Methods of airway assesment
Reading File
Finding Sources
Finding Sources
Searching the Web
methods of airway assessment anaesthesia Mallampati LEMON 2024
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive material to give a thorough, well-structured answer.
Methods of Airway Assessment
A pre-procedure airway assessment is mandatory before every anaesthetic and any anticipated intubation. No single test predicts a difficult airway with 100% accuracy; a combination of history, physical examination, and scoring systems is the standard approach.
1. History
The single most predictive factor for difficult intubation is a previous history of difficult intubation. The history should cover:
- Prior anaesthetic records and any documented difficulty
- Symptoms of airway-related pathology: stridor, dysphagia, hoarseness, positional dyspnoea
- History of snoring / obstructive sleep apnoea (predictive of difficult mask ventilation)
- Changes in weight or neck size since last anaesthetic
- Head and neck surgery, radiation, or trauma
- Conditions that restrict mouth opening: rheumatoid arthritis, temporo-mandibular joint disease, scleroderma
2. External Visual Inspection
Inspect the face and neck for:
- Obvious facial deformities, asymmetry, or dysmorphic features
- Short, thick, or bull neck
- Receding or small mandible (micrognathia)
- Large goitre or neck masses
- Facial burns, angioedema, Ludwig's angina, airway tumours
- Beard (increases risk of poor mask seal)
- Cervical collar or traction devices (restrict laryngoscopy)
- Neck circumference >43 cm (17 inches) is more predictive of difficult intubation than BMI alone
3. Mouth Opening
- Measure inter-incisor distance with maximal mouth opening
- < 3 cm (or < 2 fingerbreadths) between upper and lower incisors predicts difficult intubation
- Inspect the oropharynx for neoplasm, high arched palate, macroglossia
4. Mallampati Classification
The most widely used scoring test. Performed with the patient seated, mouth fully open, tongue protruded maximally, and phonation avoided. It relates tongue size to the oral cavity.
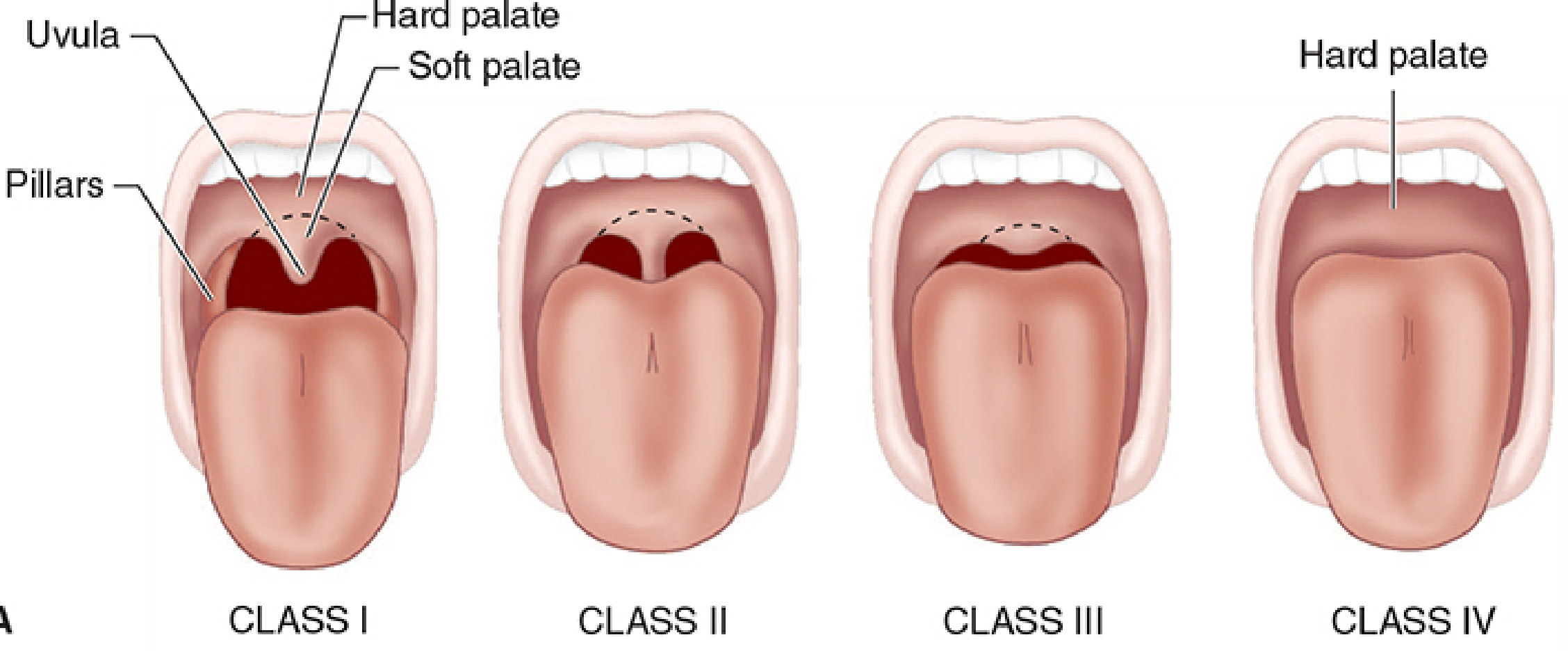
| Class | Structures Visible |
|---|---|
| I | Soft palate, uvula, fauces, tonsillar pillars all visible |
| II | Soft palate, uvula, upper fauces visible; pillars obscured |
| III | Only soft and hard palate visible |
| IV | Only hard palate visible |
- Class III or IV predicts a potentially difficult laryngoscopy
- Best used in combination with other tests - sensitivity alone is ~39% but specificity ~86%
- The modified Mallampati test (Samsoon & Young, 1987) adds Class IV to the original three-class system
5. Thyromental Distance (TMD)
- Measured from the thyroid notch to the mentum (chin) with the neck fully extended
- < 6.5 cm (< 3 fingerbreadths) indicates reduced submandibular space ("anterior larynx") and predicts difficult intubation
- During laryngoscopy, the tongue must be displaced into this space; a small or non-compliant space limits glottic exposure
6. Sternomental Distance (SMD)
- Measured from the sternal notch to the point of the chin with the head in full extension, mouth closed
- < 12.5 cm is associated with difficult intubation
- Reflects the combined contribution of neck mobility and mandibular space
7. Neck Range of Motion
- Optimal laryngoscopy requires cervical flexion + atlanto-occipital extension (the "sniffing position")
- < 80° of total neck flexion-extension is predictive of difficult intubation
- Conditions that restrict movement: cervical spondylosis, rheumatoid arthritis, ankylosing spondylitis, Halo brace, collar
8. Upper Lip Bite Test (ULBT)
Patient is asked to bite the upper lip with the lower incisors:
- Class I: Lower incisors bite above the upper lip vermilion line - easy intubation likely
