Everything about dry eye disease
"dry eye disease" AND management
dry eye disease 2025 TFOS DEWS guidelines pathophysiology treatment
Dry Eye Disease (DED) - Complete Overview
Definition
- Keratoconjunctivitis sicca (KCS) - any eye with some degree of dryness
- Xerophthalmia - dry eye associated with vitamin A deficiency
- Xerosis - extreme dryness and keratinization from severe conjunctival cicatrization
- Sjögren syndrome - autoimmune inflammatory disease of which dry eye is a prominent feature
Tear Film - The Foundation
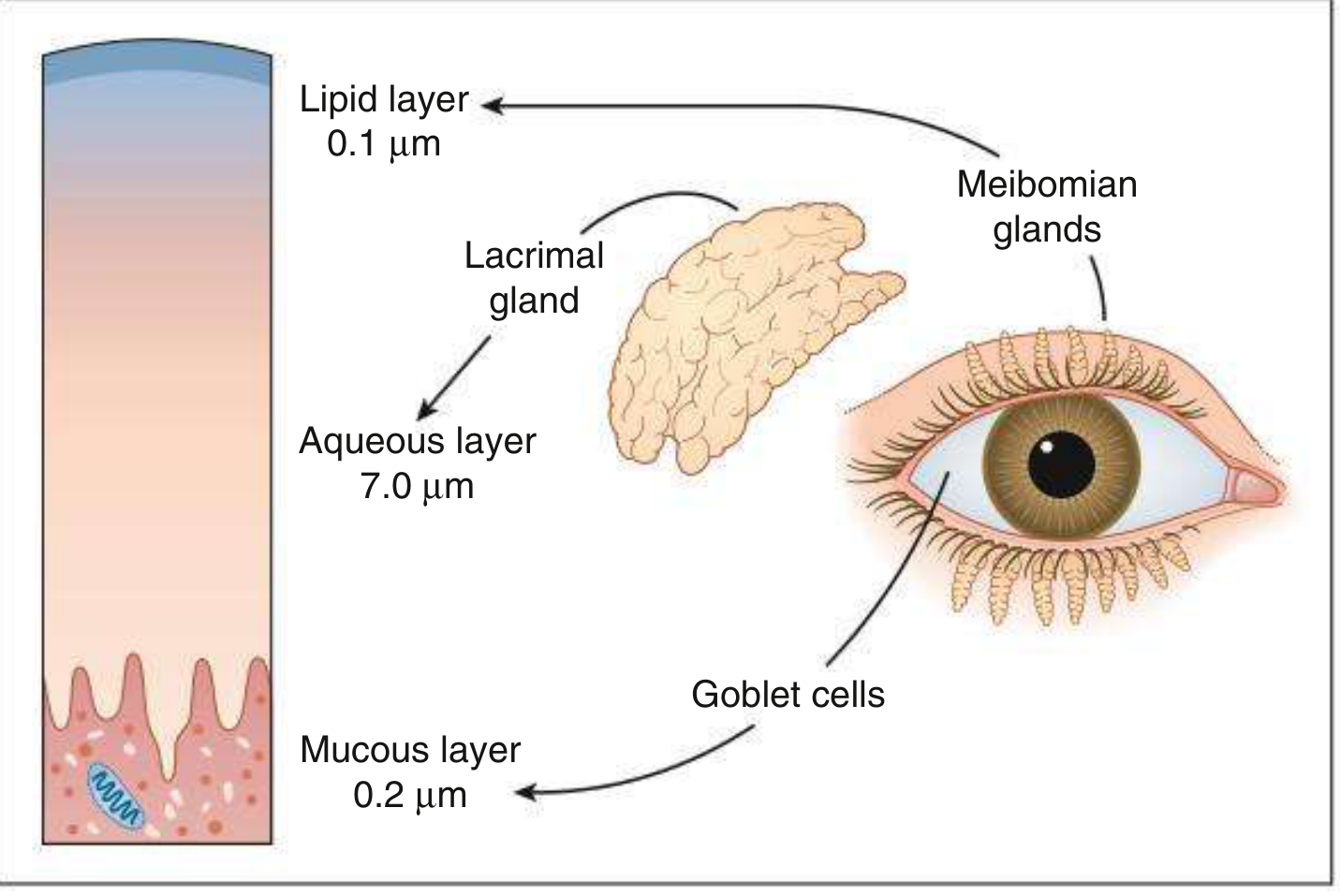
| Layer | Thickness | Source | Function |
|---|---|---|---|
| Lipid | ~0.1 µm | Meibomian glands (polar phospholipids + non-polar waxes/cholesterols) | Prevents evaporation; acts as surfactant; deficiency → evaporative DED |
| Aqueous | ~7.0 µm | Lacrimal glands (main + accessory) | Oxygen/nutrient delivery, antibacterial (lactoferrin, lysozyme, IgA), wash debris |
| Mucous | ~0.2 µm | Conjunctival goblet cells | Wets the hydrophobic epithelium; allows tear spread; deficiency → poor wetting |
- Androgens are the prime regulators of meibomian lipid production
- Oestrogen and progesterone receptors in the conjunctiva and lacrimal glands are essential for normal function
- Neural fibers adjacent to lacrimal glands and goblet cells stimulate aqueous and mucus secretion
Epidemiology
- Prevalence varies widely by diagnostic criteria: 5-50% of adults globally
- More common in women (especially postmenopausal) and the elderly
- Risk increases with: age, female sex, Asian ethnicity, low humidity environments, contact lens wear, screen use
- A 2025 systematic review found pediatric DED prevalence is also notable (PMID: 39971589)
- A 2025 meta-analysis linked diabetes mellitus to significantly increased DED risk (PMID: 40829554)
Pathophysiology
- Tear instability - rapid break-up, poor spreading
- Tear hyperosmolarity - the hallmark; results from reduced aqueous production or excessive evaporation
- Inflammation - present in ~80% of patients with KCS; both a cause AND consequence (perpetuates the cycle)
- Ocular surface damage - epithelial and goblet cell loss
Tear instability → hyperosmolarity → ocular surface damage → inflammatory cytokine release (IL-1, TNF-α, MMP-9) → lacrimal and goblet cell dysfunction → further tear instability
Classification
1. Aqueous-Deficient Dry Eye (ADDE)
- Primary or secondary (associated with rheumatoid arthritis, SLE, etc.)
- Autoimmune destruction of lacrimal and salivary glands
- Lacrimal deficiency (primary): Age-related dry eye, congenital alacrima, familial dysautonomia
- Lacrimal deficiency (secondary): Inflammatory/neoplastic lacrimal gland infiltration, AIDS, graft-versus-host disease, lacrimal gland ablation
