Explain the DEFINITION Etiopathogenesis(CHART), Diagnosis(CLINICAL FEATURES, INVESTIGATION), Principles of management (NON PHARMACOLOGICAL & PHARMACOLOGICAL )and Ayurvedic perspective( SHODHAN & SAMANANA of Ashu Vrikka-nishkriyata (Acute Renal Failure) & Chirakaari vrikka-nishkriyata ( Chronic Renal Failure)
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Searching the Web
Ayurvedic perspective Ashu Vrikka Nishkriyata acute renal failure Shodhana Shamana treatment
Reading File
Reading Web Page
https://ahr.a2zjournals.com/index.php/ahr/article/download/1…
Finding Sources
Finding Sources
Finding Sources
Searching the Web
Vrikka Nishkriyata Ayurvedic concept ARF CRF Dosha Samprapti Shodhana Shamana herbs Punarnava Gokshura Varuna
Reading File
Reading File
Searching the Web
Ashu Vrikka Nishkriyata Chirakaari Vrikka Nishkriyata Ayurvedic definition pathogenesis Dosha treatment Shodhana Basti
Reading File
Reading Web Page
https://www.ijcrt.org/papers/IJCRT2411055.pdf
Loading Image
Ashu Vrikka-Nishkriyata (Acute Renal Failure / AKI) & Chirakaari Vrikka-Nishkriyata (Chronic Renal Failure / CKD)
PART I — ASHU VRIKKA-NISHKRIYATA (Acute Renal Failure / Acute Kidney Injury)
1. DEFINITION
Acute Kidney Injury (AKI) — formerly "Acute Renal Failure" — is a rapid decline in the kidney's ability to clear waste products and maintain fluid-electrolyte homeostasis, occurring over hours to days.
KDIGO 2012 Diagnostic Criteria (current gold standard)
| Criterion | Threshold |
|---|---|
| Rise in serum creatinine | ≥ 0.3 mg/dL within 48 hours OR |
| Rise in serum creatinine | ≥ 1.5× baseline within prior 7 days OR |
| Urine output | < 0.5 mL/kg/h for ≥ 6 hours |
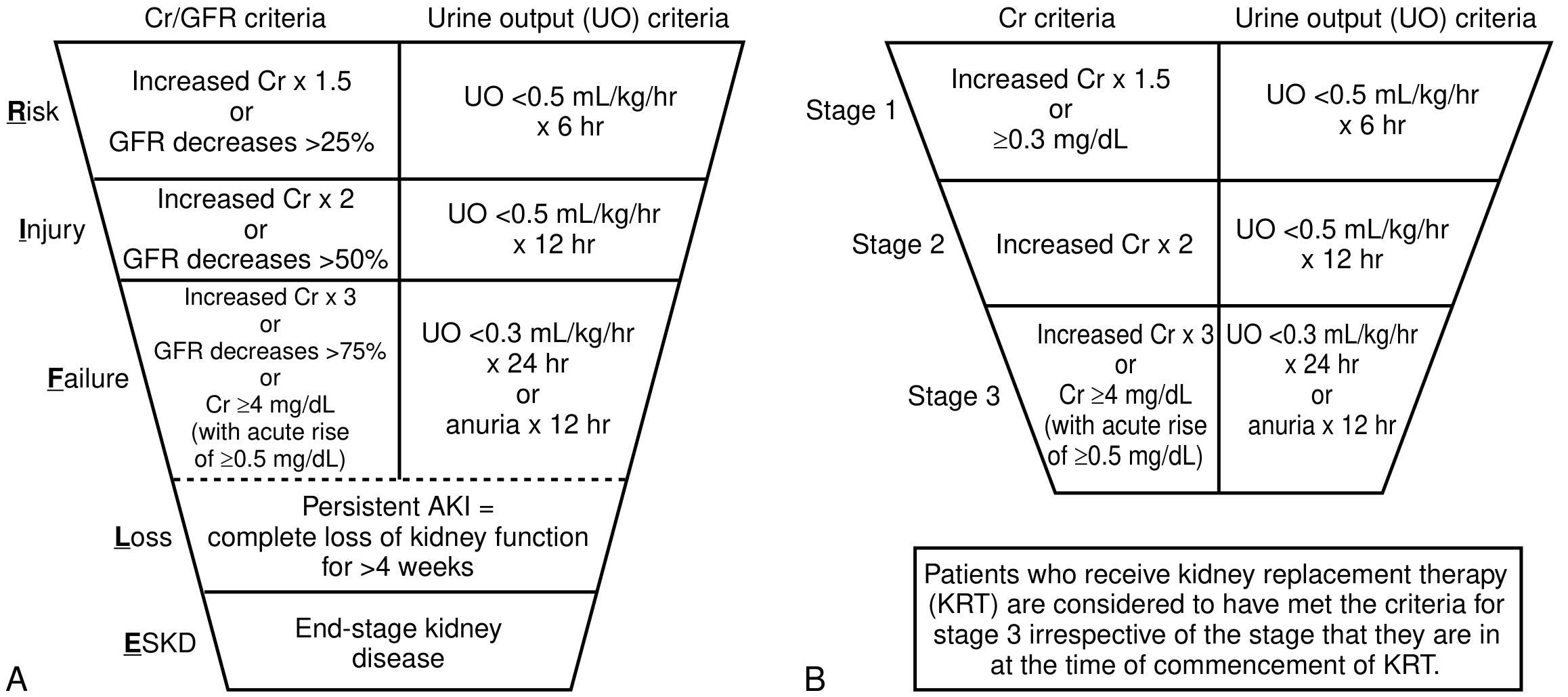
STAGING (KDIGO)
| Stage | Serum Creatinine | Urine Output |
|---|---|---|
| 1 | 1.5–1.9× baseline or ≥0.3 mg/dL rise | <0.5 mL/kg/h × 6–12 h |
| 2 | 2.0–2.9× baseline | <0.5 mL/kg/h × ≥12 h |
| 3 | ≥3× baseline OR ≥4.0 mg/dL OR RRT initiated | <0.3 mL/kg/h × ≥24 h OR anuria ≥12 h |
