Physiology of placenta
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
I have very rich content from multiple textbooks. I now have enough to write a comprehensive, well-structured answer on placental physiology. Let me compile it.
Physiology of the Placenta
The placenta is a hemochorial, discoid organ derived from both fetal (chorionic) and maternal (decidual) tissues. It serves as the sole interface between mother and fetus for gas exchange, nutrient transfer, waste excretion, hormone production, and immunological tolerance.
1. Structure and Development
Chorionic Villi - the Functional Unit
The placenta develops from trophoblast cells that invade the endometrium after implantation. Three stages of villus formation occur:
| Stage | Timing | Composition |
|---|---|---|
| Primary villi | ~12-15 days post-fertilization | Syncytiotrophoblast + cytotrophoblast core |
| Secondary villi | ~Day 16 | Mesenchymal invasion into core |
| Tertiary villi | End of 3rd week | Blood vessels form in mesenchymal core |
In the mature placenta, each villus is covered by a thin syncytiotrophoblast with prominent microvilli (brush border) facing maternal blood. Beneath this lie cytotrophoblasts, mesenchyme, and fetal capillaries. The fetal blood is thus separated from maternal blood by only four layers: fetal capillary endothelium, mesenchyme, cytotrophoblast, and syncytiotrophoblast. - Medical Physiology (Boron & Boulpaep), p. 1659
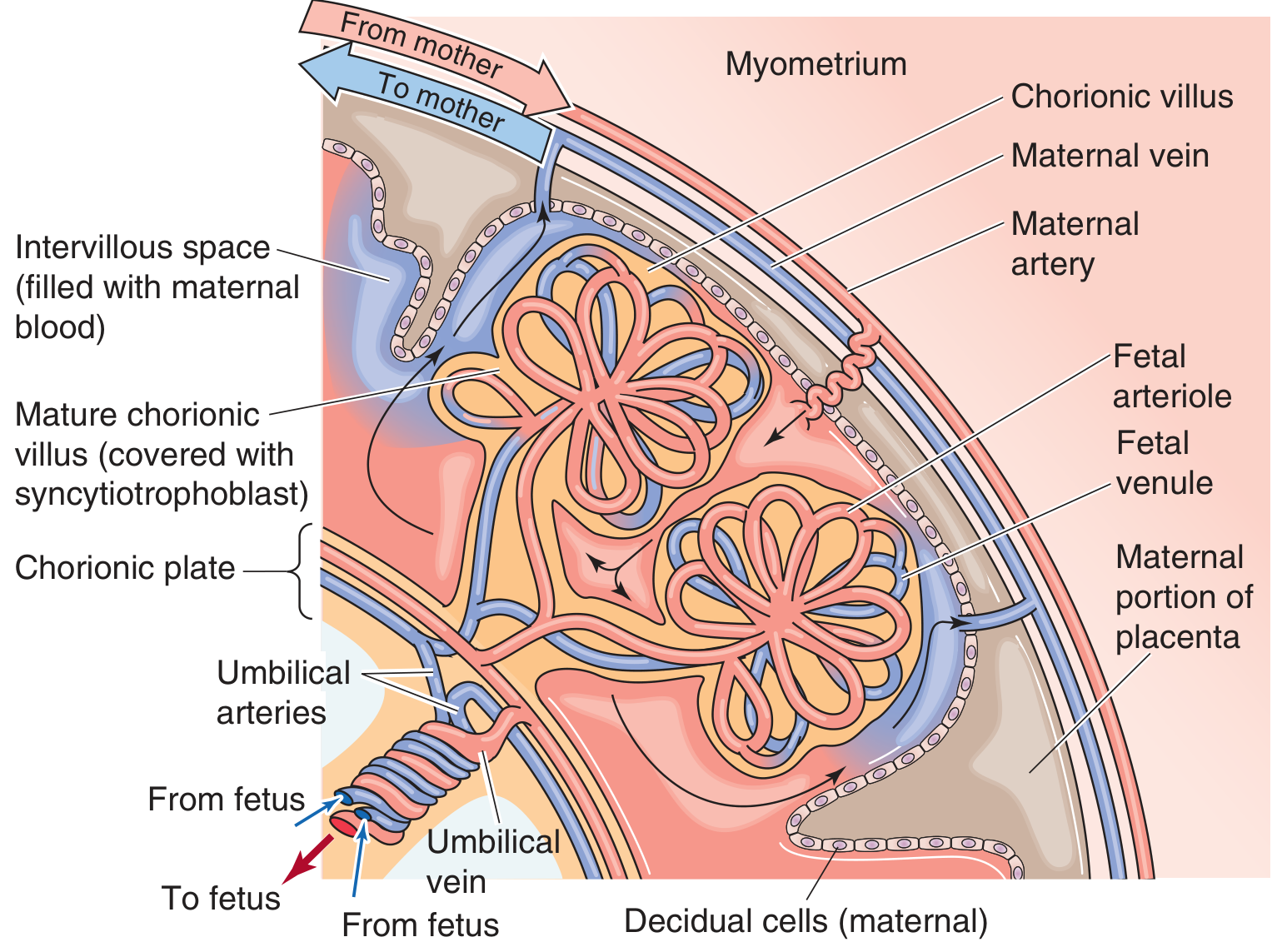
Figure: The mature placenta. Fetal umbilical arteries branch in the chorionic plate and extend into chorionic villi. Maternal spiral arteries empty into the intervillous space. Gas and nutrient exchange happens across the thin syncytiotrophoblast.
