Coronary artery disease
Reading File
Finding Sources
Finding Sources
Searching PubMed
"coronary artery disease" AND management
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
I now have comprehensive material from multiple authoritative sources. Here is the full, detailed response:
Coronary Artery Disease (CAD)
Definition
Coronary artery disease refers to the narrowing or obstruction of one or more of the epicardial coronary arteries, most commonly caused by atherosclerosis. It is the leading cardiovascular disease globally, causing approximately 600,000 first acute myocardial infarctions (MIs), 200,000 recurrent MIs, and ~170,000 "silent" MIs annually in the United States alone. About 365,000 Americans die from CAD each year. - Goldman-Cecil Medicine
Pathophysiology
Atherosclerosis
The foundational process begins when LDL accumulates in the arterial intima and becomes oxidized, triggering the release of chemokines and adhesion molecules. This recruits monocytes that differentiate into macrophages, which engulf oxidized cholesterol to form foam cells. Macrophages also produce proinflammatory mediators (TNF, IL-1, free radicals, prothrombotic factors), creating a chronic inflammatory milieu within the vessel wall. - Goldman-Cecil Medicine, Pathophysiology of Atherosclerosis
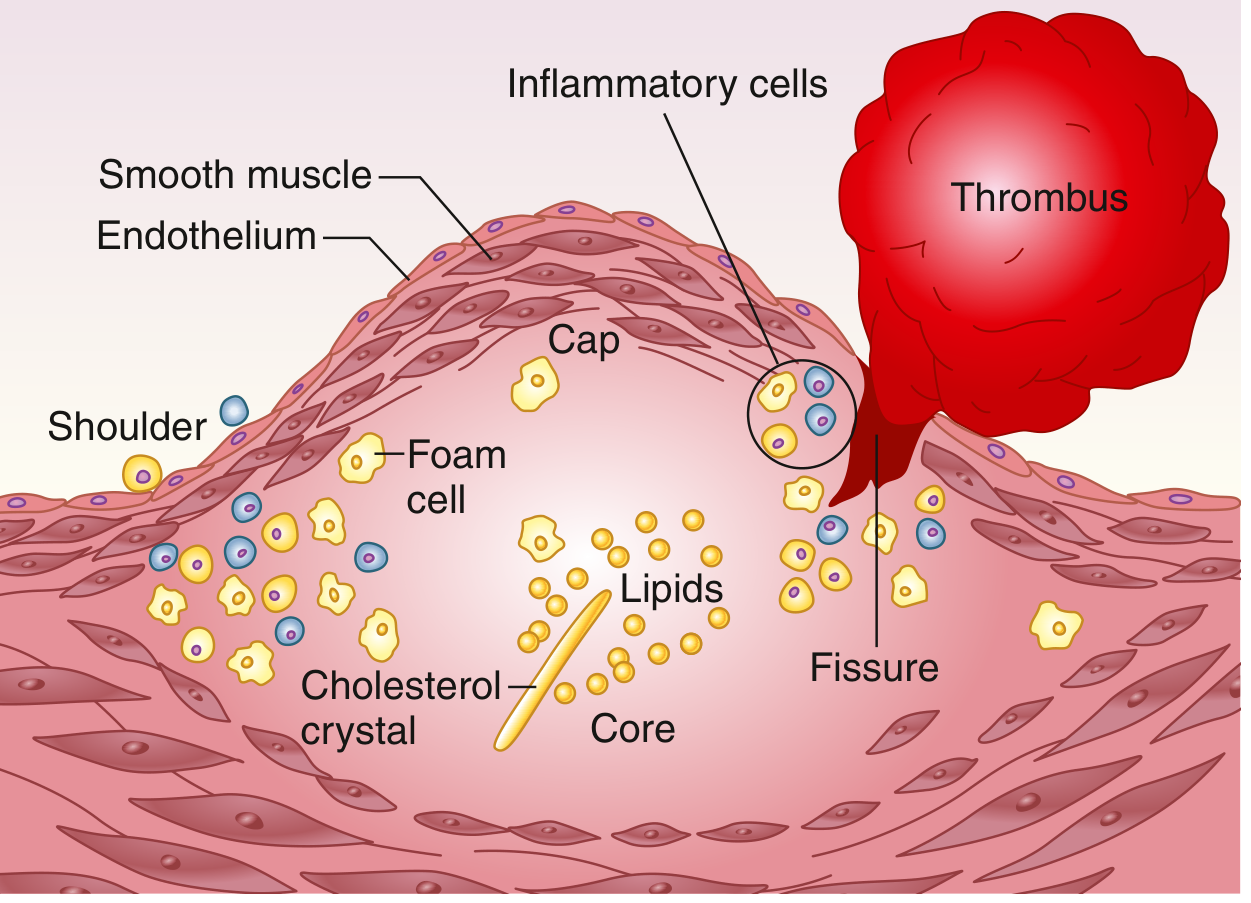
Plaque rupture and atherothrombosis. The advanced plaque has a lipid-laden necrotic core covered by a fibrous cap. Rupture at the shoulder region exposes thrombogenic material, triggering platelet aggregation and thrombus formation. - Goldman-Cecil Medicine
Plaque Rupture and Thrombosis
The atherosclerotic process is typically silent for decades. Clinical events occur when a vulnerable plaque ruptures, exposing circulating blood to the highly thrombogenic core (lipids, collagen, tissue factor). Platelet aggregates form and are stabilized by a fibrin network. Tissue factor - expressed in vascular smooth muscle cells and macrophage-rich plaques - initiates the coagulation cascade. Atherothrombi can fill the lumen within minutes, causing ischemia and infarction.