RIFLE Classification (older, still used):
- Risk → Injury → Failure → Loss (complete loss >4 weeks) → ESKD
2. ETIOPATHOGENESIS — CHART
Etiological Classification
ACUTE KIDNEY INJURY (AKI)
│
├── PRE-RENAL (most common ~55–60%)
│ ├── Hypovolemia: hemorrhage, burns, vomiting, diarrhea, dehydration
│ ├── Low cardiac output: heart failure, cardiogenic shock, cardiac tamponade
│ ├── Systemic vasodilation: sepsis, anaphylaxis, hepatorenal syndrome
│ ├── Renal afferent arteriolar constriction: NSAIDs, contrast agents
│ └── Efferent arteriolar dilation: ACE inhibitors, ARBs
│
├── INTRA-RENAL / RENAL (~35–40%)
│ ├── Tubular (ATN — most common intrinsic cause)
│ │ ├── Ischemic ATN (prolonged prerenal → tubular necrosis)
│ │ └── Nephrotoxic ATN
│ │ ├── Exogenous: aminoglycosides, amphotericin B, contrast dye,
│ │ │ cisplatin, cyclosporine
│ │ └── Endogenous: myoglobin (rhabdomyolysis), hemoglobin (hemolysis),
│ │ uric acid (tumor lysis), myeloma proteins
│ ├── Glomerular: rapidly progressive GN, SLE, vasculitis
│ ├── Interstitial: acute interstitial nephritis (drugs, infections)
│ └── Vascular: renal artery/vein thrombosis, malignant hypertension,
│ thrombotic microangiopathy (HUS/TTP)
│
└── POST-RENAL / OBSTRUCTIVE (~5%)
├── Ureteral: calculi, strictures, retroperitoneal fibrosis
├── Bladder: BPH, neurogenic bladder, clot retention, bladder carcinoma
└── Urethral: strictures, phimosis
Pathogenetic Mechanism of Ischemic ATN
↓ Renal Perfusion
↓
Tubular cell ischemia → ATP depletion
↓
↑ Intracellular Ca²⁺ + reactive oxygen species
↓
Cell swelling, brush border loss, cytoskeleton disruption
↓
Cell death (necrosis/apoptosis) → tubular obstruction by casts
↓
Backleak of glomerular filtrate → ↓ effective GFR
↓
Oliguria / Anuria → AKI
Key mediators: Loss of polarity, Na⁺-K⁺-ATPase mislocalization, tubuloglomerular feedback activation, afferent arteriolar vasoconstriction (endothelin, thromboxane A₂), neutrophil/macrophage infiltration.