- Lacrimal duct obstruction: Trachoma, cicatricial pemphigoid, chemical injury, Stevens-Johnson syndrome
- Reflex hyposecretion (sensory): Contact lens wear, diabetes, refractive surgery, neurotrophic keratitis
- Reflex hyposecretion (motor): CN VII damage, systemic anticholinergic drugs
2. Evaporative Dry Eye (EDE)
- Meibomian gland dysfunction (MGD) - most common cause; associated with posterior blepharitis, rosacea
- Disorders of lid aperture: excessive scleral show, lid retraction, proptosis, facial nerve palsy
- Low blink rate: Parkinson disease, computer/screen use, reading, TV watching
- Drug action: Antihistamines, beta-blockers, antispasmodics, diuretics
- Vitamin A deficiency
- Topical drugs (especially preservative effects - BAK)
- Contact lens wear
- Allergic conjunctival disease
3. Mixed/Combined
Clinical Features
Symptoms
- Burning, stinging, foreign body/gritty sensation
- Dryness, discomfort, mild-to-moderate blurred vision
- Paradoxical excess tearing (reflex hyperlacrimation)
- Worsened by: smoke, wind, heat, low humidity, AC, screen use (reduced blink rate), air travel
- Usually bilateral and chronic
- Discomfort often out of proportion to clinical signs - a hallmark feature
- Symptoms worse in the morning → evaporative type (MGD)
- Symptoms worse in the evening/after prolonged use → aqueous-deficient type
Signs
- Scanty or irregular tear meniscus (<0.25 mm height; normal ≥0.5 mm, convex shape)
- Decreased tear break-up time (TBUT) - <10 seconds indicates tear film instability
- Punctate epithelial erosions (fluorescein staining) - inferior cornea and interpalpebral area
- Conjunctival staining with rose bengal or lissamine green
- Excess mucus/debris in tear film
- Filaments (mucus+shed epithelium strands attached to cornea) - stain with rose bengal; seen in severe disease
- Mucous plaques (semi-transparent grey-white lesions) - severe cases
- Epithelial breakdown
- Corneal melting (keratolysis)
- Corneal perforation
- Bacterial keratitis (secondary infection)
Diagnosis & Investigation
| Test | What it Measures | Normal | Abnormal |
|---|---|---|---|
| Tear Break-Up Time (TBUT) | Tear film stability (fluorescein instilled, time from blink to first dry spot) | >10 sec | <10 sec |
| Schirmer's test | Aqueous tear production (filter paper in lower fornix for 5 min) | >10 mm/5 min (without anaesthetic) | <5 mm (severe), 5-10 mm (borderline) |
| Rose bengal / Lissamine green staining | Devitalized/dead epithelial cells; mucin deficiency | Absent | Inferior corneal/conjunctival staining |
| Fluorescein staining | Epithelial defects (punctate erosions) | Absent | Inferior/interpalpebral staining |