Up to one-third of acute MIs may result from superficial erosion of fibrous caps (rather than full rupture), and a minority involve a fractured calcified nodule. Matrix metalloproteinases and cysteine proteinases (from macrophages) are found at rupture sites and contribute to plaque instability. - Goldman-Cecil Medicine
Risk Factors
Non-modifiable:
- Age (men >45, women >55 or postmenopausal)
- Male sex
- Family history of premature CAD
Modifiable:
- Hypertension
- Hypercholesterolemia (elevated LDL)
- Diabetes mellitus
- Tobacco use
- Truncal obesity / sedentary lifestyle
- Cocaine use (associated with AMI even in young patients)
When all modifiable risk factors are optimal, the lifetime risk of CAD for a 45-year-old is estimated at <5%. With two or more major risk factors, it rises to 50% for men and 31% for women. All modifiable risk factors combined account for over 90% of the population-attributable risk of acute MI globally. The genetic contribution is estimated at ~40%, and polygenic risk scores can provide supplementary prognostic information. - Goldman-Cecil Medicine
Clinical Spectrum
CAD presents across a spectrum:
| Syndrome | Description |
|---|---|
| Stable angina | Predictable chest pain with exertion, relieved by rest or nitrates |
| Unstable angina (UA) | Angina at rest, new-onset, or crescendo pattern; no troponin rise |
| NSTEMI | UA pattern + elevated troponins (myocardial necrosis present) |
| STEMI | Complete occlusion with ST elevation on ECG; requires urgent reperfusion |
| Silent ischemia | Ischemia without chest pain (common in diabetics and elderly) |
- Stable angina is promptly relieved by rest or nitroglycerin
- Unstable angina occurs with increased frequency, duration, and intensity and is not relieved by rest or nitroglycerin; it is an acute coronary syndrome (ACS) requiring urgent medical attention
- The distinction between UA and NSTEMI is the presence of elevated cardiac troponins (indicating necrosis) in NSTEMI - Lippincott Pharmacology; Swanson's Family Medicine
Diagnosis
History
Typical features: substernal chest pressure/heaviness, radiation to left arm, jaw, or neck, associated with exertion, diaphoresis, dyspnea, nausea. Traditional cardiac risk factors are modestly predictive but are poor predictors of ACS risk in the emergency setting. - Tintinalli's Emergency Medicine
ECG
- Resting ECG: ST depression or T-wave inversions in stable disease; ST elevation in STEMI
- Exercise stress ECG: first-line for diagnosis in patients with an interpretable ECG and adequate exercise capacity
Cardiac Biomarkers
- High-sensitivity troponin (hsTn): cornerstone of ACS diagnosis
- Serial measurements are more reliable than a single value
Imaging Modalities
- Stress echocardiography: reliable for initial diagnosis of CAD, especially when the stress ECG is non-diagnostic
- Coronary CTA (CCTA): useful for ruling out CAD in intermediate pre-test probability; pre-test probability <15% = CCTA best suited to rule out; >85% = invasive angiography most appropriate
- Nuclear perfusion imaging / Cardiac MRI: stress perfusion
- Invasive coronary angiography (cardiac catheterization): gold standard for anatomy; mandatory before revascularization
Indications for coronary angiography include: CCS Class II-IV stable angina on medical therapy, ACS (UA/NSTEMI/STEMI), chest pain of unclear etiology with equivocal noninvasive testing, pulmonary edema with reduced EF, cardiogenic shock, prior to cardiac surgery when CAD is suspected, and unexplained new-onset cardiomyopathy. - Harrison's Principles of Internal Medicine 22e
Management
1. Lifestyle and Risk Factor Modification
- Smoking cessation
- Heart-healthy diet (Mediterranean-type)
- Regular aerobic exercise
- Weight management
- Control of hypertension, diabetes, dyslipidemia
- Cardiac rehabilitation (indicated after MI, CABG, PCI, valvular surgery) - Fuster & Hurst's The Heart
2. Pharmacotherapy
Antiplatelet therapy:
- Aspirin 75-325 mg/day: reduces coronary events in stable CAD, UA, and post-MI patients
- P2Y12 inhibitors (clopidogrel, ticagrelor, prasugrel): used as dual antiplatelet therapy (DAPT) after ACS or PCI