3. DIAGNOSIS
A. CLINICAL FEATURES
Symptoms (develop as azotemia worsens):
- Oliguria (<400 mL/day) or anuria (<100 mL/day)
- Nausea, vomiting, anorexia
- Fatigue, lethargy, confusion (uremic encephalopathy)
- Asterixis, myoclonus (severe uremia)
- Pericardial friction rub (uremic pericarditis)
- Abnormal bleeding (platelet dysfunction)
Signs of volume overload:
- Peripheral oedema
- Raised JVP
- Pulmonary oedema (dyspnoea, basal crepitations)
- Hypertension
Signs pointing to etiology:
- Hypotension + skin turgor ↓ → prerenal
- Palpable bladder / suprapubic fullness → obstructive (post-renal)
- Purpuric rash → vasculitis/HUS
- Livedo reticularis → cholesterol emboli
Phases of AKI (particularly ATN):
| Phase | Duration | Key Feature |
|---|---|---|
| Initiation | Hours–days | Injury occurring; creatinine rising |
| Oliguric | 1–3 weeks (avg 10–14 days) | UO <400 mL/day; ↑ BUN, creatinine; hyperkalaemia, acidosis |
| Diuretic | Days–weeks | UO 3–5 L/day; risk of dehydration, hyponatraemia |
| Recovery | Weeks–months | GFR gradually returns; may be incomplete |
B. INVESTIGATIONS
Urinalysis & Microscopy:
| Finding | Suggests |
|---|---|
| Specific gravity >1.020; urine Na <20 mEq/L; FENa <1% | Prerenal |
| Granular "muddy brown" casts; renal tubular epithelial cells; urine Na >50 mEq/L; FENa >3% | ATN (intrinsic) |
| RBC casts, dysmorphic RBCs; proteinuria | Glomerulonephritis |
| WBC casts, eosinophiluria | Acute interstitial nephritis |
| No casts; dilute urine | Obstructive (post-renal) |
FENa (Fractional Excretion of Sodium) = (Urine Na × Plasma Cr) / (Plasma Na × Urine Cr) × 100
Serum Biochemistry:
- Serum creatinine & BUN (rising)
- Electrolytes: Hyperkalaemia, Hyponatraemia, Hyperphosphataemia, Hypocalcaemia
- Arterial blood gas: metabolic acidosis (↓ pH, ↓ HCO₃⁻, ↑ anion gap)
- CBC: anaemia (dilutional), eosinophilia (AIN), thrombocytopenia (HUS/TTP)
- Complement (C3/C4), ANA, ANCA, anti-GBM antibodies (if glomerular cause suspected)
Imaging:
- Ultrasound kidneys: first-line — bilateral enlarged/normal kidneys (AKI); small kidneys (CKD); hydronephrosis (obstructive)
- Doppler: renal artery/vein thrombosis
- CT abdomen/pelvis (non-contrast): calculi, retroperitoneal pathology
- Chest X-ray: pulmonary oedema
Renal Biopsy: Indicated when cause is unclear after initial workup, especially when glomerulonephritis or vasculitis is suspected.
Novel Biomarkers (early AKI detection):
- NGAL (neutrophil gelatinase-associated lipocalin)
- KIM-1 (kidney injury molecule-1)
- Cystatin C
- IL-18
- TIMP-2 × IGFBP7 (NephroCheck®)
4. PRINCIPLES OF MANAGEMENT
A. NON-PHARMACOLOGICAL
- Fluid management: Aggressive IV fluid resuscitation for hypovolaemia (isotonic saline or balanced crystalloids); avoid fluid overload. Fluid balance strictly monitored.
- Dietary modification:
- Restrict protein (0.6–0.8 g/kg/day in non-dialysis AKI to reduce urea generation)
- Restrict potassium, phosphorus, sodium
- Adequate calories (25–35 kcal/kg/day) — enteral nutrition preferred
- Avoidance of nephrotoxins: Withhold NSAIDs, aminoglycosides, contrast agents, ACE inhibitors/ARBs in the acute setting; dose-adjust all renally cleared drugs.
- Monitoring: Strict intake/output, daily weights, cardiac monitoring (hyperkalaemia), blood pressure control.
- Treat underlying cause: Relieve obstruction (catheterisation, nephrostomy), treat sepsis, remove nephrotoxic agents.
