Tetralogy of fallot
Reading File
Finding Sources
Searching PubMed
"tetralogy of fallot"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive, well-sourced content from multiple textbooks and recent literature. Let me compose the full answer.
Tetralogy of Fallot (TOF)
Definition & Epidemiology
Tetralogy of Fallot is the most common cause of cyanotic congenital heart disease beyond infancy, accounting for approximately 5% of all congenital cardiac malformations. It is defined by four structural abnormalities that all arise from a single embryologic defect.
- Robbins & Kumar Basic Pathology, p. 273
- Rosen's Emergency Medicine, p. 3210
The Four Cardinal Features
| Feature | Details |
|---|---|
| 1. Right ventricular outflow tract (RVOT) obstruction | Usually subpulmonic (infundibular) stenosis; can be valvular or complete atresia |
| 2. Ventricular septal defect (VSD) | Large, unrestrictive, misaligned defect near the membranous septum |
| 3. Overriding aorta | Aortic valve straddles the VSD, receiving blood from both ventricles |
| 4. Right ventricular hypertrophy (RVH) | Secondary to high pressure load from RVOT obstruction |
Embryologic Basis
All four features result from a single embryologic error: anterosuperior displacement of the infundibular septum (failure of subpulmonic conus to expand), leading to abnormal septation between the pulmonary trunk and the aortic root. In essence, unequal division of the truncus arteriosus results in a small pulmonary trunk and large aortic root.
- The Developing Human, p. 847
- Robbins & Kumar, p. 283
Anatomy & Morphology (Robbins)
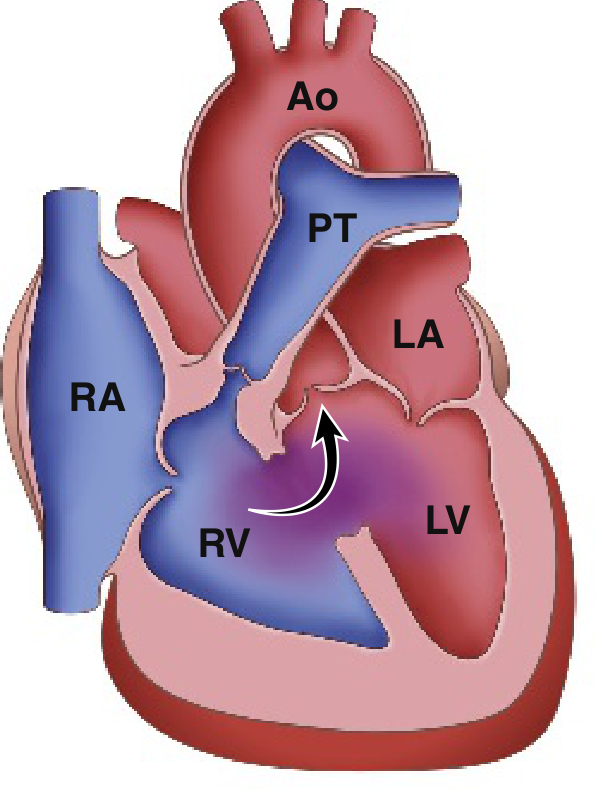
Classic Tetralogy of Fallot: note the hypoplastic pulmonary trunk (PT), enlarged right ventricle (RV), and the overriding aorta (Ao). Arrow shows right-to-left blood flow across the VSD.
- Heart is enlarged and boot-shaped on CXR (coeur en sabot) due to RVH
- Proximal aorta is dilated; pulmonary trunk is hypoplastic
- Left-sided chambers are normal in size
- RV wall is markedly hypertrophied, sometimes exceeding LV thickness
- In severe cases with pulmonary atresia, pulmonary blood flow depends entirely on a patent ductus arteriosus (PDA) or bronchial collateral vessels
Pathophysiology & Hemodynamics
The RVOT obstruction + large VSD produces a right-to-left shunt, meaning deoxygenated blood is ejected from the RV directly into the systemic circulation via the overriding aorta. This results in:
- Decreased pulmonary blood flow
- Increased aortic volume (mixed oxygenated/deoxygenated blood)
- Systemic hypoxemia and cyanosis
The severity of shunting depends on: degree of RVOT obstruction + VSD size + systemic vascular resistance (SVR).