| Tear osmolarity | Osmolarity (TearLab system) | <316 mOsm/L | ≥316 mOsm/L; >8 mOsm/L inter-eye difference |
| Tear meniscometry | Volume of lower lid meniscus | 0.2-0.4 mm height | <0.25 mm |
| MMP-9 testing (InflammaDry) | Inflammatory marker in tears | Negative | Positive (>40 ng/mL) |
| Impression cytology | Goblet cell density | Normal counts | Decreased in DED |
| Meibography | Meibomian gland morphology | Normal glands | Gland dropout/truncation in MGD |
Severity Grading (DEWS)
| Grade | Discomfort | Visual symptoms | Conjunctival injection | Conjunctival staining | Corneal staining | Corneal/tear signs |
|---|---|---|---|---|---|---|
| 1 | Mild/episodic | None or mild | None/mild | None/mild | None | TBUT variable |
| 2 | Moderate/episodic to chronic | Mild | None/mild | Variable | Variable | Reduced TBUT <10s |
| 3 | Severe frequent/constant | Marked, activity-limiting | Marked | Marked | Central staining | Poor meniscus |
| 4 | Severe/disabling | Constant | Marked | Severe | Severe/erosions | Filaments |
Differential Diagnosis
- Allergic/vernal conjunctivitis
- Blepharitis (anterior) without tear deficiency
- Superior limbic keratoconjunctivitis (SLK)
- Superficial punctate keratopathy (from other causes)
- Floppy eyelid syndrome
- Neurotrophic keratitis
Treatment
Level 1 / Mild DED
- Artificial tears q.i.d. (preservative-free preferred for frequent use)
- Lifestyle modification: humidifiers, screen orientation below eye level, regular blink reminders, smoking cessation
- Environmental review: reduce AC exposure, increase humidity
- Eyelid hygiene: warm compresses, lid massage, lid scrubs for blepharitis/MGD
- Systemic medication review: eliminate anticholinergics, antihistamines, diuretics, beta-blockers if possible
- Dietary advice: omega-3 fatty acids (flaxseed oil, fish oil)
- Education about the chronic nature of the disease
Level 2 / Moderate DED
- Increase artificial tears to q1-2h; only preservative-free
- Lubricating gel or ointment at bedtime
- Cyclosporine 0.05% or 0.09% b.i.d. (Restasis, Cequa) - approved for chronic DED with inflammation; increases tear production; takes 1-3 months for full effect; burning is common early
- Co-treat with mild topical steroid (loteprednol 0.5%, fluorometholone 0.1%) b.i.d. for first month to reduce burning and hasten improvement
- Lifitegrast 5% b.i.d. (Xiidra) - LFA-1/ICAM-1 antagonist; reduces T-cell-mediated ocular surface inflammation; symptomatic improvement may be noted within 2 weeks; causes burning, transient blurring, metallic taste
- Punctal occlusion (if inflammation controlled):
- Collagen plugs (temporary, dissolve in days-weeks)
- Silicone or acrylic plugs (reversible, semi-permanent)
- Thermal cautery (permanent - use when plugs continually fall out)