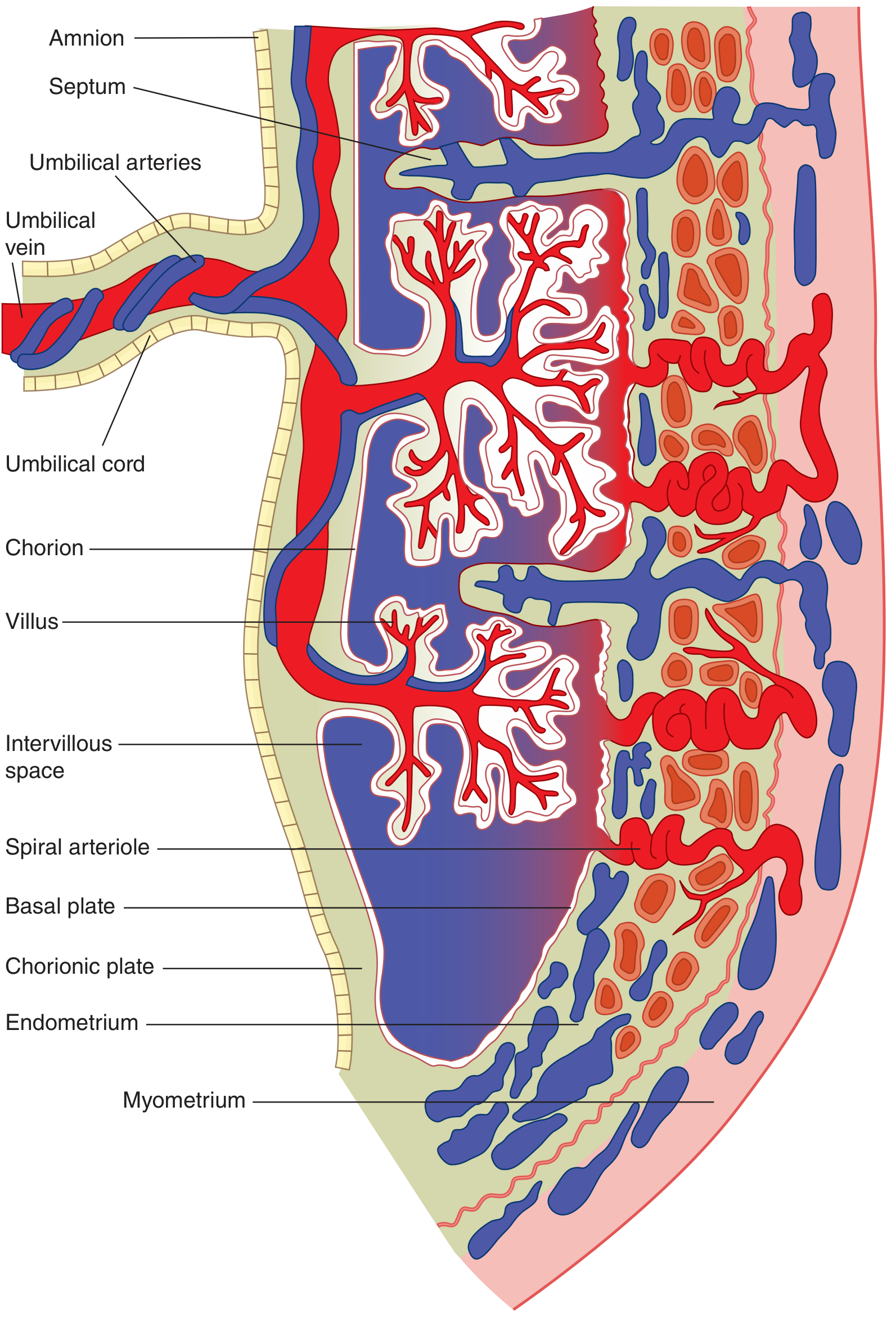
Figure: Full cross-section showing the fetal villous tree projecting into the maternal intervillous space. Note the spiral arterioles emptying into the space from the basal plate.
