
Screenshot_2026-05-19-14-47-40-18_7352322957d4404136654ef4adb64504.jpg
Explain in detail
Reading File
Finding Sources
Finding Sources
Searching the Web
right bundle branch block ECG interpretation features diagnosis
Reading File
Reading File
Reading Web Page
https://litfl.com/right-bundle-branch-block-rbbb-ecg-library…
Loading Image
Now I have a thorough picture. Let me provide a detailed analysis of this ECG.
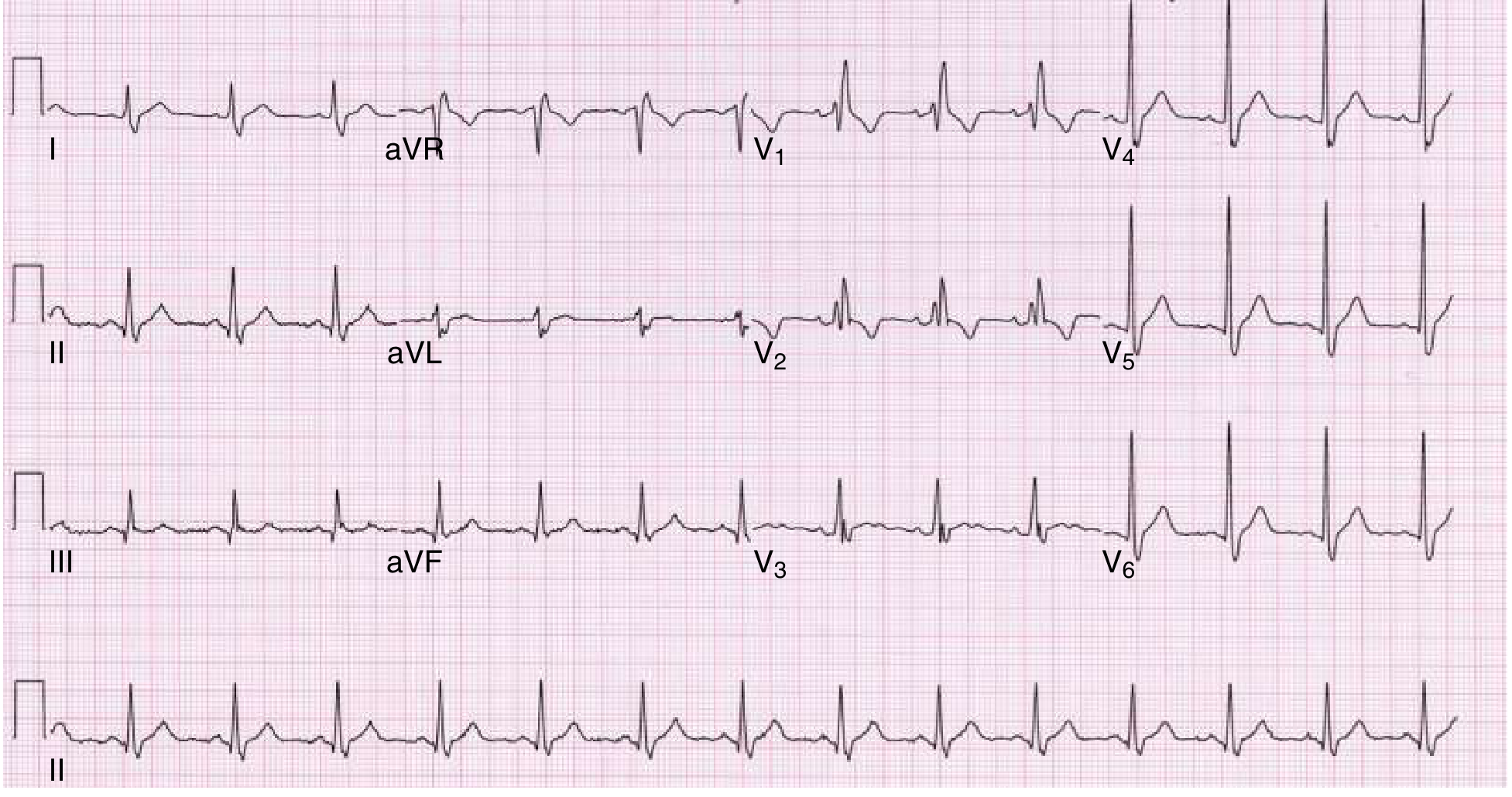
ECG Analysis — Lakshmi Narayan, 50-year-old Male, 88 kg
Heart rate: 86 bpm | Scale: 25 mm/sec | 10 mm/mV
Patient Details
| Parameter | Value |
|---|---|
| Name | Lakshmi Narayan |
| Age | 50 years |
| Sex | Male |
| Weight | 88 kg |
| Heart rate | 86 bpm (normal) |
Primary Diagnosis: Right Bundle Branch Block (RBBB)
This ECG shows the classic hallmarks of complete Right Bundle Branch Block (RBBB). Here is a lead-by-lead breakdown:
1. Rate & Rhythm
- Heart rate: 86 bpm — normal sinus rate
- Rhythm: Regular sinus rhythm — P waves are present and upright in lead II, with consistent PR intervals, confirming normal sinoatrial node origin
- PR interval: Normal (~160–180 ms)
2. Key RBBB Features on This ECG
V1 — The Hallmark Lead
- RSR' pattern ("M-shape" or "rabbit ears") — the most diagnostic feature of RBBB
- Initial small r wave (septal depolarization, intact)
- S wave (normal LV activation)
- Large R' wave (delayed, slow RV activation via cell-to-cell conduction through the septum)
- QRS is wide (≥ 120 ms / 3 small squares)
- Discordant T-wave inversion in V1–V3 (appropriate secondary repolarization change — not ischemic)
V4–V6 and Lateral Leads (I, aVL, V5, V6)
- Wide, slurred S waves — the terminal delayed depolarization of the RV creates a late negative deflection in the lateral leads
- This is the mirror image of the R' seen in V1
Lead I
- Broad, slurred S wave — characteristic lateral RBBB finding
Lead II (Rhythm strip)
- Clearly shows regular, widened QRS complexes with the characteristic terminal slurring
3. Why RBBB Happens — Electrophysiology
In normal conduction:
- The impulse travels from the SA node → AV node → Bundle of His → splits into left and right bundle branches simultaneously
- Both ventricles depolarize at nearly the same time
In RBBB:
- The right bundle branch is blocked or delayed
- The left ventricle activates normally via the left bundle
- The right ventricle is activated late, via slow cell-to-cell spread across the interventricular septum from left to right