- Tetracyclines (doxycycline 50-100mg/d) for MGD/rosacea-associated DED - anti-MMP activity and anti-inflammatory effects
- Topical steroids (short course) for acute inflammatory exacerbations
Level 3 / Severe DED
- All of the above, plus:
- Punctal occlusion of both lower AND upper puncta if necessary
- Autologous serum tears (20% in saline) - contains growth factors, proteins, antioxidants, lipids; formulated from patient's own blood
- Bandage soft contact lens or scleral lens - scleral lenses vault the cornea and maintain a tear reservoir
- Moisture chamber goggles/glasses (sealed at orbital rim) to reduce evaporation
- 10% acetylcysteine q.i.d. if mucus strands or filaments are present (mucolytic)
- Topical vitamin A (retinoic acid) - for goblet cell restoration
- Oral flaxseed oil / omega-3 fatty acids - anti-inflammatory lipid precursors
Level 4 / Refractory/Severe
- Tarsorrhaphy (lateral or medial) - surgical narrowing of palpebral aperture to reduce evaporation
- Temporary: adhesive tape tarsorrhaphy (tape lateral one-third closed pending surgery)
- Permanent: small lateral tarsorrhaphy if all other measures fail
- Amniotic membrane transplantation - for persistent epithelial defects
- Salivary gland autotransplantation - extreme cases of aqueous-deficient DED
- Secretagogues (pilocarpine, cevimeline) - oral muscarinic agonists to stimulate lacrimal and salivary secretion; used especially in Sjögren syndrome
Pharmacology Summary
| Drug | Class | Mechanism | Dose | Notes |
|---|---|---|---|---|
| Cyclosporine 0.05%/0.09% (Restasis/Cequa) | Calcineurin inhibitor | Inhibits T-cell activation; reduces lacrimal inflammation; increases tear production | b.i.d. | Takes 1-3 months; burning common early |
| Lifitegrast 5% (Xiidra) | Integrin antagonist | Blocks LFA-1/ICAM-1; prevents T-lymphocyte adhesion/activation | b.i.d. | Effect at 2 weeks; metallic taste, burning |
| Loteprednol / Fluorometholone | Corticosteroid | Reduces acute inflammation | b.i.d.-q.i.d. (short course) | Bridge therapy; IOP risk with prolonged use |
| Doxycycline | Tetracycline | Anti-MMP-9; anti-inflammatory; improves meibum quality | 50-100 mg/d orally | For MGD/rosacea-associated DED |
| Hydroxypropyl cellulose insert (Lacrisert) | Ocular insert | Dissolves slowly in cul-de-sac; prolongs lubrication | Once or twice daily | For moderate-severe DED |
| Pilocarpine / Cevimeline | Muscarinic agonist | Stimulates lacrimal and salivary gland secretion | Oral | Sjögren syndrome; side effects: sweating, GI upset |
Special Populations & Associations
- Sjögren syndrome: Most severe form; primary (isolated) or secondary (with RA, SLE, myositis). Oral cyclosporine, hydroxychloroquine, and rituximab for systemic disease.
