Excellent - I have both the skull X-ray image showing punched-out lesions and the bone marrow aspirate showing malignant plasma cells. Now I have everything needed for a comprehensive answer.
MULTIPLE MYELOMA
15-Mark Long Answer | Based on Standard Medicine Textbooks (Archith Boloor / Harrison's / Robbins / Goldman-Cecil)
CASE SUMMARY
A 65-year-old male with severe back pain, fatigue, recurrent respiratory infections, weight loss, anaemia (Hb 8.2 g/dL), markedly elevated ESR (120 mm/hr), hypercalcaemia, elevated creatinine, and skull X-ray showing punched-out lesions. This is a classic presentation of Multiple Myeloma.
NORMAL REFERENCE VALUES
| Parameter | Normal Value | Patient Value |
|---|
| Haemoglobin (Male) | 13.5 - 17.5 g/dL | 8.2 g/dL (LOW) |
| ESR | 0 - 20 mm/hr (Westergren) | 120 mm/hr (HIGH) |
| Serum Calcium | 8.5 - 10.5 mg/dL | Elevated |
| Serum Creatinine | 0.6 - 1.2 mg/dL | Elevated |
| Serum Total Protein | 6 - 8 g/dL | Elevated (M protein) |
| Serum Albumin | 3.5 - 5 g/dL | Often low in myeloma |
| Bone Marrow Plasma Cells | < 5% | >10% (diagnostic) |
(a) DIAGNOSIS [2 Marks]
1. Multiple Myeloma (MM)
Definition: Multiple myeloma is a malignancy of clonal plasma cells (derived from post-germinal centre B lymphocytes) that accumulate in the bone marrow, secrete a monoclonal immunoglobulin (M protein), and cause organ damage.
Basis for diagnosis in this case:
| Feature | Significance |
|---|
| Severe back pain, punched-out skull lesions | Osteolytic bone disease from plasma cell infiltration |
| Hb 8.2 g/dL (normocytic normochromic anaemia) | Marrow replacement by plasma cells |
| ESR 120 mm/hr | Elevated due to high serum M protein (rouleaux formation) |
| Elevated serum calcium | Osteoclast activation by myeloma cells releasing RANKL |
| Elevated creatinine | Myeloma kidney from Bence Jones protein cast nephropathy |
| Recurrent infections | Suppression of normal immunoglobulin synthesis |
| Age 65, male | Typical demographic (median age at diagnosis ~65 years) |
The clinicopathologic diagnosis relies on identification of clonal plasma cells in the marrow plus the presence of CRAB criteria (Robbins Pathologic Basis of Disease).
(b) CRAB CRITERIA [3 Marks]
CRAB is the mnemonic used to define myeloma-defining end-organ damage. Its presence distinguishes symptomatic (active) myeloma requiring treatment from MGUS or smouldering myeloma.
C - hyperCalcaemia
- Serum calcium > 11 mg/dL (or > 1 mg/dL above upper normal limit)
- Mechanism: Malignant plasma cells secrete osteoclast-activating factors and increase RANKL (receptor activator of nuclear factor κB ligand) in the bone marrow. RANKL induces osteoclast differentiation and activation, leading to massive bone resorption and release of calcium into the blood. Simultaneously, myeloma cells inhibit osteoblast differentiation.
- Clinical features: Confusion, weakness, lethargy, constipation, polyuria, polydipsia, nausea, vomiting ("bones, moans, groans, psychic overtones").
- This patient: Serum calcium elevated - C criterion met.
R - Renal insufficiency
- Serum creatinine > 2 mg/dL (or eGFR < 40 mL/min)
- Mechanism: The most important cause is light chain cast nephropathy (myeloma kidney) - excess monoclonal free light chains (Bence Jones proteins) are filtered, precipitate in distal tubules with Tamm-Horsfall protein, and form obstructing casts that are toxic to renal tubular epithelial cells. Other causes include:
- Hypercalcaemia-induced nephrocalcinosis
- AL amyloidosis depositing in glomeruli
- Hyperuricaemia and urate nephropathy
- Direct plasma cell infiltration of kidney (rare)
- This patient: Creatinine elevated - R criterion met.
