Portal hypertension anatomy physiology
Reading File
Finding Sources
Finding Sources
Searching PubMed
"portal hypertension" AND physiology
Reading File
Reading File
Reading File
Searching Images
portal venous system anatomy tributaries liver
Finding Sources
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Excellent — I now have comprehensive textbook content and all the key diagrams. Here is a thorough, well-illustrated overview:
Portal Hypertension: Anatomy & Physiology
1. Anatomy of the Portal Venous System
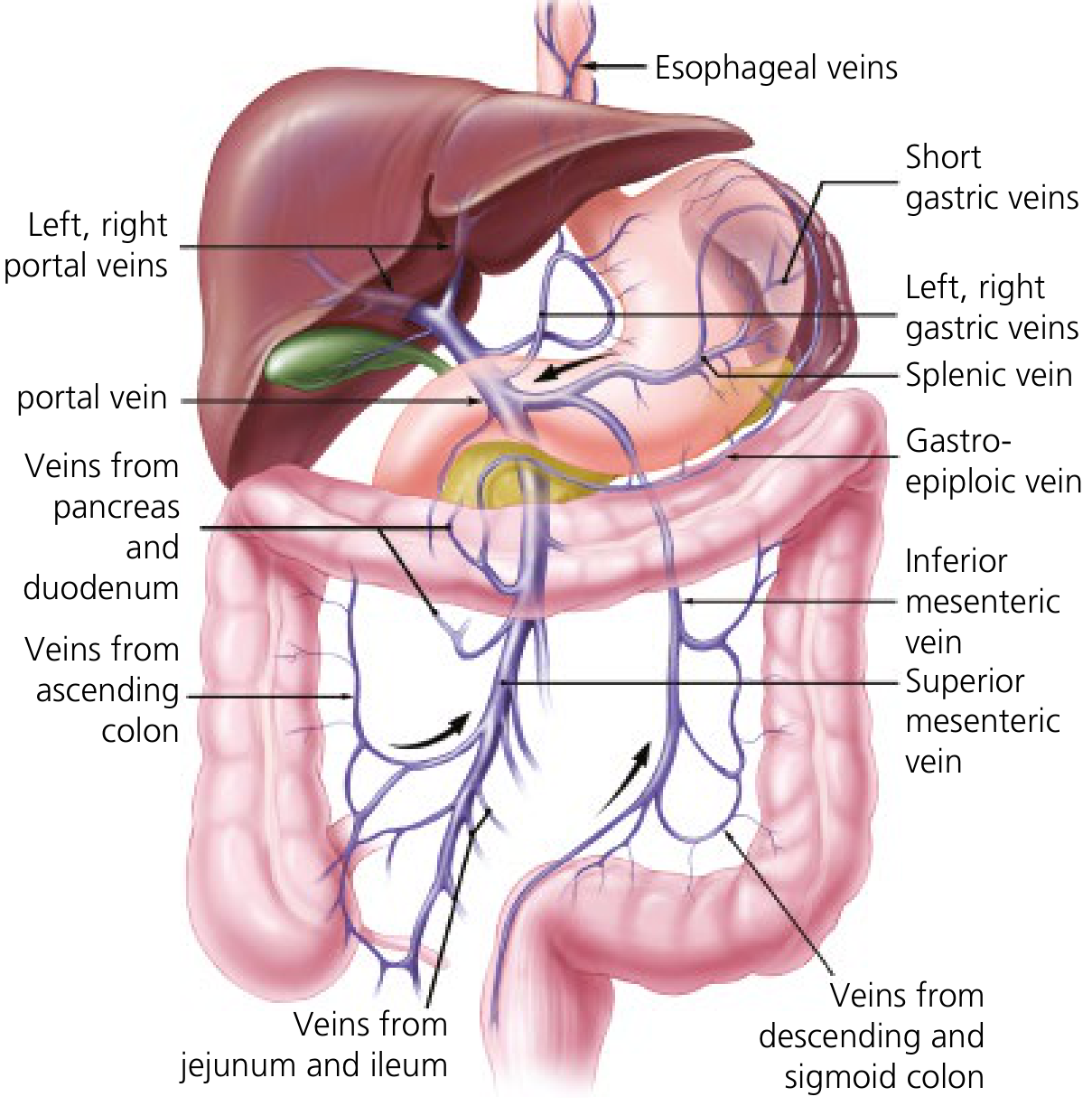
The portal vein collects blood from virtually the entire gastrointestinal tract (except the upper esophagus and distal rectum), plus the spleen, pancreas, and gallbladder.
Formation: The superior mesenteric vein (SMV) and splenic vein join posterior to the neck of the pancreas to form the main portal vein. Key tributaries:
- Left gastric vein (coronary vein) → drains at the SMV–splenic confluence
- Inferior mesenteric vein (IMV) → drains into the splenic vein
- Short gastric veins, gastro-epiploic veins → via the splenic vein
- Veins from pancreas, duodenum, jejunum, ileum, ascending and descending colon
Course: The portal vein is devoid of tributaries in its upper ~5 cm. It divides into left and right branches at the hepatic hilum. The umbilical vein (obliterated postnatally, persisting as the ligamentum teres) drains into the left portal vein. The portal vein, along with the hepatic artery and bile duct, forms the portal triad within the hepatoduodenal ligament.