- Post-refractive surgery (LASIK/PRK): Cutting corneal nerves reduces reflex lacrimation + blink frequency; can take 6-18 months to recover; pre-screen for DED risk.
- Contact lens wearers: Lens deposits alter tear film; increased evaporation; may need daily disposables or silicone hydrogel lenses.
- Diabetes: 2025 meta-analysis confirmed significant association between DM and DED risk (PMID 40829554) - corneal neuropathy reduces sensory feedback.
- Chronic pain: 2024 systematic review noted high discordance between DED signs and chronic pain comorbidity (PMID 38851945) - neuropathic component in some patients.
- Pediatric DED: Increasing with screen use; 2025 systematic review documents rising prevalence in children (PMID 39971589).
TFOS DEWS III (2025) - Latest Updates
- Pathophysiology update: Expanded from tear-film-centric to "loss of homeostasis of the entire ocular surface microenvironment" - includes neural, hormonal, and microbiome contributions
- Sex and hormones: New dedicated section on how sex, gender, and hormones influence DED
- Neuromodulation section: New pharmacological and device-based approaches to stimulate tear component production (including Alcon's Tryptyr, approved 2025)
- Updated diagnostics: Noninvasive TBUT (NITBUT), osmolarity, MMP-9 as key targeted diagnostics
- Three new treatment algorithms for tear-film deficiency subtypes
- Precision medicine approach: Match treatment mechanism to the patient's specific etiological driver(s)
- Pediatric DED and effect of patient sex on treatment efficacy identified as future research priorities
Key Takeaways
- DED is multifactorial - always identify the dominant subtype (evaporative vs. aqueous-deficient) as management differs
- The vicious circle of hyperosmolarity → inflammation → damage → instability must be interrupted at multiple points
- Inflammation is present in ~80% of KCS patients - anti-inflammatory therapy (cyclosporine, lifitegrast) is often essential
- Step up treatment systematically; address blepharitis/MGD before punctal occlusion
- Symptoms often exceed signs - take patient complaints seriously even with mild slit-lamp findings
- DED is chronic; set realistic expectations with patients about the need for long-term therapy
Meibography
meibography meibomian gland imaging
meibography technique grading scales clinical applications 2024 2025
PMID: 39383472
PMID: 41083413
https://pmc.ncbi.nlm.nih.gov/articles/PMC10164226
meibography grading scale Meiboscore Pult meibomian gland dropout scoring system infrared imaging
Meibography
Definition
Meibomian Gland Anatomy - Brief Review
- Upper eyelid: ~25-30 glands (larger tarsus, longer glands ~5-6 mm)
- Lower eyelid: ~20-25 glands (smaller tarsus, shorter glands ~3-4 mm)
- A central duct running vertically through the tarsus
- Multiple acini (lobules) budding off the central duct
- A single orifice opening onto the posterior lid margin
Technique
Historical Background
- Original meibography (1970s): Contact transillumination - a fiber-optic light source was pressed against the everted eyelid while viewing through a biomicroscope. Provided good images but was uncomfortable and limited by contact.
- Non-contact infrared meibography (Arita et al., 2008): Revolutionary development - IR illumination combined with IR-sensitive camera; eyelid is everted or the device captures through it without contact. This became the clinical standard.