- Rosen's Emergency Medicine, p. 3210
Clinical Features
Cyanosis Spectrum
- "Pink Tet" (acyanotic): mild RVOT obstruction → left-to-right shunt predominates → no cyanosis at birth; gradually develops cyanosis by 1-3 years
- Cyanotic TOF: severe RVOT obstruction → profound cyanosis within days of life; may require prostaglandin E1 (PGE1) infusion to keep PDA open and maintain pulmonary blood flow
Signs & Symptoms
- Cyanosis (variable degree) - worsens with crying, feeding, exertion
- Systolic ejection murmur along the left sternal border (from RVOT obstruction, not the VSD)
- Clubbing of fingers and toes (from chronic hypoxemia)
- Compensatory polycythemia (from chronic hypoxemia)
Associated Anomalies
- Right-sided aortic arch (25% of cases)
- ASD
- Anomalous origin of the left coronary artery
Investigations
| Investigation | Findings |
|---|---|
| CXR | Boot-shaped heart (coeur en sabot), decreased pulmonary vascular markings, concave main pulmonary artery segment, possible right-sided aortic arch |
| ECG | Right ventricular hypertrophy, right axis deviation |
| Echocardiography | Defines all four features; assesses degree of RVOT obstruction, coronary anatomy |
| Cardiac catheterization | Used pre-operatively in complex cases |
Tet Spells (Hypercyanotic / Hypoxic Spells)
These are potentially life-threatening acute events, most common between 2-4 months of age.
Triggering Mechanism
Any event that acutely lowers SVR (crying, defecation) or causes hypovolemia/tachycardia initiates a vicious cycle:
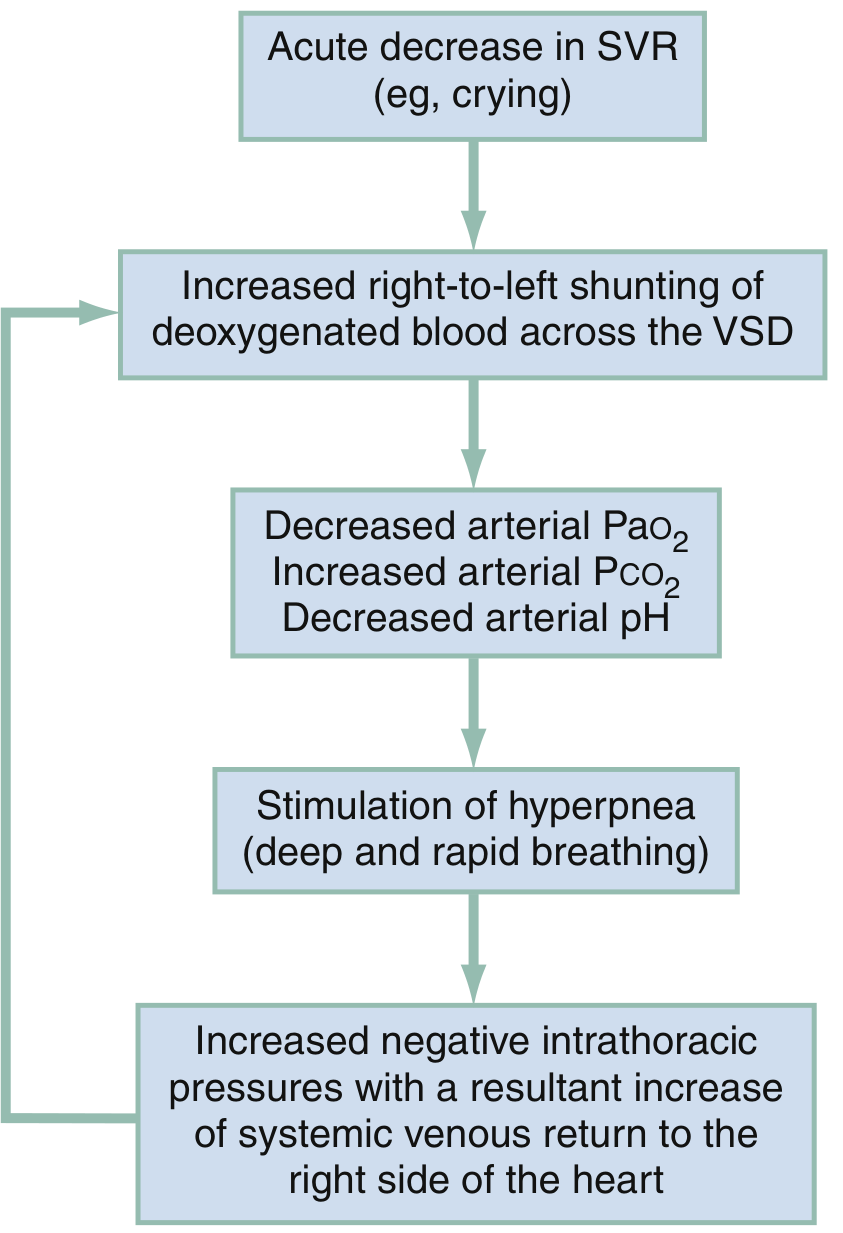
Vicious cycle of a hypoxic (tet) spell: falling SVR increases R-to-L shunting → metabolic acidosis → hyperpnea → increased venous return to RV → more shunting
Clinical Features of Tet Spell
- Hyperpnea, prolonged crying, worsening cyanosis
- Murmur diminishes (less flow through RVOT, more through VSD)
- Severe: limpness, seizures, CVA, or death
Management of Tet Spells
From Rosen's Emergency Medicine, Box 165.8:
| Step | Intervention | Rationale |
|---|---|---|