2. Normal Hepatic Hemodynamics
| Parameter | Value |
|---|---|
| % of cardiac output to liver | 25–30% |
| Portal vein contribution to hepatic flow | ~75% |
| Portal vein contribution to hepatic O₂ | ~50% |
| Hepatic artery contribution | ~25% flow |
| Normal portal pressure | 5–10 mmHg |
| Portal hypertension threshold (HVPG) | ≥ 6 mmHg (clinically relevant: ≥ 10 mmHg) |
The hepatic sinusoids are highly permeable — they lack a basement membrane and have fenestrated endothelial cells. The space of Disse lies between endothelium and hepatocytes, containing hepatic stellate cells (HSCs) and Kupffer cells.
Hepatic arterial buffer response: When portal flow decreases, hepatic arterial flow compensates to maintain total hepatic blood flow at a near-constant level. The reverse (portal compensation after arterial occlusion) is more limited.
Vasoregulatory mediators:
- Nitric oxide (NO) — produced by endothelial NOS (eNOS) in response to shear stress → vasodilation
- Endothelin-1 (ET-1) — produced by endothelial cells → binds ET-A receptors on HSCs → vasoconstriction; binds ET-B receptors on endothelium → vasodilation (via eNOS)
- Others: sympathetic NS, angiotensin, prostaglandins, CO, hydrogen sulfide
3. Pathophysiology of Portal Hypertension
Portal pressure obeys Ohm's law:
Portal Pressure = Portal Flow × Vascular Resistance
Portal hypertension arises from an increase in resistance, an increase in portal blood flow, or both.
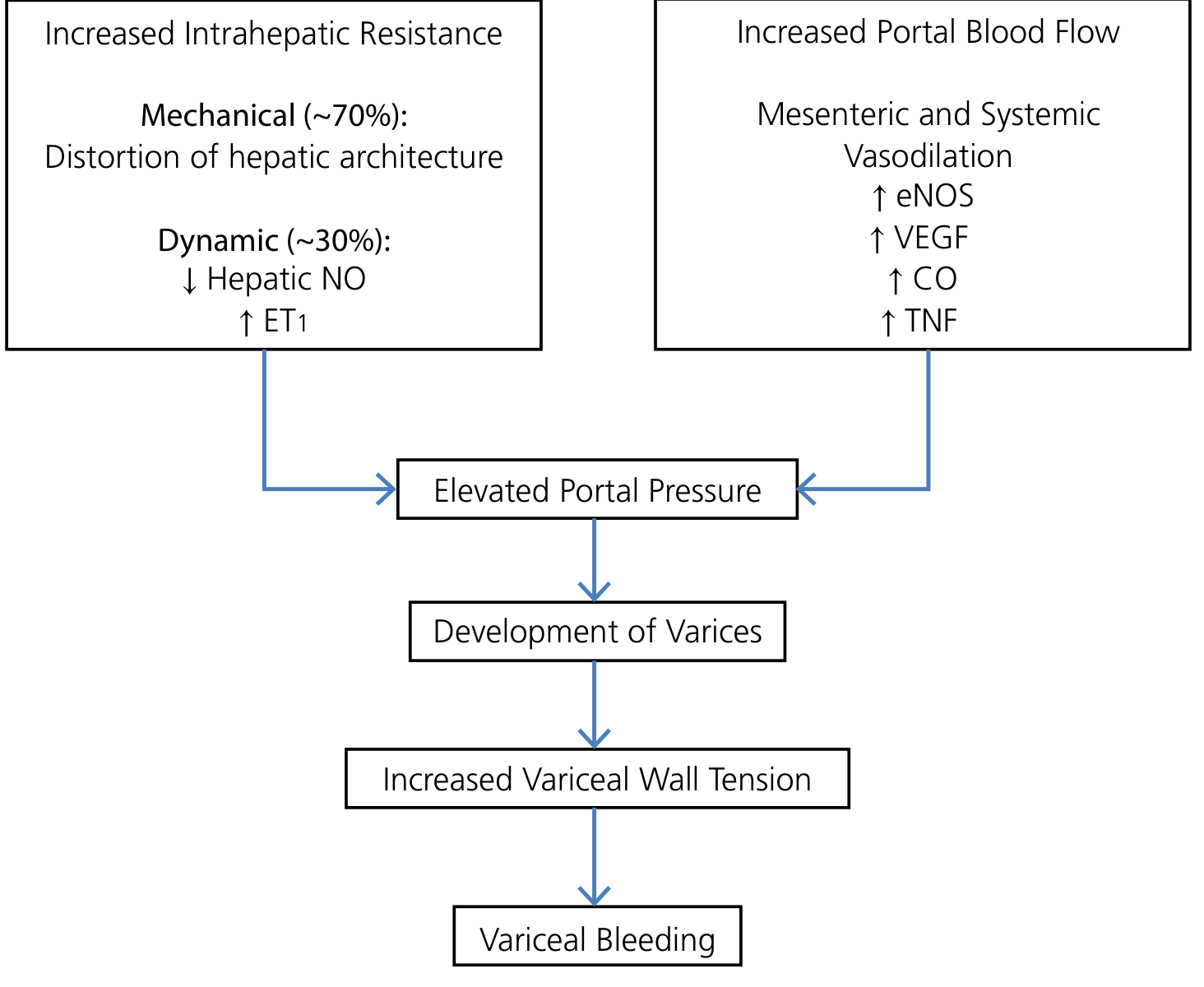
3a. Increased Intrahepatic Resistance (in Cirrhosis)
Two components:
Fixed/mechanical (~70%):
- Architectural distortion from progressive collagen deposition and regenerative nodules
- Vascular obliteration and sinusoidal capillarization
- Activated HSCs deposit collagen in the space of Disse → loss of endothelial fenestrae → formation of a subendothelial basement membrane
- Increased resistance at all levels: intrahepatic portal vein branches, sinusoids, hepatic venules
Dynamic/functional (~30%):
- ↓ intrahepatic NO production (dysfunctional eNOS in cirrhotic liver)
- ↑ ET-1 → HSC contraction → active sinusoidal narrowing
- This component is pharmacologically modifiable
3b. Increased Portal Blood Flow (Hyperdynamic Circulation)
Once portal pressure rises, systemic vasodilatory mediators — particularly NO, VEGF, carbon monoxide, TNF — cause splanchnic arterial vasodilation. This:
- Increases blood flow into the portal system
- Creates a hyperdynamic circulation: high cardiac output, low systemic vascular resistance
- Perpetuates and worsens portal hypertension despite collateral formation
Despite the opening of collaterals, portal pressure is not adequately reduced — hypertension persists.
