
- May cause fetal death or severe anemia
KERNICTERUS (Bilirubin Encephalopathy)
- Unconjugated bilirubin is lipophilic → crosses the immature blood-brain barrier → deposits in basal ganglia, subthalamic nuclei, hippocampus, cerebellum
- Risk: bilirubin >20 mg/dL (340 µmol/L) in term infants (lower threshold in preterm/sick infants)
Clinical Stages of Acute Bilirubin Encephalopathy (BIND)
| Stage | Features |
|---|---|
| Early (1st 1–2 days) | Lethargy, hypotonia, poor suck, high-pitched cry |
| Middle | Stupor, irritability, hypertonia, retrocollis, opisthotonos, fever |
| Advanced | Deep stupor/coma, apnea, seizures, death |
Chronic Kernicterus (Sequelae)
- Athetoid cerebral palsy (basal ganglia damage)
- Sensorineural hearing loss
- Upward gaze palsy
- Intellectual impairment (variable)
MANAGEMENT SUMMARY
| Condition | Treatment |
|---|---|
| Physiological jaundice | Reassurance, adequate feeding, watch & wait |
| Mild pathological (unconjugated) | Phototherapy (blue-green light, 478 nm peak) — converts bilirubin to water-soluble photoisomers excreted in bile/urine |
| Severe pathological (unconjugated) | Exchange transfusion (double-volume) |
| Conjugated / biliary obstruction | Surgical (Kasai portoenterostomy for biliary atresia), stenting, Whipple |
| Breast milk jaundice | Temporary cessation of breastfeeding for 24–48 hrs if needed, resume after |
| Hypothyroidism | Thyroid hormone replacement |
AAP Thresholds for Phototherapy (Term Infants, Low Risk)
| Age | Phototherapy Threshold |
|---|---|
| 24 hours | ≥12 mg/dL |
| 48 hours | ≥15 mg/dL |
| 72 hours | ≥18 mg/dL |
| ≥96 hours | ≥20 mg/dL |
According to pediatrics nelson Pathological and physiological jaundice
Nelson textbook pediatrics physiological pathological neonatal jaundice criteria classification
https://repository.uobaghdad.edu.iq/user/1016099091285656275…
Nelson textbook pediatrics neonatal jaundice "physiological" "pathological" criteria 24 hours bilirubin level site:ncbi.nlm.nih.gov OR site:aap.org OR site:emedicine.medscape.com
https://emedicine.medscape.com/article/974786-overview