Explain me the chapter 28 renal tubular reabsorption and secretion from guyton and hall physiology edition 14th
Reading File
Finding Sources
Searching the Web
Guyton Hall Medical Physiology 14th edition chapter 28 renal tubular reabsorption secretion
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive content from the chapter. Let me compile the full, detailed explanation.
Chapter 28: Renal Tubular Reabsorption and Secretion
Guyton and Hall Textbook of Medical Physiology, 14th Edition
Overview: The Core Equation
After glomerular filtrate enters the renal tubules, it flows sequentially through the proximal tubule, loop of Henle, distal tubule, collecting tubule, and collecting duct. Along the way, substances are selectively reabsorbed back into blood or secreted from blood into the lumen. The governing equation is:
Urinary Excretion = Glomerular Filtration - Tubular Reabsorption + Tubular Secretion
For most substances, reabsorption is the dominant process. Secretion is particularly important for K⁺, H⁺, and certain organic compounds.
1. Tubular Reabsorption Is Quantitatively Large and Highly Selective
The kidneys filter approximately 180 L of plasma per day, yet only 1.5 L of urine is normally excreted. This means ~99% of the filtrate is reabsorbed. Key points:
- Quantitatively massive: A 10% decrease in tubular reabsorption (from 178.5 to 160.7 L/day) would increase urine volume from 1.5 to 19.3 L/day - nearly a 13-fold increase - if GFR remained constant.
- Highly selective: Unlike glomerular filtration (which is essentially nonselective), tubular reabsorption is precise:
- Glucose and amino acids: nearly 100% reabsorbed (essentially zero in urine under normal conditions)
- Na⁺, Cl⁻, HCO₃⁻: highly reabsorbed but variable depending on body needs
- Urea and creatinine: poorly reabsorbed - excreted in large amounts
Filtration rate formula:
Filtration = GFR × Plasma Concentration
Example: Plasma glucose = 1 g/L → Filtered glucose = 180 L/day × 1 g/L = 180 g/day, all of which is normally reabsorbed.
2. Mechanisms of Reabsorption
A. Active Transport
Primary active transport moves solutes against an electrochemical gradient using energy directly from ATP hydrolysis. Key primary active transporters in the kidney include:
- Na⁺-K⁺ ATPase (most important - found throughout the renal tubule)
- H⁺ ATPase, H⁺-K⁺ ATPase, Ca²⁺ ATPase
Secondary active transport uses an ion gradient (established by primary active transport) as its energy source. Example:
- Glucose reabsorption in the proximal tubule is coupled to Na⁺ entry via Na⁺-glucose co-transporters (SGLT). The Na⁺ gradient created by basolateral Na⁺-K⁺ ATPase drives glucose in.
Water is always reabsorbed passively by osmosis - it is never actively transported.