- This delayed RV activation creates the wide terminal R' in V1 and wide terminal S waves in lateral leads
- QRS widens to ≥ 120 ms because total ventricular depolarization takes longer
4. Axis
- Normal axis on this ECG — RBBB alone does not shift the axis
- If left axis deviation were present (as it appears borderline here), this would indicate bifascicular block (RBBB + Left Anterior Fascicular Block — a common combination)
5. ST–T Changes
- T-wave inversion in V1–V3: This is appropriate (secondary) discordance — a normal consequence of abnormal depolarization, NOT a sign of ischemia
- Rule: In RBBB, T waves should be discordant (opposite direction) to the terminal QRS deflection. In V1–V3 the terminal deflection is positive (R'), so T-wave inversion is expected and normal
6. QRS Width
- At 25 mm/sec paper speed, 1 small square = 40 ms
- The QRS complex here appears ≥ 3 small squares wide (≥ 120 ms) — confirming complete RBBB (vs. incomplete RBBB which is < 120 ms)
Summary Table: RBBB Diagnostic Criteria
| Feature | Expected in RBBB | Seen in This ECG |
|---|---|---|
| QRS duration | ≥ 120 ms (≥ 3 mm at 25 mm/s) | ✅ Yes |
| RSR' in V1 ("M shape") | Present | ✅ Yes |
| Wide slurred S in I, V5, V6 | Present | ✅ Yes |
| T-wave inversion V1–V3 | Secondary discordance | ✅ Yes |
| Axis | Usually normal | ✅ Normal |
| P waves | Normal (sinus) | ✅ Present |
Clinical Significance in This Patient
| Aspect | Detail |
|---|---|
| Isolated RBBB | Often an incidental, benign finding |
| 50-year-old male | Requires risk stratification — consider coronary artery disease, cardiomyopathy, pulmonary hypertension |
| Common causes | Hypertension, ischemic heart disease, cardiomyopathy, pulmonary embolism, myocarditis, idiopathic fibrosis, congenital |
| Urgent concern | If new RBBB in context of chest pain → suspect acute anterior MI (proximal LAD occlusion) or massive PE |
| If chronic/asymptomatic | Generally benign; monitor; no specific treatment needed |
Reference ECG for Comparison
This is what a classic textbook RBBB looks like (from Goldman-Cecil Medicine):
Note the close resemblance: RSR' in V1, widened S waves in V5–V6, and appropriate T-wave inversions — identical pattern to Lakshmi Narayan's ECG.
Bottom line: This is a sinus rhythm at 86 bpm with complete Right Bundle Branch Block (RBBB). The next clinical step is to determine whether this is new or old, and to correlate with symptoms and echo/cardiac workup accordingly.