How It Works
- Eyelid eversion: The upper or lower eyelid is gently everted to expose the tarsal conjunctival surface
- IR illumination: Near-infrared light (wavelength ~850-940 nm) is directed at the everted eyelid
- Image capture: An IR-sensitive CCD camera captures the transmitted/reflected image
- Gland visualization: The meibomian gland tissue appears pale/white (lipid-rich tissue transmits/reflects IR well), while areas of dropout appear dark (atrophied/absent gland tissue does not transmit)
Commercial Devices
| Device | Manufacturer | Type | Notes |
|---|---|---|---|
| LipiView II / LipiScan | Johnson & Johnson Vision (TearScience) | Non-contact IR video | Also measures blink dynamics; "Dynamic Meibomian Imager" |
| Keratograph 5M | OCULUS | Non-contact IR; slit-lamp integrated | Multifunction: also NIBUT, tear meniscus height, bulbar redness |
| Systane iLux 2 | Alcon | Non-contact IR | Combined imaging + thermal treatment |
| CA-800 Corneal Analyzer | Topcon Healthcare | Non-contact IR | Integrated with topography |
| Meibox | Box Medical Solutions | Non-contact portable | Compact, standalone |
| IDRA Ocular Surface Analyzer | SBM Sistemi | Non-contact | Multifunction ocular surface suite |
| LacryDiag | Quantel Medical | Non-contact | Combined meibography + tear film analysis |
| SL-D701 (slit-lamp adapted) | Topcon | Contact transillumination | Classic slit-lamp attachment |
Meibographic Findings
Normal Meibomian Glands
- Glands appear as elongated, parallel, white/bright strands running perpendicularly from the lid margin toward the fornix
- Regular spacing, uniform caliber, no gaps or kinking
- Full length reaching toward the fornix without truncation
Pathological Features in MGD/DED
| Finding | Description | Significance |
|---|---|---|
| Dropout (atrophy) | Partial or complete absence of gland tissue (dark areas replacing white strands) | Most clinically significant; indicates irreversible gland loss |
| Truncation | Glands end prematurely before reaching the fornix (shortened length) | Early/moderate MGD |
| Tortuosity | Glands deviate ≥45° from the midline, or show multiple bends | Associated with obstruction, fibrosis |
| Segmentation | Disjointed, discontinuous gland appearance (black lines splitting the gland) | Ductal obstruction, inflammation |
| Dilation/distension | Widened gland lumen - "dilated ducts" | Obstructive MGD with meibum stasis |
| Thickening | Increased gland diameter | Chronic inflammation, cystic dilation |
| Ghost glands | Very faint, barely visible remnants | End-stage atrophy |
| Gland reduction | Fewer glands than normal | Global atrophy |
Grading Systems
1. Meiboscore (Arita et al., 2008) - Most widely used
| Grade | Gland Loss |
|---|---|
| 0 | No loss (normal) |
| 1 | 1-33% of gland area lost |
| 2 | 34-66% of gland area lost |
| 3 | ≥67% of gland area lost |
- Graded separately for upper and lower eyelids
- Total Meiboscore = sum of upper + lower lid scores (range 0-6 per eye)
- Good repeatability; widely used in clinical trials
2. Pult 5-Grade Meiboscale (Pult et al., 2013)
| Grade | Gland Loss |
|---|---|
| 0 | No atrophy |
| 1 | <25% lost |
| 2 | 26-50% lost |
| 3 | 51-75% lost |
| 4 | >75% lost |
3. Tortuosity Grading (Halleran Scale)
- Grades the degree of gland bending/deviation
- Tortuosity defined as ≥45° deviation from midline, or multiple bends
4. LEO Segmentation Scale
- Novel scale for grading gland segmentation (discontinuous gland appearance)
5. Objective/AI-based quantification
- ImageJ software: Calculates percentage of MG area vs. total tarsal plate area
- Deep learning (DL) models: Automated segmentation, dropout quantification, meiboscore classification
- Upper lid cutoff: >16.9% area loss has sensitivity 0.889 and specificity 0.857 for diagnosing dry eye
Which Eyelid to Image?