2. Uteroplacental Circulation
Maternal Blood Flow
- ~120 spiral arteries discharge maternal arterial blood into the intervillous space in pulsatile spurts.
- Blood enters perpendicular to the uterine wall, dissipates near the chorionic plate, then cascades over the villi and exits through venous orifices in the basal plate.
- The intervillous space is the functional capillary - there are no true capillaries between arterioles and venules on the maternal side.
- Uterine contractions increase the volume of blood in the intervillous space (by compressing veins more than arteries), ensuring continued exchange even during labor. - Medical Physiology, p. 1659
Fetal Blood Flow
- Two umbilical arteries carry deoxygenated blood from the fetus to the placenta (unique - arteries carrying deoxygenated blood).
- These branch within the chorionic villi into a dense capillary network.
- Oxygenated, nutrient-rich blood returns to the fetus via the single umbilical vein.
- Ganong's Review of Medical Physiology, 26th Ed., p. 614
3. Gas Exchange
Oxygen Transfer
The placenta is described as the "fetal lung." Oxygen moves from maternal blood in the intervillous space to fetal blood by simple diffusion down a partial pressure gradient.
| Site | PO₂ (mmHg) | Hb Saturation (%) |
|---|---|---|
| Maternal uterine artery | 100 | 97.5 |
| Intervillous space | 30-35 | 57-67 |
| Maternal uterine vein | 30 | 57 |
| Fetal umbilical arteries | 23 | 60.5 |
| Fetal umbilical vein | 30 | 85.5 |
Despite the low PO₂ in the intervillous space, the fetus achieves 85% Hb saturation via two key mechanisms:
- Fetal hemoglobin (HbF) has a higher O₂ affinity than adult HbA (the oxygen-dissociation curve is shifted left), allowing it to extract O₂ from maternal blood even at lower PO₂.
- Higher cardiac output per unit body weight and rising Hb concentration (50% higher than adult) near term increase oxygen delivery. - Medical Physiology, p. 1660
CO₂ Transfer
CO₂ moves from fetal blood (umbilical artery PCO₂ ~48 mmHg) to the intervillous space (PCO₂ ~43 mmHg) along a ~5 mmHg gradient. Fetal blood also has a lower affinity for CO₂ than maternal blood (double Bohr effect), which further favors CO₂ transfer to the mother. - Medical Physiology, p. 1660
4. Nutrient and Solute Transport
Different substances use different transport mechanisms:
| Substance | Mechanism |
|---|---|
| O₂, CO₂ | Simple diffusion |
| Glucose | Facilitated diffusion (GLUT transporters) |
| Amino acids | Secondary active transport |
| Fatty acids, steroids, fat-soluble vitamins | Simple diffusion (lipid soluble) |
| Iron, calcium | Active transport |
| Urea, creatinine (fetal waste) | Passive diffusion (fetus → mother) |
| Water-soluble vitamins, minerals | Active transport |
The syncytiotrophoblast also stores glycogen, proteins, polypeptides, and iron as reserves for poor maternal nutrition periods and the transition to extrauterine life. - Medical Physiology, p. 1661
5. Endocrine Functions
The placenta is a major endocrine organ, secreting both peptide and steroid hormones.
Peptide Hormones (key ones)
- Human chorionic gonadotropin (hCG): Secreted by syncytiotrophoblast from the earliest days of pregnancy. Its primary role is to "rescue" the corpus luteum from luteal regression, maintaining progesterone production in the first trimester. It is the basis of pregnancy tests (appears in urine ~10 days after fertilization).