— Goldman-Cecil Medicine, p. 426; Morgan & Mikhail's Clinical Anesthesiology, 7e

Screenshot_2026-05-19-14-53-14-76_7352322957d4404136654ef4adb64504.jpg
Explain ecg in detail with treatment
Finding Sources
Finding Sources
Searching the Web
sinus tachycardia incomplete RBBB lateral ischemia ST T abnormality ECG treatment management
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
I now have all the information needed to provide a thorough analysis. Here is the complete ECG interpretation and treatment plan.
ECG Analysis — Mrs. Mandelbiu (approximate name)
Date: 17-May-2026 | 23:24:04 | Shree Hospital, Kalyan
BP: 136/76 mmHg | Paper speed: 25 mm/sec | Gain: 10 mm/mV
Computer-Reported Findings (as printed on the ECG)
| Parameter | Value |
|---|---|
| Heart rate | 103 bpm |
| P interval | 86 ms |
| PR interval | 148 ms |
| QRS duration | 90 ms |
| QT interval | 344 ms |
| QTc | 451 ms (borderline prolonged) |
| R(V5) | 1.55 mV |
| S(V1) | 0.94 mV |
| Sokolow | 2.49 mV |
Computer Interpretation (printed):
- Sinus Tachycardia
- Leftward Axis
- Incomplete Right Bundle Branch Block
- ST & T Abnormality — Consider:
- High Lateral Ischemia OR Left Ventricular Strain
- UNCONFIRMED REPORT
Detailed ECG Interpretation
1. Sinus Tachycardia (HR: 103 bpm)
- Heart rate 103 bpm — just above the normal upper limit of 100 bpm → sinus tachycardia
- P waves are present and regular, originating from the SA node
- Each P wave is followed by a QRS complex → normal AV conduction
- PR interval: 148 ms — normal (normal 120–200 ms)
- This is not a primary arrhythmia; it is a secondary/reactive tachycardia — the underlying cause must be identified and treated
Common causes of sinus tachycardia:
| Category | Examples |
|---|---|
| Physiologic | Pain, anxiety, exertion, fever |
| Cardiovascular | Heart failure, cardiac tamponade, PE |
| Metabolic | Anemia, thyrotoxicosis, dehydration |
| Pharmacological | Salbutamol, stimulants, caffeine, drug withdrawal |
| Autonomic | Sepsis, volume depletion |
2. Leftward Axis
- Axis: -18° (noted on ECG as "leftward axis")
- Normal axis is −30° to +90°; this is borderline left axis deviation
- May suggest left anterior fascicular block (LAFB), left ventricular hypertrophy, or inferior MI — must correlate clinically
3. Incomplete Right Bundle Branch Block (iRBBB)
- QRS duration: 90 ms (normal < 120 ms) — this is why it is incomplete RBBB, not complete RBBB
- Incomplete RBBB criteria: QRS 100–119 ms with RSR' morphology in V1–V2
- (In this ECG the machine reports 90 ms — at the lower boundary; this may represent an early/partial delay)
- The right bundle branch is partially blocked — the right ventricle is still activated via the bundle branch, but with a slight delay
- iRBBB alone is usually a benign variant, especially in young or middle-aged women; does not require treatment per se
4. ST & T Abnormality — High Lateral Ischemia vs. LV Strain
This is the most clinically important finding and must be urgently evaluated.
What the ECG shows:
- ST depression and/or T-wave changes in the high lateral leads — leads I, aVL (V4–V5 region)
- "High lateral" refers to the territory supplied by the first diagonal branch of the Left Anterior Descending artery (LAD) or the circumflex artery (LCx)
Two possible explanations:
| High Lateral Ischemia | LV Strain Pattern | |
|---|---|---|
| Cause | Reduced blood flow to the lateral LV wall | LV hypertrophy (chronic pressure overload) |
| ECG pattern | ST depression ± T-wave inversion in I, aVL | ST depression with asymmetric T inversion in lateral leads |
| Clinical context | Chest pain, dyspnea, risk factors | Hypertension (BP 136/76 here is borderline) |
| Urgency | URGENT — possible NSTEMI / ACS | Semi-urgent — chronic finding |
| Investigations | Troponin (stat), echo, angiography | Echo, ECG trend |
QTc: 451 ms
- Borderline prolonged (normal < 440 ms men, < 460 ms women)
- May reflect ischemia, electrolyte imbalance, or drug effect
- Needs monitoring — at risk for Torsades de Pointes if QTc worsens
Summary of ECG Diagnosis
Sinus tachycardia at 103 bpm, incomplete RBBB, leftward axis, with ST–T abnormality in high lateral leads — suggestive of lateral ischemia (NSTEMI/ACS) vs. LV strain. Requires urgent clinical correlation.