-
Lower eyelid traditionally preferred (easier to evert, more commonly studied)
-
Upper eyelid increasingly recognized as equally or more important:
- Better inter-examiner agreement on dropout grading
- Denser, firmer tarsus → less distortion during eversion → more reliable images
- Better for longitudinal follow-up
- Some studies show upper lid meiboscore correlates better with TBUT than lower lid
- Important for early detection of Sjögren syndrome, thyroid eye disease (Gupta & Karpecki, Cornea 2025 - PMID 39383472)
-
Lower eyelid caveat: Less dense tarsus allows the lid and glands to distort more easily, potentially yielding less accurate images
Clinical Applications
1. Diagnosis of MGD
- Confirms structural gland loss when clinical signs are ambiguous
- Distinguishes obstructive MGD (glands present but dysfunctional) from atrophic MGD (glands absent)
- Identifies early-stage MGD before significant dropout develops
2. DED Subtyping
- Distinguishes evaporative (MGD-related) from aqueous-deficient DED
- Essential for directing targeted therapy
3. Disease Severity Assessment
- Correlates with TBUT, lid margin signs, and symptomatic scores (though correlation is moderate)
- Gland dropout indicates more advanced, irreversible disease
- Note: gland dropout correlates more weakly with symptoms than functional parameters (meibum expressibility, quality)
4. Treatment Monitoring
- Tracks structural response to:
- Thermal pulsation (LipiFlow, iLux) - heat + pressure to evacuate obstructed meibum
- Intense Pulsed Light (IPL) - may improve MG morphology; reports of "MG dropout score improvement" (though whether this represents true regrowth or image artifact is debated)
- Intraductal probing - mechanical opening of obstructed ducts
- Topical cyclosporine/lifitegrast - anti-inflammatory; may slow gland loss progression
- Baseline meibography allows comparison at follow-up
5. Pre-surgical Screening
- Mandatory before LASIK/refractive surgery (surgery worsens DED; pre-existing MGD increases risk)
- Before cataract surgery (optimize ocular surface pre-operatively for better outcomes and accurate biometry)
- Before contact lens fitting
6. Systemic Disease Monitoring
- Sjögren syndrome: MGD contributes to DED; upper lid meibography useful for early detection (Rheumatology, 2-Vol. Set, Elsevier)
- Thyroid eye disease (TED): Lid retraction → increased evaporation → MGD secondary changes
- Rosacea: Posterior blepharitis → MGD; monitor gland status
- Isotretinoin therapy: Known to cause severe MGD - baseline and monitoring meibography recommended (Goodman & Gilman's)
- Demodex infestation: Meibomian gland inflammation and secondary dropout
7. Pediatric Considerations
- A 2025 review (PMID 40600588) characterized MG morphology in children - important given rising screen use and pediatric DED
Meibography + Other Imaging Technologies
| Technology | What it Shows | Advantage vs. Meibography |
|---|---|---|
| IR meibography | Gland morphology, dropout (macro-level) | Clinical standard; fast; widely available |
| In vivo confocal microscopy (IVCM) | Cellular detail: acinar cells, ductal epithelium, inflammatory cells | Better for pathogenesis research; slow; expensive |
| Anterior segment OCT | Gland cross-section, ductal anatomy, tarsus thickness | Quantitative depth information; emerging |
| Tear film interferometry | Lipid layer thickness and spread | Functional complement to structural meibography |
| Meibum expressibility | Gland function (not structure) | Correlates better with symptoms than dropout |
AI and Automation in Meibography
- Deep learning (DL) segmentation - automated gland boundary delineation; removes need for manual tracing
- Automated dropout quantification - DL models achieve ~73% accuracy for meiboscore classification, comparable to MGD experts
- Generative adversarial networks (GANs) - used to remove specular reflections from IR images that interfere with analysis
- Morphometric analysis: AI can simultaneously quantify dropout, tortuosity, segmentation, density, and gland count from a single image
- Limitations: Limited dataset diversity, lack of standardized image quality control, poor generalizability across devices, regional gland variation not well modeled
Limitations of Meibography
- Poor symptom-sign correlation: Dropout is an advanced marker - patients with significant gland loss may have tolerable symptoms; early dysfunction may cause severe symptoms with minimal structural change
- Eyelid eversion artifact: Lower lid distortion can reduce image reliability
- No functional information: Structural dropout alone does not tell you about meibum quality
- Inter-observer variability: Manual grading has moderate-to-substantial agreement; AI is improving this
- No standardization across devices: Different IR wavelengths and eversion techniques make cross-device comparison difficult
- Cost: Dedicated meibography devices add to practice overhead
- Cannot detect early obstructive MGD before gland loss occurs (glands may appear normal early in obstruction)
Summary
- Confirming and quantifying gland loss (dropout) beyond clinical examination
- Guiding treatment selection (structural loss → aggressive therapy warranted)
- Monitoring treatment response over time
- Pre-surgical ocular surface assessment
- Detecting systemic disease ocular involvement early
- Kanski's Clinical Ophthalmology, 10th ed.