- Renal Replacement Therapy (RRT) — non-pharmacological intervention:
- Indications (AEIOU): Acidosis, Electrolyte disturbance (refractory hyperkalaemia), Ingestion/toxin, Overload (pulmonary oedema), Uraemia (symptomatic — pericarditis, encephalopathy)
- Modalities: Intermittent Haemodialysis (IHD) or Continuous Renal Replacement Therapy (CRRT — preferred in haemodynamically unstable patients)
B. PHARMACOLOGICAL
| Indication | Drug/Intervention |
|---|---|
| Prerenal hypotension | IV isotonic saline / balanced crystalloids; vasopressors (norepinephrine) in septic shock |
| Hyperkalaemia | IV calcium gluconate (membrane stabilisation); IV insulin + dextrose; sodium bicarbonate; calcium resonium/patiromer (exchange resins); dialysis for refractory cases |
| Metabolic acidosis | IV sodium bicarbonate (pH <7.1 or HCO₃⁻ <12 mEq/L) |
| Pulmonary oedema (volume overload) | IV furosemide (loop diuretic — converts oliguria, facilitates fluid management but does NOT improve outcome) |
| Sepsis-AKI | Broad-spectrum antibiotics; early goal-directed therapy |
| Contrast-induced AKI prophylaxis | IV N-acetylcysteine; adequate pre- and post-hydration; use iso-osmolar contrast |
| Hyperuricaemia (tumour lysis) | Rasburicase / allopurinol + aggressive hydration |
| Uremic bleeding | Desmopressin (DDAVP); dialysis |
| Anaemia | Erythropoiesis-stimulating agents (ESA) if prolonged; transfusion if severe |
Note: Dopamine ("renal dose") is NOT recommended — no proven benefit in AKI.
PART II — CHIRAKAARI VRIKKA-NISHKRIYATA (Chronic Renal Failure / Chronic Kidney Disease)
1. DEFINITION
Chronic Kidney Disease (CKD) is defined as abnormalities of kidney structure or function, present for >3 months, with implications for health.
Diagnostic criteria (either one for >3 months):
- GFR < 60 mL/min/1.73 m²
- Markers of kidney damage: albuminuria (≥30 mg/24h), abnormal urinary sediment, electrolyte abnormalities due to tubular disorders, structural abnormality on imaging, history of kidney transplantation
KDIGO Staging of CKD
| Stage | GFR (mL/min/1.73 m²) | Description |
|---|---|---|
| G1 | ≥90 | Normal/High (with markers of damage) |
| G2 | 60–89 | Mildly decreased |
| G3a | 45–59 | Mildly–moderately decreased |
| G3b | 30–44 | Moderately–severely decreased |
| G4 | 15–29 | Severely decreased |
| G5 | <15 | Kidney failure (ESKD); dialysis/transplant |
Albuminuria categories (A1: <30, A2: 30–300, A3: >300 mg/g) further risk-stratify.
2. ETIOPATHOGENESIS — CHART
Common Causes
CAUSES OF CKD (Global)
│
├── DIABETES MELLITUS (most common worldwide — ~40%)
│ └── Diabetic nephropathy: glomerulosclerosis (Kimmelstiel-Wilson lesion)
│ microalbuminuria → proteinuria → GFR decline
│
├── HYPERTENSION (~25–30%)
│ └── Hypertensive nephrosclerosis: afferent arteriolar thickening,
│ glomerular ischaemia, tubular atrophy, interstitial fibrosis
│
├── GLOMERULONEPHRITIS (~10–15%)
│ ├── IgA nephropathy, Focal segmental glomerulosclerosis (FSGS)
│ ├── Membranous nephropathy, Lupus nephritis
│ └── ANCA-associated vasculitis
│
├── HEREDITARY / GENETIC
│ ├── ADPKD (Autosomal Dominant Polycystic Kidney Disease)
│ └── Alport syndrome, Fabry disease
│
├── OBSTRUCTIVE NEPHROPATHY
│ └── Chronic BPH, renal calculi, posterior urethral valves
│
├── CHRONIC TUBULOINTERSTITIAL NEPHRITIS
│ └── Chronic analgesic use, heavy metals (lead, cadmium), sickle cell
│
└── RECURRENT AKI → progressive CKD
Pathogenetic Mechanism (Common Final Pathway)
Any Initiating Injury (DM, HTN, GN, etc.)
↓
Nephron loss → Compensatory hyperfiltration in remaining nephrons
↓
Intraglomerular hypertension → Glomerular hypertrophy
↓
Proteinuria → Tubulo-interstitial inflammation
↓
TGF-β activation → Fibroblast proliferation
↓
Glomerulosclerosis + Tubular atrophy + Interstitial fibrosis
↓
Further nephron loss → Self-perpetuating cycle
↓
End-Stage Kidney Disease (ESKD)
Key mediators of progression: Angiotensin II (intrarenal), TGF-β1, RAAS activation, oxidative stress, proteinuria itself (tubular toxicity), systemic and intraglomerular hypertension.