3c. Classification by Site of Resistance
| Level | Examples |
|---|---|
| Presinusoidal (extrahepatic) | Portal vein thrombosis, splenic vein thrombosis |
| Presinusoidal (intrahepatic) | Schistosomiasis, primary biliary cholangitis (early) |
| Sinusoidal | Cirrhosis (most common in Western countries) |
| Postsinusoidal | Hepatic vein thrombosis (Budd-Chiari), alcohol (centrilobular fibrosis), right heart failure |
4. Portosystemic Collaterals
When portal pressure rises, blood is rerouted through pre-existing anastomoses between portal and systemic venous circulations:
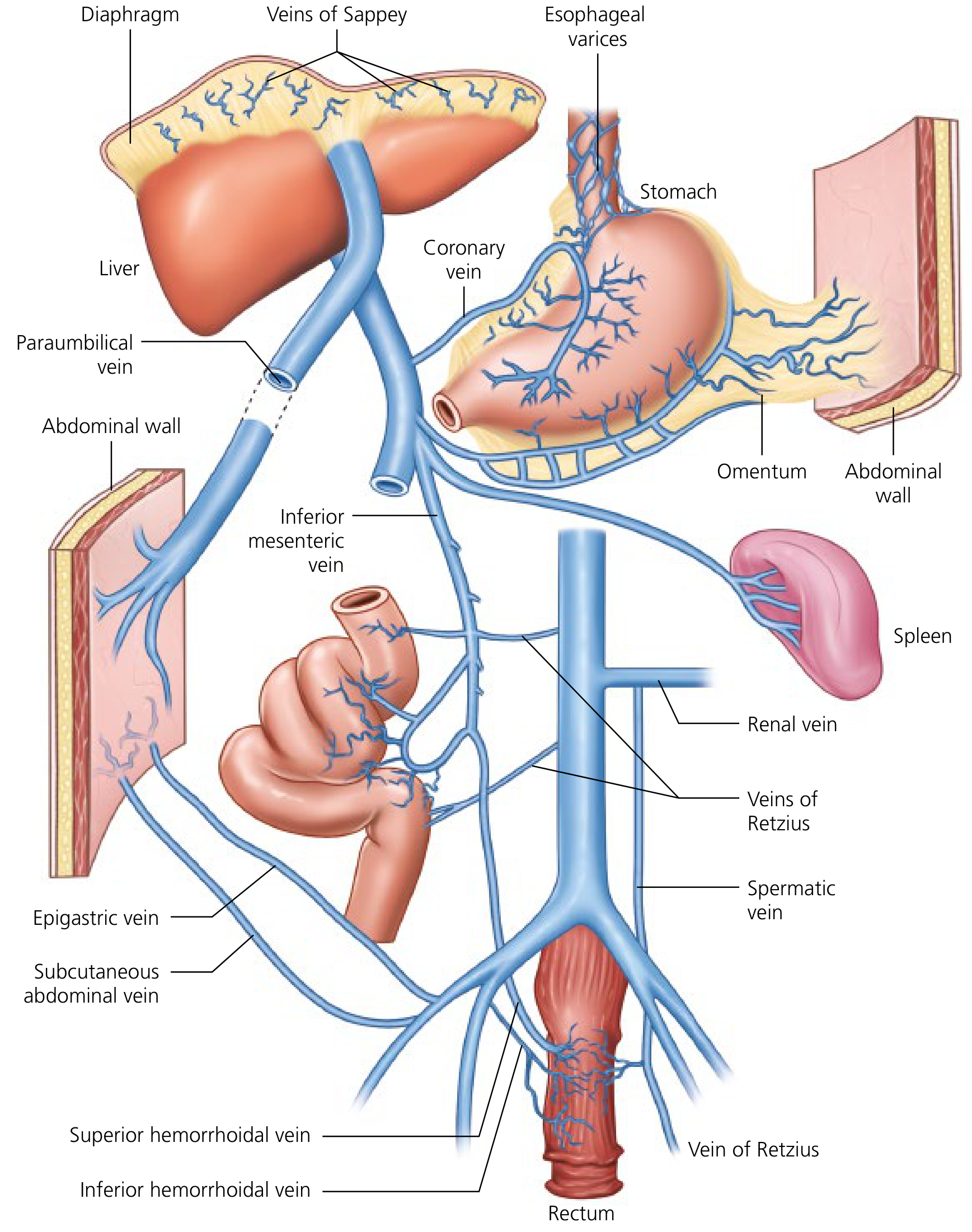
| Site | Portal Tributary | Systemic Vein | Clinical Result |
|---|---|---|---|
| Distal esophagus / proximal stomach | Left gastric (coronary) vein | Azygos system | Esophageal/gastric varices |
| Umbilicus | Paraumbilical vein ← left portal vein | Epigastric/abdominal wall veins | Caput medusae |
| Rectum | Superior hemorrhoidal (inferior mesenteric) | Pudendal vein (inferior hemorrhoidal) | Rectal varices |
| Retroperitoneum | Colonic veins | Renal, spermatic/ovarian, iliac veins | Veins of Retzius |