- Class II: Lower incisors bite below the vermilion line
- Class III: Lower incisors cannot reach the upper lip - difficult intubation predicted
Higher specificity and less interobserver variability than Mallampati alone. Also assesses temporo-mandibular joint mobility and mandibular prognathism.
9. Mandibular Prognathism (Jaw Protrusion Test)
- Ask the patient to slide the lower jaw forward so the lower incisors protrude beyond the upper
- Inability to prognath (lower incisors cannot reach or exceed the upper) predicts difficult laryngoscopy
- Reflects temporo-mandibular joint laxity and range of motion
10. Dentition Assessment
- Long upper incisors impair direct laryngoscopy
- Loose or poor dentition increases risk of dental trauma and aspiration of teeth
- Edentulous patients are usually easier to intubate but harder to mask-ventilate (poor seal)
- Veneers, crowns, and bridges are at high risk of damage
11. Mnemonics for Difficult Airway Prediction
LEMON (Emergency Medicine / Difficult Intubation)
| Letter | Assessment |
|---|---|
| L - Look externally | Facial trauma, obesity, large incisors, large tongue, dysmorphic features |
| E - Evaluate 3-3-2 rule | Mouth opening ≥3 fingers; hyomental distance ≥3 fingers; thyroid-to-hyoid ≥2 fingers |
| M - Mallampati | Class I-IV |
| O - Obstruction | Stridor, foreign body, tumour, epiglottitis, angioedema |
| N - Neck mobility | Extension and flexion assessed |
MOANS (Difficult Bag-Mask Ventilation)
| Letter | Factor |
|---|---|
| M | Mask seal difficulty (beard, facial trauma) |
| O | Obesity / Obstruction |
| A | Age > 55 |
| N | No teeth (edentulous) |
| S | Stiff lungs (asthma, COPD) |
ROMAN (Difficult Bag-Mask Ventilation - Rosen's EM)
- R - Radiation/Resistance to ventilation
- O - Obstruction, Obesity, OSA
- M - Mallampati, Male, Mask seal
- A - Aged
- N - No teeth
12. Multivariate Scoring Systems
Individual tests have poor sensitivity; combined scores perform better:
| Score | Components |
|---|---|
| Wilson Risk Sum Score | Weight, head/neck movement, jaw movement, receding mandible, buck teeth |
| El-Ganzouri Risk Index | Mouth opening, TMD, Mallampati, neck movement, prognathism, weight, previous difficult intubation |
13. Imaging Adjuncts
- Point-of-care ultrasound (POCUS): Skin-to-epiglottis distance (US-DSE) shows higher sensitivity (0.80) and specificity (0.77) than most bedside tests in a 2024 systematic review - now increasingly used pre-operatively
- CT/MRI neck: For known masses, subglottic stenosis, or complex pathology
- Lateral neck X-ray: Useful for assessing tracheal deviation, subglottic narrowing, retropharyngeal masses
14. Factors Associated With Difficulty (Summary)
From Tintinalli's Emergency Medicine, the key risk factors are:
- Obesity
- History of snoring / sleep apnoea
- Short neck / limited neck mobility
- Small or large chin
- Prominent incisors
- High arched palate
- Edentulous anatomy
- Facial or airway trauma
- Head and neck tumours
- Angioedema, Ludwig's angina
- Airway burns / inflammation
Key Principle
No single test is sufficient. The ASA difficult airway guidelines and anaesthesia texts (Morgan & Mikhail, Miller's) recommend a combined assessment: history + visual inspection + mouth opening + Mallampati + thyromental distance + neck mobility + prognathism. Absence of all abnormal findings is reassuring but never guarantees an easy airway - the clinician must always have a plan B and C ready.
Sources:
- Morgan and Mikhail's Clinical Anesthesiology, 7e, p. 570-571
- Miller's Anesthesia, 10e, Box 40.1, pp. 5845-5851
- Tintinalli's Emergency Medicine, Table 29A-2, pp. 221-222
- 2024 systematic review (BMC Anesthesiology) - ultrasound-based US-DSE outperforms traditional bedside tests
This is a shared conversation. Sign in to Orris to start your own chat.