3. DIAGNOSIS
A. CLINICAL FEATURES
Early CKD (Stages 1–3): Usually asymptomatic; detected on screening (incidental lab findings).
Advanced CKD (Stages 4–5) — Uraemic Syndrome:
| System | Manifestations |
|---|---|
| General | Fatigue, anorexia, nausea, weight loss, pruritis |
| CVS | Hypertension, LVH, pericarditis, accelerated atherosclerosis, arrhythmias |
| CNS | Lethargy, cognitive impairment, peripheral neuropathy, restless leg syndrome, uraemic encephalopathy |
| GIT | Anorexia, nausea, vomiting, peptic ulceration, GI bleeding (platelet dysfunction) |
| Haematological | Normochromic normocytic anaemia (↓ EPO), bleeding tendency, thrombocytopenia |
| Musculoskeletal | Renal osteodystrophy (osteoporosis, osteomalacia, osteitis fibrosa cystica), fractures, myopathy |
| Endocrine | Hyperparathyroidism (secondary → tertiary), hypogonadism, amenorrhoea, impotence, hypothyroidism |
| Fluid/Electrolyte | Oedema, hyperkalaemia, hyperphosphataemia, hypocalcaemia, hypermagnesaemia, metabolic acidosis |
| Skin | Pallor (anaemia), uraemic frost (severe), pruritus, hyperpigmentation |
| Immune | Immunosuppression → susceptibility to infections |
B. INVESTIGATIONS
Blood Tests:
- Serum creatinine + eGFR (CKD-EPI or MDRD equation)
- BUN, electrolytes (K⁺ ↑, Na⁺ variable, phosphate ↑, calcium ↓)
- Bicarbonate ↓ (metabolic acidosis)
- CBC: normochromic normocytic anaemia; ↓ reticulocytes
- Serum PTH ↑ (secondary hyperparathyroidism), Vitamin D ↓
- Fasting lipids, blood glucose / HbA1c
- Serum albumin (marker of nutritional status/inflammation)
Urine Tests:
- Spot urine albumin:creatinine ratio (ACR) or protein:creatinine ratio (PCR) — performed twice
- Urinalysis: proteinuria, haematuria, casts
- 24-hour urine collection (when needed for GFR estimation)
Imaging:
- Renal ultrasound: bilateral small, echogenic kidneys (most CKD); loss of corticomedullary differentiation; exceptions: DM (kidneys may be normal/large early), ADPKD (markedly enlarged, cystic)
- DMSA scan: differential renal function, scarring
- CT KUB: structural anomalies, obstruction, calculi
Renal Biopsy: Indicated in CKD with suspected glomerular cause, unexplained rapid progression, or when nephrotic syndrome is present; generally avoided when kidneys are small.
ECG: Hyperkalaemic changes (peaked T waves, widened QRS, sine wave pattern).
4. PRINCIPLES OF MANAGEMENT
A. NON-PHARMACOLOGICAL
-
Dietary modification:
- Low protein diet (0.6–0.8 g/kg/day) — reduces uraemia and slows progression
- Sodium restriction (<2 g/day) — BP control, oedema
- Potassium restriction (if hyperkalaemic)
- Phosphate restriction (<800 mg/day); avoid phosphate-rich foods (dairy, nuts, processed food)
- Adequate caloric intake (35 kcal/kg/day)
- Fluid restriction (in advanced CKD)
-
Lifestyle modifications:
- Smoking cessation (independent risk factor for progression)
- Regular moderate exercise
- Weight reduction (BMI <25)
- Alcohol moderation
-
BP control target: <130/80 mmHg (or <125/75 if proteinuria >1 g/day)
-
Avoidance of nephrotoxins: NSAIDs, contrast dye, herbal nephrotoxins, aminoglycosides
-
Patient education & self-management: Home BP monitoring, understanding signs of decompensation, fluid balance logs
-
Renal Replacement Therapy (RRT) — when GFR <15 or symptomatic uraemia:
- Haemodialysis (HD): 3× weekly, 3–4 hours; requires arteriovenous fistula
- Peritoneal Dialysis (PD): CAPD or APD; home-based; better for residual renal function preservation
- Renal Transplantation: Treatment of choice for ESKD; best long-term outcomes
B. PHARMACOLOGICAL
| Problem | Drug / Strategy |
|---|---|