B. Transcellular vs. Paracellular Pathways
Renal tubular cells are held together by tight junctions (containing occludin, claudins, junctional adhesion molecules):
- Transcellular pathway: through the cell itself
- Paracellular pathway: through tight junctions and intercellular spaces
There is more than a 100-fold decrease in paracellular permeability from the proximal tubule to the collecting duct. Claudins vary by segment:
- Proximal tubule claudins: facilitate paracellular salt and water reabsorption
- Thick ascending loop claudins: important for Ca²⁺ and Mg²⁺ reabsorption (regulated by the calcium-sensing receptor)
- Distal nephron claudins: form tight barriers to cation movement
3. Proximal Tubular Reabsorption
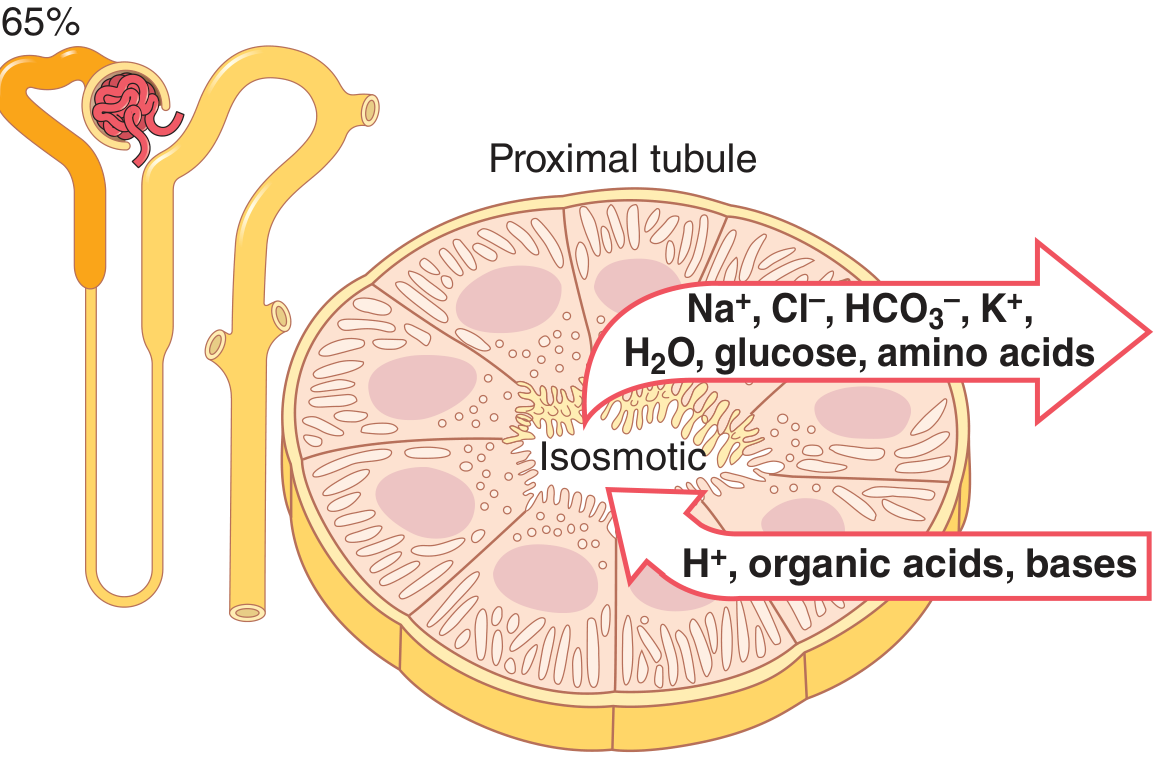
Figure 28.6 (from the text): Cellular ultrastructure and primary transport characteristics of the proximal tubule.
The proximal tubule normally reabsorbs ~65% of filtered Na⁺, water, Cl⁻, K⁺, and essentially all filtered glucose and amino acids. It also secretes organic acids, bases, and H⁺.
Why can the proximal tubule do so much?
- Cells are highly metabolic with abundant mitochondria
- Extensive brush border (microvilli) on the luminal (apical) side - vastly increases surface area
- Extensive labyrinth of intercellular and basal channels on the basolateral side
- Loaded with protein carrier molecules
Two distinct segments of the proximal tubule:
| Early Proximal Tubule | Late Proximal Tubule |
|---|---|
| Na⁺ reabsorbed with glucose, amino acids, bicarbonate via co-transport | Little glucose or amino acids remain |
| Cl⁻ ~105 mEq/L | Cl⁻ ~140 mEq/L (concentrated by preferential reabsorption of other solutes) |
| Bicarbonate reabsorption dominant | Cl⁻ diffuses passively through intercellular junctions down its gradient |
The Na⁺-K⁺ ATPase on the basolateral membrane provides the primary driving force throughout the proximal tubule. On the luminal side, Na⁺ enters via:
- Co-transport with glucose, amino acids (early segment)
- Counter-transport (Na⁺-H⁺ exchanger) - reabsorbs Na⁺ while secreting H⁺ (important for HCO₃⁻ removal)
4. Transport Maximum (Tm) - Tubular Maximum
Every carrier-mediated transport system has a maximum rate at which it can transport a substance (the transport maximum, Tm). This is because:
- At high concentrations, all carrier molecules become saturated
Glucose as the classic example:
- Normal plasma glucose: ~1 g/L → filtered load ~180 g/day → all reabsorbed (no glucose in urine)
- Tm for glucose: ~375 mg/min (approximately)
- When plasma glucose exceeds ~180-200 mg/dL (the renal threshold), filtered glucose exceeds Tm → glucose appears in urine (glycosuria)
- This is why diabetic patients spill glucose in urine
Not all substances have a sharp Tm. Some show "splay" - glucose appears in urine slightly before the theoretical Tm, because different nephrons have slightly different individual Tm values.