| 1st | Knee-to-chest position (infants) or squatting (older children) | Increases SVR, decreases R-to-L shunt |
| 2nd | Supplemental oxygen | Limited benefit alone, but useful adjunct |
| 3rd | Morphine 0.1-0.2 mg/kg IV/IM | Reduces hyperpnea, decreases sympathetic drive |
| Alt opioid | Fentanyl 1 µg/kg IV/IM or 1.5-2 mcg/kg intranasal | Alternative to morphine |
| Sedation | Midazolam 0.2-0.3 mg/kg intranasal | Reduces agitation |
| Acidosis | Sodium bicarbonate 1 mEq/kg IV | Corrects metabolic acidosis |
| Consider | Ketamine 1-2 mg/kg IV or 3-5 mg/kg IM | Increases SVR and provides sedation |
| Consider | Propranolol 0.1-0.2 mg/kg | Reduces infundibular spasm |
| Consider | Phenylephrine 0.01-0.02 mg/kg IV | Pure alpha-agonist - raises SVR directly |
The three treatment goals are: (1) increase SVR, (2) abolish hyperpnea, (3) correct metabolic acidosis
Definitive Surgical Treatment
- Primary surgical repair is the treatment of choice, ideally in early infancy
- Involves VSD patch closure + RVOT reconstruction (infundibulectomy ± pulmonary valvotomy)
- In severely symptomatic neonates, there is ongoing debate between primary repair vs. staged repair (palliative shunt first, then complete repair)
- A recent 2024 systematic review and meta-analysis (PMID 39444206) found no significant mortality difference between primary and staged repair in symptomatic neonates
- In pulmonary atresia variant: a Blalock-Taussig (BT) shunt or other palliative shunt may bridge until complete repair
- Del Nido cardioplegia vs. conventional blood cardioplegia is being studied; a 2025 meta-analysis (PMID 39757359) compared these approaches in TOF repair
Prognosis
- Even untreated, some patients survive into adulthood (especially "pink tets")
- With mild RVOT obstruction, presentation resembles an isolated VSD
- Post-repair adults with TOF can develop late complications (RV dysfunction, pulmonary regurgitation, arrhythmias) and require ongoing surveillance with echocardiographic deformation imaging
Sources:
This is a shared conversation. Sign in to Orris to start your own chat.