A - Anaemia
- Haemoglobin < 10 g/dL or > 2 g/dL below lower normal limit
- Mechanism:
- Replacement of normal marrow by neoplastic plasma cells - reduces erythropoiesis
- Suppression of erythropoietin production (from renal failure)
- Chronic disease (inflammatory cytokines like IL-6 suppress iron utilisation)
- Haemolysis (accelerated RBC destruction)
- Anaemia is normocytic normochromic in most patients; peripheral smear may show rouleaux formation due to elevated M protein causing RBCs to stack like coins.
- This patient: Hb 8.2 g/dL - A criterion met.
B - Bone lesions
- Lytic bone lesions, osteoporosis, or pathological fractures on imaging
- Mechanism: Plasma cells secrete cytokines (IL-1β, TNF-α, IL-6, MIP-1α) that activate osteoclasts via RANKL pathway while simultaneously suppressing osteoblast activity. This results in net bone destruction without new bone formation - hence bone scans are often NEGATIVE (no new bone formation; unlike metastatic cancer).
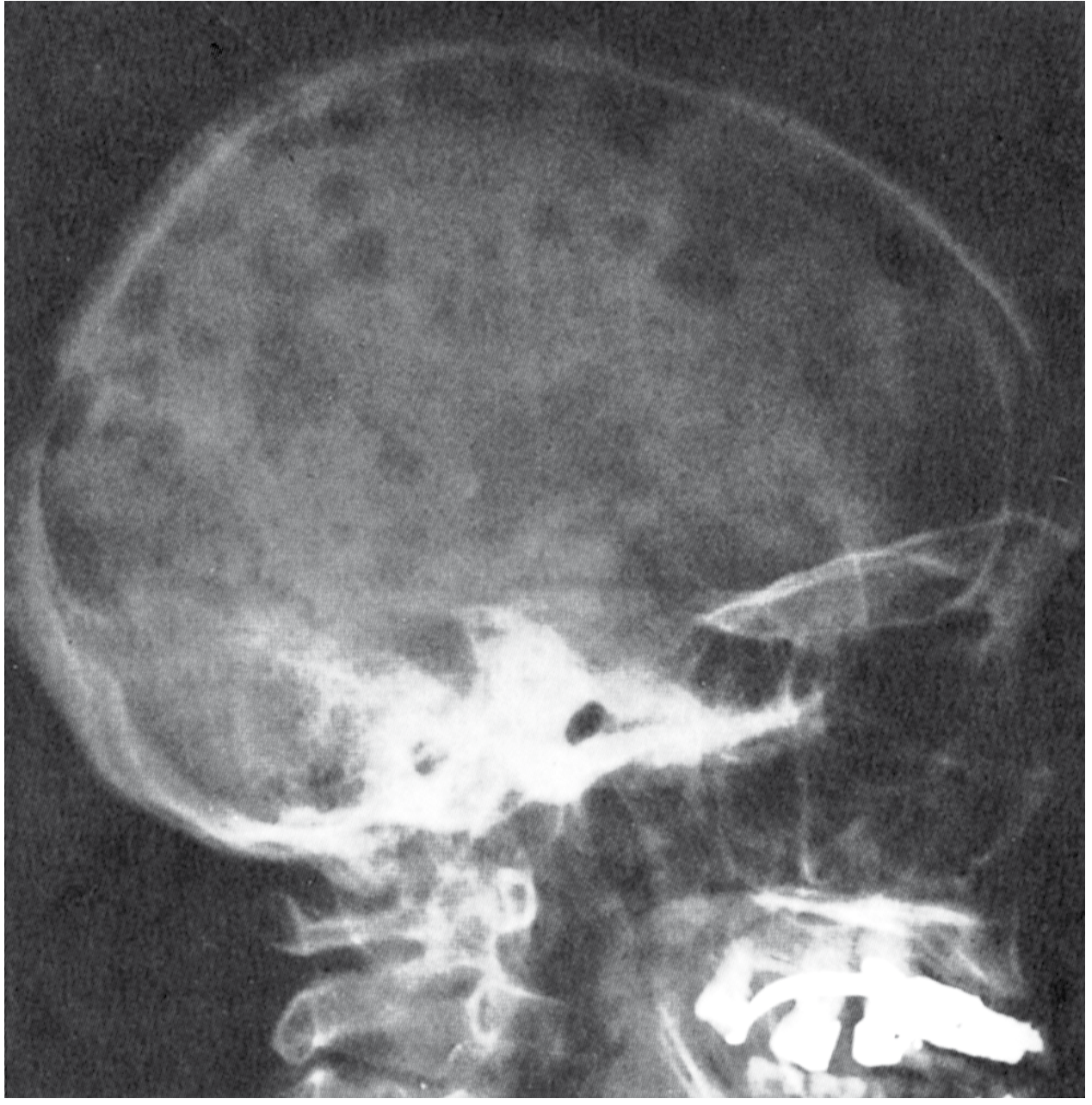
- Classic radiological finding: "Punched-out" (raindrop) lytic lesions - sharply defined, without a sclerotic rim - most prominent in skull calvaria, vertebrae, ribs, pelvis, and proximal long bones.