| Diaphragm | Veins of Sappey | Diaphragmatic veins | Diaphragmatic varices |
5. Downstream Consequences
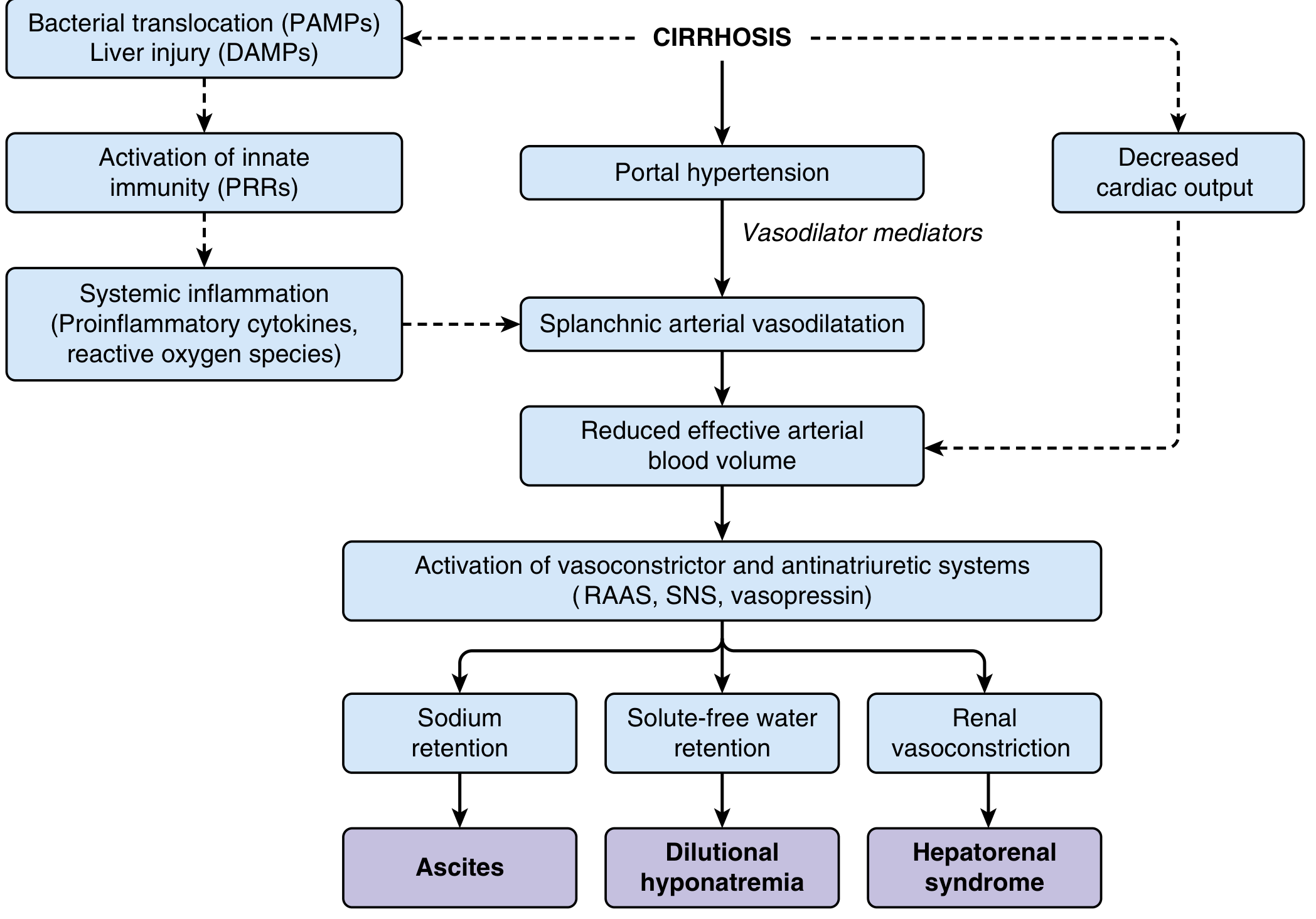
Ascites
Increased portal pressure → increased hydrostatic pressure in splanchnic capillaries → Starling forces favor fluid extravasation into the peritoneal cavity. Splanchnic vasodilation further reduces effective arterial blood volume (EABV), triggering:
- RAAS activation → aldosterone → sodium retention
- SNS activation → renal vasoconstriction
- ADH/vasopressin → water retention → dilutional hyponatremia
Variceal Hemorrhage
Varices rupture when variceal wall tension exceeds wall strength (law of Laplace: tension ∝ pressure × radius). The hepatic venous pressure gradient (HVPG) is the clinical gold standard:
- HVPG ≥ 10 mmHg → clinically significant portal hypertension (risk of varices)
- HVPG ≥ 12 mmHg → threshold for variceal bleeding
- HVPG reduction ≥ 20% from baseline or to < 12 mmHg → significantly reduces bleeding risk
Hepatic Encephalopathy
Portal blood bypasses the liver through collaterals → toxins (notably NH₃) that are normally cleared by hepatic metabolism reach the systemic circulation and cross the blood-brain barrier.