5. Regulation of Tubular Reabsorption
Because precise balance between tubular reabsorption and GFR is essential, multiple nervous, hormonal, and local control mechanisms regulate reabsorption.
A. Glomerulotubular Balance
The tubules have an intrinsic ability to increase reabsorption when tubular flow increases. If GFR rises from 125 to 150 mL/min, proximal reabsorption also rises proportionally (maintaining ~65% reabsorption). This prevents:
- Distal tubular overload when GFR increases
- Large fluctuations in urinary output with blood pressure changes
This occurs independently of hormones and may be due to changes in physical forces in the tubule and increased availability of ion transporters (especially the Na⁺-H⁺ exchanger) at higher flow rates.
B. Peritubular Capillary Physical Forces
The final step of reabsorption is bulk flow from the renal interstitium into peritubular capillaries. This follows the Starling forces:
| Force | Effect |
|---|---|
| Peritubular capillary hydrostatic pressure | Opposes reabsorption |
| Peritubular capillary oncotic (colloid osmotic) pressure | Favors reabsorption |
Normal peritubular capillary reabsorption rate: ~124 mL/min.
The peritubular capillary oncotic pressure is high (~32 mmHg) because fluid filtered at the glomerulus concentrates the plasma proteins. This is a key driving force for tubular reabsorption.
6. Hormonal Control of Tubular Reabsorption
Several hormones allow the kidney to excrete different solutes independently of one another:
| Hormone | Primary Site of Action | Effect on Tubular Reabsorption |
|---|---|---|
| Aldosterone | Collecting tubule and duct | ↑ NaCl, H₂O, HCO₃⁻ reabsorption; ↑ K⁺ secretion; ↑ H⁺ secretion |
| Angiotensin II | Proximal tubule, thick ascending loop, distal tubule, collecting tubule | ↑ NaCl, H₂O, HCO₃⁻ reabsorption; ↑ H⁺ secretion |
| Antidiuretic Hormone (ADH/AVP) | Distal tubule/collecting tubule and duct | ↑ H₂O reabsorption |
| Atrial Natriuretic Peptide (ANP) | Distal tubule/collecting tubule and duct | ↓ NaCl reabsorption |
| Parathyroid Hormone (PTH) | Proximal tubule, thick ascending loop, distal tubule | ↓ PO₄³⁻ reabsorption; ↑ Ca²⁺ reabsorption |
Key hormone details:
-
Aldosterone: Acts on principal cells of the cortical collecting tubule. Stimulates the Na⁺-K⁺ ATPase pump (basolateral) and increases sodium permeability of the luminal membrane by inserting epithelial sodium channels (ENaC). Also stimulates the Na⁺-Cl⁻ co-transporter in the distal convoluted tubule. Stimulated by: elevated K⁺ concentration and elevated angiotensin II.
-
Angiotensin II: A powerful promoter of Na⁺ and water reabsorption. Acts at multiple tubular segments. Important in the response to low blood pressure or volume depletion. Stimulates the Na⁺-H⁺ exchanger in the proximal tubule.
-
ADH (Vasopressin): Increases water permeability of the collecting tubule and duct by inserting aquaporin water channels (AQP2) into the luminal membrane. Allows water to follow the high osmolarity of the medullary interstitium, concentrating the urine.