- Rheumatology, 2-Volume Set (Elsevier, 2022)
- Gupta PK & Karpecki P. "Comprehensive Assessment of the Meibomian Glands by Meibography: Why the Upper Eyelids Matter." Cornea 2025 - PMID 39383472
- Swiderska K et al. "Advancements in artificial intelligence for meibography." Clin Exp Optom 2026 - PMID 41083413
- Arita R et al. "Noncontact infrared meibography." Ophthalmology 2008 (foundational paper)
- Contact Lens Update: Meibomian Gland Morphology Q&A
Is 27% dropout normal?
meibomian gland dropout normative values healthy population
meibomian gland dropout percentage normal healthy population age-related normative data
meibomian gland dropout age normal population Arita noncontact infrared meibography
https://www.reviewofoptometry.com/article/improve-your-under…
"meibomian gland" dropout "healthy" OR "normal subjects" percentage area loss
Arita 2008 meibography "healthy subjects" meiboscore age-related dropout percentage results
Is 27% Meibomian Gland Dropout "Normal"?
Grading Scale Placement
| Scale | Grade for 27% | Category |
|---|---|---|
| Meiboscore (Arita) | Grade 1 (1-33%) | Mild loss |
| Pult 5-grade | Grade 2 (26-50%) | Moderate loss |
What "Normal" Actually Looks Like
- 55% of normal adults had at least some meibomian gland atrophy (Meiboscore ≥1)
- Meiboscore showed a significant positive correlation with age (R=0.428, p<0.0001) in both sexes
- Younger healthy adults tend to have very low or no dropout; older adults accumulate dropout as a normal aging phenomenon
- Upper eyelid: >16.9% dropout → sensitivity 0.889, specificity 0.857 for diagnosing dry eye
- Lower eyelid: >13.7% dropout → similar diagnostic accuracy
Age Context Matters Enormously
| Age group | Expected MG dropout (general trend) |
|---|---|
| Children / Young adults (<30) | Near zero; any visible dropout is abnormal |
| Middle age (40-60) | Some mild dropout (~Grade 1) can be seen in normals |
| Older adults (>60) | Grade 1-2 dropout common; ~70% of those over 60 have MGD |
| Elderly (>80) | Grade 2-3 dropout not uncommon even in "normal" aging |
The Contact Lens Warning
Clinical Significance of 27% Dropout
- 27% dropout = pathological by objective cutoffs, regardless of symptoms
- Symptoms may be absent (subclinical MGD) or present
- The Pult cutoff (>16.9% upper lid) was specifically validated to distinguish healthy from dry eye - 27% is well above this
- Meibum expressibility (can you express meibum with gentle pressure?)
- Meibum quality (clear, cloudy, inspissated, absent?)
- TBUT - does the lipid layer dysfunction translate to tear film instability?
Bottom Line
| 27% by Pult scale | Grade 2 (moderate) - above normal |
| 27% by Meiboscore | Grade 1 (mild) - abnormal but low severity |
| vs. diagnostic cutoff | Above the ~16.9% threshold for dry eye diagnosis |
| "Normal"? | Not normal in any age group by evidence-based cutoffs; may be expected (but not healthy) in older adults |
| Clinical action | Warrants treatment directed at preserving remaining glands; document as baseline for follow-up |