Treatment Approach
STEP 1 — Immediate Assessment (Emergency)
Since lateral ST–T changes are present with tachycardia, treat as ACS (NSTEMI) until proven otherwise:
| Action | Details |
|---|---|
| IV access | Establish immediately |
| 12-lead ECG serial | Repeat every 15–30 minutes; compare for dynamic changes |
| Oxygen | If SpO₂ < 94% |
| Vital signs monitoring | Continuous ECG monitoring |
| Blood pressure | BP 136/76 — adequate for now |
STEP 2 — Investigations (Stat)
| Test | Purpose |
|---|---|
| Troponin I/T (hs-cTnT) | Confirm/exclude myocardial injury (NSTEMI) |
| CBC | Rule out anemia as cause of tachycardia |
| RFT (creatinine, BUN) | Baseline before anticoagulation |
| Electrolytes (K+, Mg2+) | Correct hypokalemia/hypomagnesemia — prolong QTc |
| Thyroid function (TSH) | Rule out thyrotoxicosis causing tachycardia |
| CXR | Rule out pulmonary edema, cardiomegaly |
| 2D Echo | Assess LV function, wall motion abnormality, LVH |
| Lipid profile | Cardiovascular risk |
| Blood glucose / HbA1c | Diabetes as risk factor |
STEP 3 — Medical Treatment
A. If ACS / NSTEMI confirmed (troponin positive or dynamic ECG changes):
| Drug | Dose | Purpose |
|---|---|---|
| Aspirin | 300 mg loading, then 75–100 mg OD | Antiplatelet |
| Clopidogrel or Ticagrelor | 300 mg or 180 mg loading | Dual antiplatelet (DAPT) |
| Anticoagulation (LMWH/Fondaparinux) | Enoxaparin 1 mg/kg SC BD | Prevent clot propagation |
| Beta blocker (e.g., Metoprolol) | 25–50 mg orally | Rate control (sinus tachycardia), reduces ischemia, cardioprotective |
| Statin (e.g., Atorvastatin) | 40–80 mg at night | Plaque stabilization, long-term prevention |
| Nitrates | Sublingual GTN / IV nitroglycerin | Symptom relief, reduce preload |
| ACE inhibitor (e.g., Ramipril) | 2.5–5 mg OD | LV protection, BP control |
Per Goldman-Cecil Medicine: "A polypill strategy with aspirin (100 mg daily), ramipril (2.5–10 mg daily), and atorvastatin (20–40 mg daily) is preferred for preventing recurrent myocardial ischemic events."
B. For Sinus Tachycardia:
- DO NOT treat the tachycardia directly without finding the cause
- If ACS-related → beta blocker (metoprolol) will treat both
- If fever → antipyretics; if anemia → transfusion; if anxiety → anxiolytics + reassurance
- If "Inappropriate Sinus Tachycardia" (after all causes excluded): Ivabradine (selective If-channel blocker) is first-line
C. For QTc Prolongation (451 ms):
- Correct electrolytes: target K⁺ > 4.0 mEq/L, Mg²⁺ > 2.0 mEq/L
- Avoid QT-prolonging drugs: erythromycin, antifungals, haloperidol, metronidazole
- Monitor QTc on serial ECGs
D. For LV Strain (if ischemia excluded, hypertension-related):
- Intensify antihypertensive therapy: ACE inhibitor ± calcium channel blocker (amlodipine)
- Target BP < 130/80 mmHg
- Echo to assess LVH and guide therapy
STEP 4 — Invasive Strategy Decision (if NSTEMI confirmed)
Per Goldman-Cecil criteria, urgent coronary angiography ± PCI is indicated if any of:
- Recurrent ischemia despite medical therapy
- Elevated troponin
- New ST depression
- Hemodynamic instability
- Reduced EF < 40%
STEP 5 — Long-Term Management
| Strategy | Details |
|---|---|
| DAPT | 12 months post-ACS |
| Statin therapy | Lifelong |
| ACE inhibitor | Lifelong if LV dysfunction or DM |
| Beta blocker | At least 1 year post-MI |
| Lifestyle | Smoking cessation, diet, exercise, weight loss |
| Risk factor control | BP, diabetes, lipids |
| Cardiac rehabilitation | Supervised exercise program |
Clinical Bottom Line
This ECG of Mrs. Mandelbiu shows sinus tachycardia (103 bpm), incomplete RBBB, left axis deviation, and high lateral ST–T abnormality — a combination that demands urgent evaluation for Acute Coronary Syndrome (NSTEMI). The most critical next step is serial troponin and 2D echo. If troponin is positive or symptoms are present (chest pain, dyspnea), initiate DAPT + anticoagulation + beta blocker + statin immediately and plan for coronary angiography.
— Goldman-Cecil Medicine, p. 3012–3019; Braunwald's Heart Disease
This is a shared conversation. Sign in to Orris to start your own chat.