- This patient: Punched-out skull lesions - B criterion met.
This patient satisfies all 4 CRAB criteria, confirming symptomatic multiple myeloma requiring treatment.
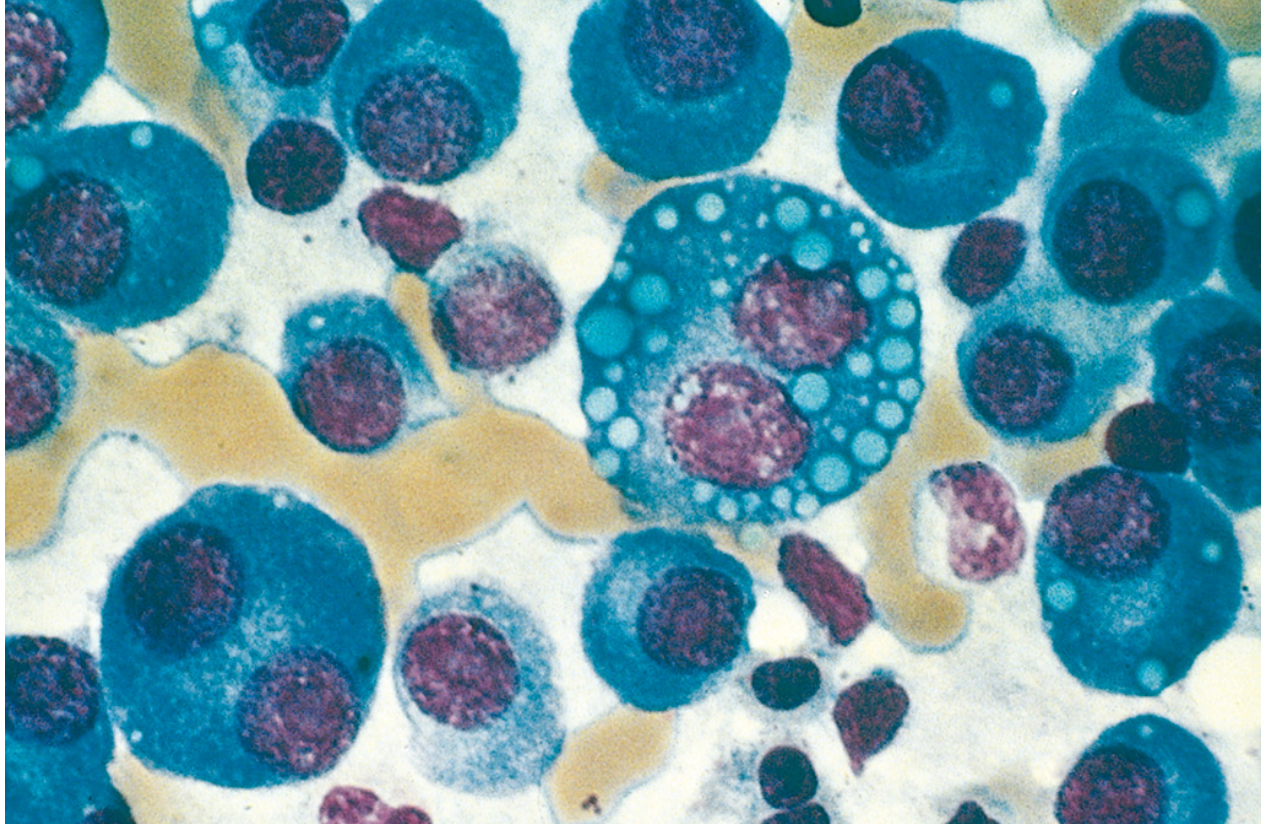
Textbook Images from Robbins Pathologic Basis of Disease:
Fig. Multiple myeloma of the skull (radiograph, lateral view) - sharply punched-out bone lesions most obvious in the calvaria.