Splenomegaly / Hypersplenism
Elevated portal pressure is transmitted to the splenic vein → passive congestion → splenomegaly → sequestration and destruction of blood cells (thrombocytopenia, anemia, leukopenia).
Hepatopulmonary Syndrome / Portopulmonary Hypertension
Vasoactive mediators bypassing the liver reach pulmonary circulation:
- HPS: intrapulmonary vasodilation → V/Q mismatch → hypoxemia
- PoPH: pulmonary arterial hypertension, related to excess vasoconstrictors reaching the pulmonary bed
6. Measurement: HVPG
The hepatic venous pressure gradient = wedged hepatic venous pressure (WHVP) − free hepatic venous pressure (FHVP), measured via transjugular catheterization. It reflects sinusoidal pressure and is the standard for monitoring in cirrhotic portal hypertension. HVPG does not accurately reflect presinusoidal portal hypertension (e.g., portal vein thrombosis, schistosomiasis).
Sources:
- Yamada's Textbook of Gastroenterology, 7th ed. — Ch. 124, "Pathophysiology of portal hypertension"
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease — Ch. 93, "Portal hypertension"
- Medical Physiology (Boron & Boulpaep) — Ch. 24, "Portal Hypertension"
Symptoms
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive clinical content. Here is the full breakdown of symptoms and signs of portal hypertension:
Symptoms & Signs of Portal Hypertension
Portal hypertension itself is often asymptomatic in its early, compensated stage (HVPG 5–10 mmHg, can persist ≥10 years). Symptoms emerge when clinically significant portal hypertension (CSPH) develops — defined as HVPG ≥ 10 mmHg — and the patient decompensates. The three primary clinical complications are variceal hemorrhage, ascites, and hypersplenism. With decompensation, median survival drops to < 2 years.
1. Gastrointestinal Bleeding
Most dramatic and life-threatening presentation.
- Hematemesis — often effortless, recurrent; vomit described as dark red
- Melena — black tarry stool from upper GI blood
- Hematochezia — if bleeding is brisk
- Sources:
- Esophageal varices — most common (lower esophagus, where left gastric vein anastomoses with azygos)
- Gastric varices — especially fundal; bleed more massively
- Portal hypertensive gastropathy (PHG) — chronic insidious blood loss, iron-deficiency anemia
- Ectopic varices — duodenal, rectal, stomal (less common)
Suspect variceal hemorrhage in any patient with upper GI bleed who has peripheral stigmata of liver disease.
2. Ascites
Most common complication of cirrhosis (~60% of patients within 10 years).
Symptoms:
- Abdominal distension, bloating, early satiety
- Dyspnea (diaphragm elevation, hepatic hydrothorax)
- Discomfort or pain from abdominal fullness
Signs:
- Bulging flanks
- Shifting dullness on percussion
- Fluid wave (large volumes)
- Everted umbilicus
- Hepatic hydrothorax — usually right-sided pleural effusion (diaphragmatic defect allows ascites to track into pleural space)
Key diagnostic lab: SAAG (serum-ascites albumin gradient)
- SAAG ≥ 1.1 g/dL → portal hypertension as cause (cirrhosis, cardiac ascites)
- SAAG < 1.1 g/dL → non-portal cause (malignancy, infection, TB)
- Ascitic fluid protein < 1.5 g/dL → high risk for spontaneous bacterial peritonitis (SBP)
3. Splenomegaly & Hypersplenism
Elevated portal pressure transmits back to the splenic vein → passive congestion and splenic enlargement.
Symptoms:
- Left upper quadrant fullness or dull ache
- Early satiety (from enlarged spleen)
Signs:
- Palpable enlarged spleen (left upper quadrant)
- Hypersplenism → sequestration and destruction of blood cells:
- Thrombocytopenia — most sensitive lab indicator of portal hypertension; also increases bleeding risk
- Leukopenia
- Anemia (hemolytic + nutritional)
Thrombocytopenia is often the first laboratory clue to underlying portal hypertension.
4. Hepatic Encephalopathy (HE)
Portosystemic shunting of blood past the liver → accumulation of neurotoxins (notably NH₃) in systemic circulation → crosses blood-brain barrier.
Symptoms (graded by West Haven criteria):
| Grade | Features |
|---|---|
| 0 / Minimal | Subtle cognitive impairment, detectable only on testing |
| I | Mild confusion, sleep disturbance, shortened attention span, mood change |
| II | Lethargy, disorientation (time/place), personality change, inappropriate behavior |
| III | Somnolence, semi-stupor, significant disorientation, responsive to stimuli |
| IV | Coma, no response to stimuli |
Signs:
- Asterixis ("flapping tremor") — involuntary jerking of outstretched hands; hallmark of early-to-moderate HE
- Fetor hepaticus — sweet, musty breath odor from sulfur compounds (dimethyl sulfide)
- Hyperreflexia, Babinski sign (in advanced cases)
- Slurred speech, ataxia
Precipitants: GI bleeding, infection (SBP), diuretic overdose/electrolyte disturbance, constipation, sedatives, dietary protein excess, TIPS.