- Human chorionic somatomammotropin (hCS/hPL): Also called human placental lactogen. It is anti-insulin (causes maternal insulin resistance, shunting glucose to the fetus), promotes lipolysis, and prepares mammary glands for lactation.
- Placental-variant growth hormone (pvGH): Stimulates IGF-1; may regulate fetal and placental growth.
- CRH, TRH, GnRH, GHRH: Hypothalamic-like releasing hormones; may act in an autocrine/paracrine fashion to regulate placental function.
- Inhibins: Modulate maternal gonadotropins.
Steroid Hormones and the Maternal-Placental-Fetal Unit
The placenta alone is an imperfect steroid organ - it lacks three key enzymes (17α-hydroxylase, 17,20-desmolase, 16α-hydroxylase) and cannot synthesize adequate cholesterol.
The maternal-placental-fetal unit works as a collaborative steroid factory:
| Partner | Contributes | Lacks |
|---|---|---|
| Mother | LDL cholesterol (precursor) | Adequate synthetic capacity for progesterone and estrogens |
| Placenta | 3β-HSD, aromatase, sulfatase | 17α-hydroxylase, 17,20-desmolase, 16α-hydroxylase |
| Fetal adrenal/liver | DHEA, 16α-OH-DHEA (androgen precursors), sulfating enzymes | Cannot make final estrogens alone |
- Progesterone: Maternal LDL cholesterol → placenta → progesterone. By ~8-10 weeks, the placenta takes over from the corpus luteum entirely. Progesterone reduces uterine motility and suppresses contractions.
- Estrogens (estrone, estradiol, estriol): Require collaboration. The fetal adrenal secretes DHEA-S → placenta converts it (via sulfatase and aromatase) → estrone/estradiol. Estriol (the dominant estrogen of pregnancy) requires 16α-hydroxylation in the fetal liver, so low estriol is a marker of fetal compromise.
- To protect the fetus from high steroid exposure, intermediates are sulfate-conjugated while in fetal tissues, inactivating them. The placenta sulfatase removes the sulfate when needed for conversion. - Medical Physiology, pp. 1663-1665
6. Immunological Tolerance
The fetus carries paternal antigens and should be rejected by the maternal immune system, yet pregnancy succeeds. Key mechanisms:
- Expression of HLA-G (a non-classical MHC class I molecule) by the trophoblast. Unlike HLA-A/B/C (which trigger NK cell attack), HLA-G inhibits NK cell cytotoxicity and suppresses T-cell responses.
- Fas ligand expression by trophoblast cells: Induces apoptosis in maternal lymphocytes bearing the Fas receptor that attempt to mount an attack.
- The syncytiotrophoblast forms a continuous non-antigenic barrier at the maternal interface - it does not express classical MHC antigens. - Medical Physiology, p. 1658
7. Amniotic Fluid
While not part of the placenta itself, the amniotic fluid is closely linked to placental physiology:
- Acts as a mechanical buffer protecting the fetus.
- Serves as a route for fetal excretion of waste products.
- Water turns over at least once a day.
- After fetal kidney maturation (10-12 weeks): ~75% from fetal kidneys, remainder from pulmonary secretions.
- Removal: fetal GI tract (~55%), amnion (~30%), lungs (~15%). - Medical Physiology, p. 1661
Summary: Functions of the Placenta at a Glance
| Function | Mechanism |
|---|---|
| O₂ delivery | Diffusion; HbF high affinity |
| CO₂ removal | Diffusion; double Bohr effect |
| Glucose supply | Facilitated diffusion (GLUT) |
| Amino acid supply | Secondary active transport |
| Waste removal | Passive diffusion to mother; amniotic fluid |
| Hormone production | hCG, hPL, progesterone, estrogens, CRH, etc. |
| Immune tolerance | HLA-G expression; Fas ligand; non-classical MHC |
| Nutrient storage | Glycogen, proteins, iron |
Sources: Medical Physiology (Boron & Boulpaep), Chapter 56; Ganong's Review of Medical Physiology, 26th Ed., Chapter 33; Histology: A Text and Atlas (Ross & Pawlina), Chapter 23.
This is a shared conversation. Sign in to Orris to start your own chat.