Fig. Multiple myeloma (bone marrow aspirate) - normal marrow cells largely replaced by plasma cells including forms with multiple nuclei, prominent nucleoli, and cytoplasmic Ig droplets (Russell bodies, Mott cells).
(c) INVESTIGATIONS [4 Marks]
1. Blood Investigations
| Test | Expected Finding | Significance |
|---|
| CBC with differential | Normocytic normochromic anaemia, leucopenia, thrombocytopenia (pancytopenia) | Marrow replacement |
| ESR | Markedly elevated (>100 mm/hr) | Due to M protein causing rouleaux |
| Peripheral smear | Rouleaux formation (RBCs stacked like coins), occasional plasma cells | Characteristic of high M protein |
| Serum calcium | Elevated (hypercalcaemia) | Osteoclast activation |
| Serum creatinine / BUN | Elevated | Myeloma kidney |
| LDH, beta-2 microglobulin | Elevated | Tumour burden, staging (ISS) |
| Serum albumin | Decreased | Displacement by M protein, poor nutrition |
| Uric acid | Elevated | Cell turnover |
| Serum LFT, coagulation | Baseline; coagulopathy if amyloid or hyperviscosity | |
2. Protein Studies (M Protein Detection) - KEY INVESTIGATION
- Serum Protein Electrophoresis (SPEP): Shows a tall, narrow M spike (monoclonal spike) in the gamma globulin region (80% of patients). M protein is IgG in 52%, IgA in 21%, light chain only in 16%, IgD in 2%.
- Serum Immunofixation Electrophoresis (IFE): More sensitive (detects M protein in 93% of patients); characterises the heavy and light chain type. Gold standard for M protein identification.
- Urine protein electrophoresis + immunofixation: Detects Bence Jones protein (free light chains - κ or λ) in urine; combined with serum studies detects M protein in 97% of myeloma patients.
- Serum Free Light Chain (FLC) assay: Measures free κ and λ light chains; useful for non-secretory myeloma, monitoring, and prognosis. Abnormal κ:λ ratio (>4:1 or <1:2) indicates clonality.
Threshold: Most myelomas have > 3 g/dL of serum M protein and/or > 6 mg/dL of urine Bence Jones protein.
3. Bone Marrow Examination (Diagnostic Standard)
- Bone Marrow Aspiration + Trephine Biopsy
- Clonal plasma cells ≥ 10% of nucleated cells (in 96% of patients)
- Plasma cells show eccentric nucleus, perinuclear clearing (clockface/cartwheel chromatin), prominent nucleolus
- Special variants: Flame cells (fiery red cytoplasm), Mott cells (grape-like cytoplasmic Ig droplets), Russell bodies (cytoplasmic Ig globules), Dutcher bodies (nuclear Ig inclusions)
- Immunophenotype: CD138+, CD38+, CD56+, CD45-, CD19-, cytoplasmic Ig κ or λ (clonal)
- Abnormal κ:λ ratio confirms clonality
4. Imaging Studies
| Modality | Finding | When to Use |
|---|
| Skeletal survey (X-rays) | Punched-out lytic lesions (skull, spine, ribs, pelvis), vertebral crush fractures, generalised osteoporosis | First-line, widely available |
| Whole-body low-dose CT (WBLDCT) | More sensitive than X-ray; detects early lytic lesions | Preferred if available |
| MRI spine/whole body | Best for cord compression, soft tissue plasmacytoma, diffuse marrow infiltration | Spinal cord compression, back pain |
| PET-CT (18F-FDG) | Detects active disease, extramedullary plasmacytoma | Staging, post-treatment response |
Note: Bone scan (technetium) is typically NEGATIVE in myeloma because there is bone destruction without new bone formation (unlike metastatic carcinoma).