5. Peripheral Stigmata of Chronic Liver Disease
These signs on exam point to the underlying cirrhosis driving portal hypertension:
| Sign | Mechanism |
|---|---|
| Spider telangiectasias | Estrogen excess from impaired hepatic metabolism → arteriovenous shunting |
| Palmar erythema | Estrogen excess, hyperdynamic circulation |
| Caput medusae | Paraumbilical venous collaterals (portal → systemic via reopened umbilical vein) |
| Jaundice | Impaired bilirubin conjugation and excretion |
| Gynecomastia / testicular atrophy | Estrogen–androgen imbalance |
| Dupuytren's contracture | Associated with alcohol-related cirrhosis |
| Parotid enlargement | Alcohol-related |
| Leukonychia / Terry's nails | Hypoalbuminemia |
| Peripheral edema | Hypoalbuminemia → reduced oncotic pressure |
| Muscle wasting / sarcopenia | Malnutrition, impaired protein synthesis |
| Venous hum (epigastric) | Collateral flow in falciform ligament |
6. Spontaneous Bacterial Peritonitis (SBP)
Complication of ascites; suspect when ascitic PMN ≥ 250/µL.
Symptoms:
- Fever, abdominal pain/tenderness
- Worsening encephalopathy
- May be asymptomatic — diagnosis requires paracentesis
7. Hepatorenal Syndrome (HRS)
Progressive renal vasoconstriction from RAAS/SNS activation and reduced effective arterial volume.
Symptoms:
- Oliguria, rising creatinine
- Dilutional hyponatremia (serum Na⁺ < 130 mEq/L)
- No proteinuria, no structural kidney disease
8. Cardiopulmonary Complications
| Condition | Key Symptoms |
|---|---|
| Hepatopulmonary syndrome | Dyspnea, platypnea (worse upright, better supine), hypoxemia, clubbing |
| Portopulmonary hypertension | Dyspnea on exertion, reduced exercise tolerance, right heart strain |
| Hepatic hydrothorax | Dyspnea, pleuritic chest pain (usually right-sided) |
Clinical Approach Summary
Portal Hypertension
│
├── GI Bleeding ──── hematemesis, melena (varices, PHG)
├── Ascites ────────── distension, dyspnea, hydrothorax
├── Splenomegaly ──── LUQ fullness → thrombocytopenia
├── Encephalopathy ── confusion, asterixis, fetor hepaticus
├── SBP ───────────── fever + ascites + AMS
├── HRS ───────────── oliguria, hyponatremia, ↑ creatinine
└── Pulmonary ─────── HPS (platypnea), PoPH (exertional dyspnea)
Sources:
- Harrison's Principles of Internal Medicine, 22nd ed. — Ch. 355, "Portal Hypertension"
- Sleisenger & Fordtran's Gastrointestinal and Liver Disease — Ch. 92, "Clinical Assessment"
- Yamada's Textbook of Gastroenterology, 7th ed. — Ch. 124
Treatment
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
I now have all the content needed for a comprehensive treatment overview. Here is the full treatment guide:
Treatment of Portal Hypertension
Treatment is organized around three goals: (1) reducing portal pressure pharmacologically, (2) managing individual complications, and (3) definitive therapy with shunting or liver transplantation.
1. Pharmacological Reduction of Portal Pressure
Nonselective Beta-Blockers (NSBBs)
The cornerstone of chronic portal pressure reduction.
Mechanism:
- β₁ blockade → ↓ cardiac output → ↓ portal inflow
- β₂ blockade → unopposed α₁ vasoconstriction in mesenteric vessels → ↓ splanchnic blood flow → ↓ portal pressure
Agents:
| Drug | Notes |
|---|---|
| Propranolol | Prototype; lipid-soluble, can cause CNS depression |
| Nadolol | Preferred — predominantly renal excretion, low lipid solubility, once daily |
| Carvedilol | Non-selective β-blocker + weak α₁-blocker → also reduces intrahepatic resistance; increasingly first choice; more potent portal pressure reduction than traditional NSBBs |
Titration: Dose is uptitrated targeting a resting heart rate of 55–60 bpm (for propranolol/nadolol); systolic BP must stay > 90 mmHg. Carvedilol doesn't require strict heart rate goals.
HVPG response targets:
- ≥ 20% reduction from baseline, OR
- Absolute HVPG < 12 mmHg → substantially reduces variceal bleeding risk and mortality
Benefit: Long-term NSBB therapy increases decompensation-free survival in compensated cirrhosis by reducing ascites incidence. Use with caution (not routinely withheld) in patients with ascites.
Vasoactive Agents (Acute Bleeding Only)
| Drug | Mechanism | Use |
|---|---|---|
| Octreotide (somatostatin analogue) | ↓ splanchnic vasodilation, ↓ portal inflow | IV infusion during acute bleeding; improves hemostasis, ↓ transfusion requirements |
| Terlipressin (vasopressin analogue) | Splanchnic vasoconstriction | Acute variceal bleed; reduces early mortality |
| Vasopressin | Mesenteric vasoconstriction | Rarely used alone; risk of systemic ischemia |
Other Agents
- Statins (simvastatin): Upregulate eNOS → improve sinusoidal endothelial function → modest portal pressure reduction. Survival benefit in Child-Pugh A/B; unsafe at ≥ 40 mg/day in Child-Pugh B/C due to rhabdomyolysis risk.
- ACE inhibitors / ARBs: Reduce intrahepatic resistance via RAAS blockade; only safe in early (Child-Pugh A) disease — high risk of hypotension and renal failure in advanced cirrhosis.
- Nitrates: No longer routinely used.