- A 2025 Lancet meta-analysis (PMID 40902613) directly compared clopidogrel vs. aspirin for secondary prevention, with implications for long-term antiplatelet choice post-PCI
Lipid-lowering:
- High-intensity statins: first-line; reduce atherosclerotic lesions, inhibit progression, and lower coronary events and all-cause mortality
- Ezetimibe: add-on to statins for additional LDL reduction
- PCSK9 inhibitors (evolocumab, alirocumab): monoclonal antibodies for very high-risk patients or statin intolerance; substantial LDL reduction and CV event reduction
Beta-blockers:
- Reduce myocardial oxygen demand (decrease HR, contractility, BP)
- Standard post-MI and in stable angina
- Combined with ACE inhibitor in post-MI reduced EF
ACE inhibitors / ARBs:
- Indicated post-MI, especially with reduced LV function
- Reduce mortality, LV remodeling, and recurrent events
Nitrates:
- Relieve angina (venodilation reduces preload; coronary vasodilation)
- Useful in both stable angina and ACS/UA
- Long-acting forms for prophylaxis; sublingual for acute relief
Calcium channel blockers:
- Non-dihydropyridines (verapamil, diltiazem): rate control + vasodilation
- Dihydropyridines (amlodipine): vasodilation; useful in vasospastic angina
Ranolazine:
- Late sodium channel inhibitor; reduces angina frequency without major hemodynamic effects; useful in refractory stable angina - Swanson's; Harrison's; Katzung's Pharmacology; Goldman-Cecil
3. Revascularization
Percutaneous Coronary Intervention (PCI):
- Preferred for single/two-vessel disease without proximal LAD involvement
- Primary PCI is standard of care for STEMI (door-to-balloon <90 minutes)
- Drug-eluting stents (DES) significantly reduce in-stent restenosis vs. bare-metal stents
Coronary Artery Bypass Grafting (CABG):
CABG is preferred over PCI in the following clinical scenarios (per 2021 ACC/AHA/SCAI guidelines):
| Scenario | Recommendation Class |
|---|---|
| Three-vessel disease or left main CAD | COR 1 (CABG > PCI) |
| Diabetes + multivessel CAD | COR 1 (CABG preferred) |
| Complex CAD (high SYNTAX score) | COR 1 |
| Previous CABG with refractory angina from LAD disease when LIMA can be used | COR 2a |
| Multivessel CAD + inability to tolerate/adhere to DAPT | COR 2a |
| Symptomatic recurrent diffuse in-stent restenosis | COR 2a |
Left internal mammary artery (LIMA) to LAD bypass offers superior long-term patency compared to vein grafts. - Sabiston Textbook of Surgery 8e
4. Special Populations
- Atrial fibrillation + stable CAD: A 2025 JACC meta-analysis (PMID 39918465) addresses optimal anticoagulation + antiplatelet combination
- Diabetes: CABG generally preferred over PCI for multivessel disease (FREEDOM trial data)
- CKD/dialysis patients: Exercise stress testing and ECG-based tests are less reliable; nuclear or pharmacologic imaging preferred
- Pregnancy: Aggressive treatment in ICU for intractable ischemia; PCI or CABG when conservative measures fail
Secondary Prevention
Post-ACS or post-revascularization patients should receive:
- Aspirin (indefinite)
- P2Y12 inhibitor (minimum 12 months after ACS/stent)
- High-intensity statin
- Beta-blocker (especially if reduced EF)
- ACE inhibitor/ARB
- Cardiac rehabilitation
- Lifestyle modification
- Swanson's Family Medicine Review
Recent Evidence (2025)
- Clopidogrel vs. aspirin meta-analysis (Lancet 2025) challenges traditional aspirin-first secondary prevention - individual patient data meta-analysis in progress (PMID 40902613)
- Anticoagulation + antiplatelet in AF + stable CAD (JACC 2025) clarifies optimal dual vs. triple therapy strategy (PMID 39918465)
- Depression as an undertreated CV risk factor in CAD guidelines highlighted by a 2025 European Heart Journal systematic review (PMID 40878995)
Sources: Goldman-Cecil Medicine (International Ed.); Harrison's Principles of Internal Medicine 22e (2025); Braunwald's Heart Disease 12e; Sabiston Textbook of Surgery 8e; Fuster & Hurst's The Heart 15e; Katzung's Basic & Clinical Pharmacology 16e; Tintinalli's Emergency Medicine; Swanson's Family Medicine Review
This is a shared conversation. Sign in to Orris to start your own chat.