5. Additional / Staging Investigations
- Cytogenetics / FISH on bone marrow: t(4;14), t(14;16), del(17p) = poor prognosis; t(11;14) = intermediate; hyperdiploidy = good prognosis
- Beta-2 microglobulin (β2M) + Serum albumin: For ISS (International Staging System) staging
- Renal ultrasound: Rule out obstruction
- Echocardiogram: Screen for AL amyloidosis (cardiac involvement)
(d) TREATMENT [4 Marks]
Treatment depends on transplant eligibility (age, performance status, organ function).
Phase 1: Induction Therapy
For Transplant-Eligible Patients (younger, fit patients):
Standard: VRd (Bortezomib + Lenalidomide + Dexamethasone) - "triplet" regimen
| Drug | Dose | Schedule |
|---|
| Bortezomib (proteasome inhibitor) | 1.3 mg/m² IV or SC | Days 1, 8, 15 every 3 weeks |
| Lenalidomide (immunomodulatory drug - IMiD) | 25 mg orally | Days 1-14 every 3 weeks |
| Dexamethasone | 20 mg on day of + day after bortezomib (or 40 mg days 1, 8, 15, 22) | Per cycle |
Current preferred: Daratumumab + VRd (D-VRd) - quadruplet regimen now standard in many centres:
- Daratumumab (anti-CD38 monoclonal antibody) 16 mg/kg IV weekly × 8 weeks, then every 2 weeks × 4 months, then monthly
For Transplant-Ineligible / Elderly Patients:
-
VCd (Bortezomib + Cyclophosphamide + Dexamethasone):
- Cyclophosphamide 300 mg/m² orally on days 1, 8, 15, 22
- Bortezomib 1.3 mg/m² IV on days 1, 8, 15, 22
- Dexamethasone 40 mg orally on days 1, 8, 15, 22 - repeated every 4 weeks
-
Daratumumab + Lenalidomide + Dexamethasone (DRd) - increasingly preferred
Phase 2: Autologous Stem Cell Transplantation (ASCT)
- For transplant-eligible patients after induction achieving response
- High-dose Melphalan (200 mg/m²) as conditioning regimen followed by autologous stem cell rescue
- Significantly prolongs progression-free survival (PFS)
- Standard of care for fit patients aged <70 years
Phase 3: Maintenance Therapy
- Lenalidomide 10-15 mg/day orally - standard maintenance post-ASCT; prolongs PFS and OS
- Bortezomib ± Lenalidomide - in high-risk cytogenetics [t(4;14), del(17p)]
- Continue until progression or intolerance
Special Subtype: APL-like - t(11;14) Myeloma
- Venetoclax (BCL-2 inhibitor) has specific activity; not recommended for other cytogenetic subtypes.