2. Management of Variceal Hemorrhage
A. Primary Prophylaxis (Before First Bleed)
Screen all cirrhotics with upper endoscopy (EGD):
- At diagnosis of compensated cirrhosis
- Every 2 years (active disease) or every 3 years (inactive disease)
- Skip screening if liver stiffness < 20 kPa AND no thrombocytopenia (low-risk varices unlikely)
Indication to treat: Medium/large varices, OR small varices with high-risk stigmata (red wale signs, cherry red spots), OR decompensated cirrhosis.
Options (equivalent efficacy):
- NSBB (propranolol, nadolol, or carvedilol) — preferred when tolerated
- Endoscopic variceal ligation (EVL) — preferred if NSBBs contraindicated or not tolerated
Carvedilol may be superior to EVL for preventing a first bleed and may slow progression of small to large varices.
B. Acute Variceal Hemorrhage (Medical Emergency)
Variceal hemorrhage carries 20–30% mortality per episode.
Step-by-step approach:
-
Resuscitation
- Restricted transfusion strategy: transfuse when Hgb < 7 g/dL, target Hgb 7–9 g/dL
- Avoid over-transfusion (worsens portal pressure)
- Do not routinely correct elevated PT with FFP unless active coagulopathy at other sites
-
Vasoactive drugs — start immediately (before endoscopy)
- IV octreotide or terlipressin → reduces portal inflow, aids hemostasis
-
Prophylactic antibiotics — start before endoscopy
- IV ceftriaxone → reduces infections, rebleeding, and mortality
- (Quinolones as alternative; ceftriaxone preferred in advanced cirrhosis)
-
Endoscopy (EGD within 12 hours)
- Endoscopic variceal ligation (EVL) — first-line for esophageal varices
- Sclerotherapy — if EVL unavailable (higher complication rate)
- Gastric varices extending into cardia/fundus → EVL often fails → consider TIPS
-
Balloon tamponade (Sengstaken-Blakemore / Minnesota tube)
- Bridge to definitive therapy if endoscopic control fails
- Self-expanding metal stents are an alternative bridge
-
Early TIPS (within 72 hours)
- In high-risk patients: HVPG > 20 mmHg, or Child-Pugh B with active bleeding at endoscopy, or Child-Pugh C
- Significantly reduces rebleeding and mortality in this group
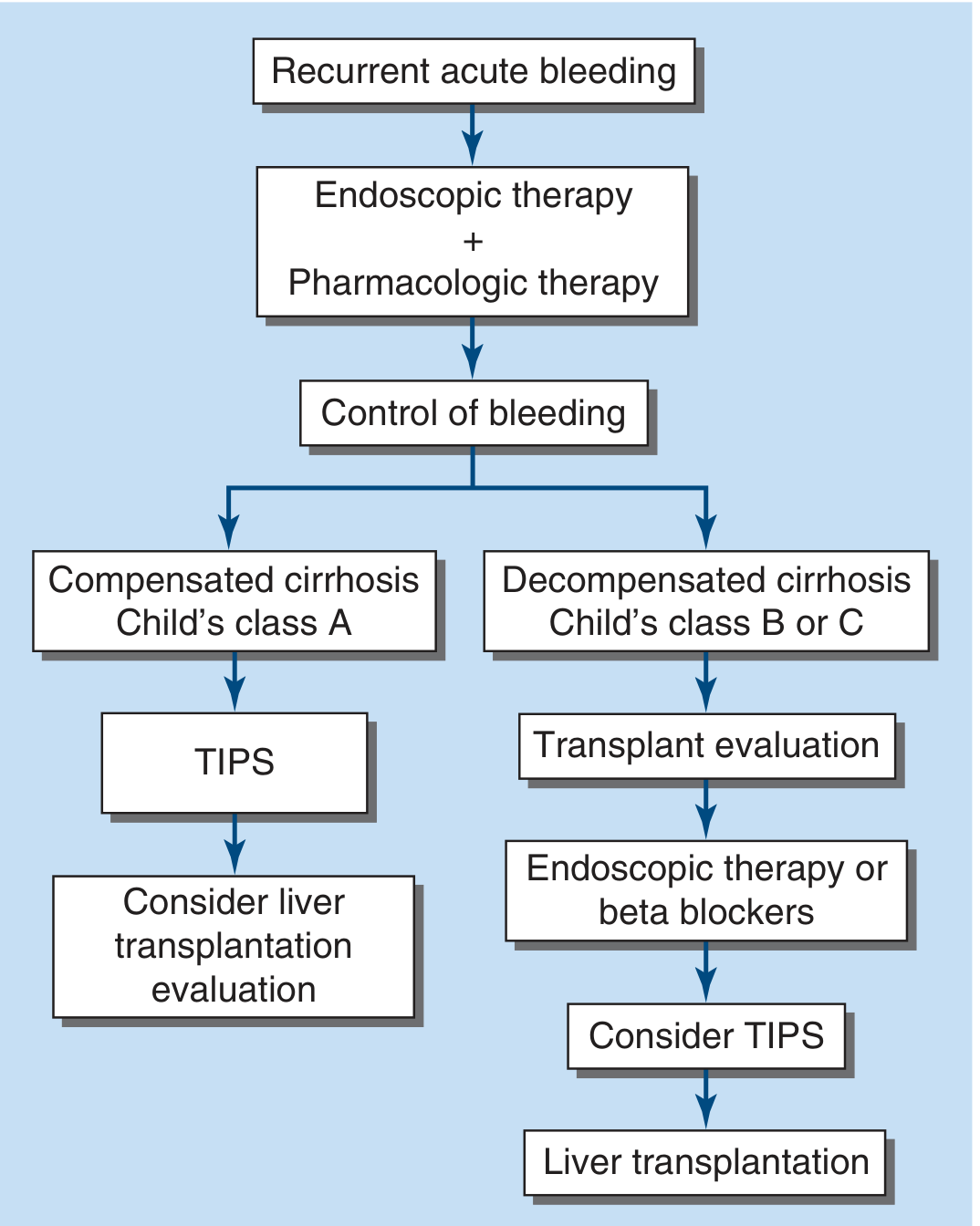
C. Secondary Prophylaxis (After First Bleed)
Prevention of rebleeding combines:
- Repeated EVL until varices obliterated, plus
- NSBB (combination superior to either alone)
If rebleeding despite above → TIPS
3. TIPS (Transjugular Intrahepatic Portosystemic Shunt)
A radiological procedure creating a direct portal-to-hepatic vein shunt through liver parenchyma using a metal stent, placed via the right internal jugular vein.