-
ANP: Released by cardiac atria when blood volume/pressure is high. Directly inhibits Na⁺ reabsorption, promoting natriuresis (sodium excretion) and diuresis.
-
PTH: Inhibits phosphate reabsorption in the proximal tubule (causing phosphaturia) while stimulating Ca²⁺ reabsorption in the distal tubule and thick ascending loop.
7. Tubular Secretion
Tubular secretion adds substances from peritubular capillaries into the tubular lumen. Important secreted substances include:
- H⁺ (critically important for acid-base balance, especially in the distal nephron)
- K⁺ (regulated in the collecting tubule by aldosterone)
- Organic acids and bases (e.g., PAH - para-aminohippuric acid, many drugs and toxins)
Potassium secretion is primarily regulated in the cortical collecting tubule principal cells, where:
- K⁺ enters the cell via basolateral Na⁺-K⁺ ATPase
- K⁺ exits into the lumen through luminal K⁺ channels
Aldosterone and high plasma K⁺ both stimulate K⁺ secretion. Most of the K⁺ in the urine actually comes from secretion, not from filtered K⁺ that escaped reabsorption.
8. Calculation of Tubular Reabsorption or Secretion
Given GFR and urinary excretion, you can determine whether a substance is reabsorbed or secreted:
If Excretion < Filtered Load → Net Reabsorption If Excretion > Filtered Load → Net Secretion
Example calculation (Na⁺):
- Urine flow (V) = 1 mL/min
- Urine Na⁺ (U_Na) = 70 mEq/L = 70 μEq/mL
- Plasma Na⁺ (P_Na) = 140 μEq/mL
- GFR = 100 mL/min
Filtered load = 100 × 140 = 14,000 μEq/min
Excreted = 70 × 1 = 70 μEq/min
Reabsorbed = 14,000 - 70 = 13,930 μEq/min
Using inulin clearance as a reference (GFR = 125 mL/min):
| Substance | Clearance (mL/min) | Interpretation |
|---|---|---|
| Glucose | 0 | Completely reabsorbed |
| Sodium | 0.9 | Mostly reabsorbed |
| Chloride | 1.3 | Mostly reabsorbed |
| Potassium | 12.0 | Reabsorbed but net excretion |
| Phosphate | 25.0 | Partially reabsorbed |
| Inulin | 125.0 | Only filtered (GFR marker) |
| Creatinine | 140.0 | Filtered + some secretion |
If clearance = inulin clearance → only filtered, not reabsorbed or secreted.
If clearance < inulin clearance → net reabsorption.
If clearance > inulin clearance → net secretion (e.g., creatinine is slightly secreted).
Summary of Key Concepts
| Concept | Key Point |
|---|---|
| Core equation | Excretion = Filtration - Reabsorption + Secretion |
| Proximal tubule | Reabsorbs ~65% of Na⁺, water, Cl⁻; 100% of glucose and amino acids |
| Primary active transport | Na⁺-K⁺ ATPase powers most reabsorption |
| Secondary active transport | Na⁺-glucose co-transport (SGLT); Na⁺-amino acid co-transport |
| Transport maximum (Tm) | Carrier saturation → glycosuria above renal threshold |
| Glomerulotubular balance | Reabsorption scales with GFR intrinsically (~65% maintained) |
| Peritubular forces | High oncotic pressure drives fluid into capillaries |
| Aldosterone | ↑ Na⁺ reabsorption, ↑ K⁺ and H⁺ secretion |
| ADH | ↑ Water reabsorption via AQP2 |
| ANP | ↓ Na⁺ reabsorption (opposes aldosterone) |
| Inulin clearance | Gold standard for GFR; compares to other clearances to detect reabsorption/secretion |
Source: Guyton and Hall Textbook of Medical Physiology, 14th Edition, Chapter 28, pp. 348-369
This is a shared conversation. Sign in to Orris to start your own chat.