Management of Complications
| Complication | Treatment |
|---|
| Bone disease | Zoledronic acid 4 mg IV monthly (bisphosphonate) - prevents skeletal events; continue for 2 years |
| Hypercalcaemia | IV hydration + Zoledronic acid + Steroids |
| Renal failure (myeloma kidney) | High urine flow maintenance (IV fluids + furosemide 100 mL/hr urine output), Plasmapheresis (if serum FLC >150 mg/dL), Bortezomib-based chemotherapy, Haemodialysis if required |
| Anaemia | Erythropoiesis-stimulating agents (EPO), RBC transfusion |
| Infections | IVIG (intravenous immunoglobulins) for recurrent bacterial infections; antibiotic prophylaxis; Pneumococcal + influenza vaccination |
| Hyperviscosity | Plasmapheresis (urgent) |
| Spinal cord compression | Emergency high-dose dexamethasone + radiation therapy (20-30 Gy) + surgical decompression |
| DVT prophylaxis | Aspirin or LMWH (especially with IMiD-based therapy; lenalidomide and thalidomide increase thrombosis risk) |
Relapsed/Refractory Myeloma (RRMM)
Newer agents used at relapse:
- Carfilzomib (next-gen proteasome inhibitor), Pomalidomide (3rd gen IMiD), Isatuximab (anti-CD38)
- CAR-T cell therapy: Idecabtagene vicleucel (ide-cel), Ciltacabtagene autoleucel (cilta-cel) - target BCMA (B-cell maturation antigen)
- Bispecific antibodies: Teclistamab (BCMA × CD3)
(e) COMPLICATIONS [2 Marks]
Major Complications of Multiple Myeloma:
1. Renal Failure (Most common cause of death after infections)
- Occurs in up to 50% of patients
- Mechanism: Light chain cast nephropathy (Bence Jones proteins precipitate in renal tubules), hypercalcaemia-induced nephrocalcinosis, AL amyloidosis (λ light chains of the λ6 and λ3 families prone to amyloid formation), hyperuricaemia, NSAIDs/contrast nephropathy.
- Myeloma kidney = obstructing casts → tubular atrophy → interstitial fibrosis → progressive renal failure
2. Infections (Leading cause of death)
- Mechanism: Suppression of normal immunoglobulin synthesis → acquired hypogammaglobulinaemia → poor humoral immunity → recurrent bacterial infections (especially encapsulated organisms: Streptococcus pneumoniae, Haemophilus influenzae, Staphylococcus aureus, gram-negative bacilli).
- Cellular immunity (T-cell) is relatively unaffected.
- Neutropenia from chemotherapy further compounds infection risk.
3. Skeletal Complications
- Pathological fractures (vertebral compression fractures most common - patient loses height)
- Spinal cord/nerve root compression - radiculopathy, paraplegia
- Bone pain (back/chest) - present in >2/3 of patients at diagnosis
4. Hypercalcaemia
- CNS effects: confusion, weakness, coma
- Cardiac arrhythmias, constipation, renal stones
5. Hyperviscosity Syndrome (~7% of patients, especially IgA and IgG3 subtypes)
- Symptoms: Headache, visual disturbances, confusion, mucosal bleeding
- Treatment: Urgent plasmapheresis
6. AL Amyloidosis
- λ light chains deposit as amyloid fibrils in heart, kidneys, nerves, tongue
- Cardiomyopathy (restrictive), nephrotic syndrome, macroglossia, peripheral neuropathy
7. Peripheral Neuropathy
- Due to amyloid deposits in nerves, or bortezomib/thalidomide toxicity
8. Plasma Cell Leukaemia
- Rare; tumour cells flood peripheral blood (>20% circulating plasma cells)
SUMMARY FLOW CHART
Old age male + Bone pain + Anaemia + Recurrent infections
↓
ESR very high + Hypercalcaemia + Renal failure + Lytic bone lesions
↓
CRAB CRITERIA → Symptomatic Multiple Myeloma
↓
Bone Marrow Biopsy (≥10% clonal plasma cells) + M spike on SPEP/IFE
↓
DIAGNOSIS CONFIRMED: Multiple Myeloma
↓
Staging (ISS/R-ISS) + Cytogenetics (FISH)
↓
Transplant Eligible?
YES → Induction (VRd/D-VRd) → ASCT → Maintenance (Lenalidomide)
NO → VCd / DRd + Supportive care
Sources:
- Robbins, Cotran & Kumar Pathologic Basis of Disease - Chapter 13: Multiple Myeloma, pp. 569-571
- Goldman-Cecil Medicine International Edition - Chapter 173: Multiple Myeloma, diagnosis, treatment dosing tables
- Harrison's Principles of Internal Medicine 22E (2025) - Chapter: Plasma Cell Disorders
- Washington Manual of Medical Therapeutics - Hematology section