Goal: Reduce HVPG to < 12 mmHg.
Indications:
- Refractory/recurrent variceal hemorrhage (salvage or secondary prevention)
- Refractory ascites
- High-risk acute variceal bleed (early/pre-emptive TIPS)
- Bridge to liver transplantation
Contraindications:
- Congestive heart failure / tricuspid regurgitation
- Moderate–severe pulmonary hypertension
- Uncontrolled hepatic encephalopathy
- Severe liver failure (relative)
Complications:
- Hepatic encephalopathy — up to 20%, especially in elderly or those with pre-existing HE
- Intra-abdominal hemorrhage (~1–2%)
- Heart failure (sudden ↑ venous return)
- Stent stenosis (monitor with Doppler ultrasound periodically)
- Contrast nephropathy, hemolytic anemia, sepsis
All patients requiring TIPS should be evaluated for liver transplantation.
4. Surgical Shunts
Largely replaced by TIPS but still used in selected patients:
| Shunt | Description | Advantage |
|---|---|---|
| Portacaval shunt (total) | Portal vein → IVC | Highly effective; reduces rebleeding |
| Distal splenorenal shunt (Warren shunt) | Splenic vein → left renal vein (selective) | Diverts only splenic outflow; lower encephalopathy rate than total shunts |
The distal splenorenal shunt is preferred because it preserves hepatoportal perfusion and carries a much lower incidence of encephalopathy.
5. Treatment of Ascites
| Severity | Treatment |
|---|---|
| Mild | Dietary sodium restriction (≤ 2 g/day) |
| Moderate | Spironolactone 100 mg/day ± furosemide 40 mg/day (ratio 100:40); uptitrate to max spironolactone 400 mg + furosemide 160 mg |
| Refractory | Repeated large-volume paracentesis (LVP) + albumin 6–8 g/L of fluid removed; OR TIPS |
| Prophylaxis against SBP | Norfloxacin or trimethoprim-sulfamethoxazole (long-term) in high-risk patients (ascitic protein < 1.5 g/dL) |
After LVP ≥ 5 L → always administer IV albumin (6–8 g per liter removed) to prevent post-paracentesis circulatory dysfunction.
6. Treatment of Hepatic Encephalopathy
Identify and correct precipitants: GI bleeding, infection, dehydration, electrolyte imbalances, constipation, sedatives.
| Treatment | Mechanism / Notes |
|---|---|
| Lactulose | Non-absorbable disaccharide → colonic acidification → traps NH₄⁺ → ↑ nitrogen excretion; goal: 2–3 soft stools/day; mainstay of therapy |
| Rifaximin 550 mg BID | Non-absorbable antibiotic → ↓ gut ammonia-producing bacteria; effective in preventing recurrent HE; has replaced neomycin/metronidazole |
| Zinc supplementation | Cofactor for urea cycle enzymes; relatively safe |
| Dietary protein | Do NOT restrict — worsens sarcopenia; maintain adequate protein intake |
| Portosystemic shunt closure | For refractory HE with large spontaneous shunts |
7. Treatment Summary by Complication
Portal Hypertension Treatment
│
├── Reduce Portal Pressure (all patients with CSPH)
│ └── NSBB (carvedilol preferred) ± EVL
│
├── Variceal Hemorrhage
│ ├── Acute: octreotide + ceftriaxone + EVL ± early TIPS
│ └── Secondary prevention: EVL + NSBB → TIPS if fails
│
├── Ascites
│ ├── Na restriction → spironolactone ± furosemide
│ └── Refractory: LVP + albumin or TIPS
│
├── Hepatic Encephalopathy
│ └── Lactulose ± rifaximin; correct precipitants
│
├── SBP
│ └── Cefotaxime (treatment); norfloxacin (prophylaxis)
│
├── HRS
│ └── Terlipressin + albumin; TIPS as bridge; transplant
│
└── Definitive Therapy
└── Liver transplantation (evaluate all decompensated patients)
Sources:
- Harrison's Principles of Internal Medicine, 22nd ed. — Ch. 355
- Yamada's Textbook of Gastroenterology, 7th ed. — Ch. 124
- Sleisenger & Fordtran's Gastrointestinal and Liver Disease — Ch. 92
- Miller's Anesthesia, 10th ed. — Ch. 14 (TIPS)
This is a shared conversation. Sign in to Orris to start your own chat.