| Slow progression | ACE inhibitors / ARBs — reduce intraglomerular pressure, reduce proteinuria (first-line in DM-CKD and proteinuric CKD) |
| SGLT2 inhibitors (empagliflozin, dapagliflozin) — reduce CKD progression and cardiovascular events (now guideline-recommended) | |
| Finerenone (non-steroidal MRA) — reduce CKD progression in DM | |
| Hypertension | ACE inhibitors/ARBs (first-line); CCBs, beta-blockers as add-on |
| Anaemia | Erythropoiesis-stimulating agents (ESA — darbepoetin, epoetin); IV iron (if ferritin <200 µg/L or TSAT <20%) — target Hb 10–12 g/dL |
| Hyperphosphataemia | Calcium carbonate (calcium-based binders); Sevelamer (non-calcium); lanthanum carbonate; iron-based binders |
| Secondary HPT | Calcitriol (activated Vit D) or analogues (paricalcitol); Cinacalcet (calcimimetic — for tertiary HPT) |
| Metabolic acidosis | Sodium bicarbonate supplementation (target HCO₃⁻ ≥22 mEq/L) |
| Hyperkalaemia | Dietary restriction; loop diuretics; sodium/potassium exchange resins (patiromer, sodium zirconium cyclosilicate) |
| Oedema / volume overload | Loop diuretics (furosemide — higher doses needed as GFR falls); thiazides lose efficacy when GFR <30 |
| Dyslipidaemia | Statins (atorvastatin, rosuvastatin) — reduce CV events in CKD |
| Diabetes control | Metformin (discontinue if GFR <30); SGLT2 inhibitors (adjust for GFR); insulin; avoid nephrotoxic oral hypoglycaemics |
| Infections | Vaccinations: Influenza (annual), Pneumococcal, Hepatitis B |
| Renal bone disease | Phosphate binders + Vitamin D analogues + Cinacalcet; bisphosphonates (use with caution in CKD) |
PART III — AYURVEDIC PERSPECTIVE
Conceptual Mapping
| Modern Term | Ayurvedic Equivalent |
|---|---|
| Kidney | Vrikka (a pair; embryologically derived from Rakta + Meda dhatu) |
| Acute Renal Failure | Ashu Vrikka-Nishkriyata (sudden / rapid cessation of kidney function) |
| Chronic Renal Failure | Chirakaari Vrikka-Nishkriyata (prolonged, gradual decline of kidney function) |
| Urine formation channels | Mutravaha Srotas |
| Urinary bladder | Basti (also the main seat of Vata) |
| Waste filtration | Kleda-vahana (kleda = excess fluid/moist waste) |
Dosha-Dushya Analysis
Pradhana Dosha: Tridosha derangement, with Vata-Kapha predominance (especially in CRF); Pitta involvement in inflammatory/haemorrhagic causes.
Dushya (affected tissues/channels):
- Rakta dhatu (blood tissue) — kidney's embryological origin
- Meda dhatu (fat/lipid tissue) — Vrikka moolasthana
- Mutravaha Srotas — channels of urine formation/excretion
Srotodushti (channel pathology): Primarily Sanga (obstruction) → Vimargagamana (misdirection of flow)
ASHU VRIKKA-NISHKRIYATA — Etiopathogenesis (Samprapti)
NIDANA (Causative Factors):
├── Ahara: Ati-ruksha (excessively dry food), Kshara (alkaline/caustic substances),
│ Ati-lavana (excessive salt), Viruddha ahara, dehydrating foods
├── Vihara: Trauma, excessive exertion, haemorrhage, suppression of natural urges (vegadharana)
└── Vyadhi: Infections (jwara), toxins (visha), haemolysis, post-surgical states
↓
PURVARUPA (Prodromal signs):
Reduced urine output, lower back discomfort, fatigue
↓
SAMPRAPTI (Pathogenesis):
Nidana Sevana
↓
Vata-Pitta vitiation
(Vata: governs urine flow / filtration; Pitta: metabolic fire)
↓
Mutravaha Srotas Dushti (obstruction/damage)
↓
Kleda (fluid waste) fails to be eliminated
↓
Toxin accumulation (Ama formation) → Srotosanga
↓
Agnimandya (impaired metabolic fire) → further Ama
↓
Rapid Vrikka Kshaya (acute kidney dysfunction)
↓
RUPA (Manifestations):
Anuria/Oliguria, Shotha (oedema), Aruchi, Chardi, Bhrama,
Klama, Sandhi shoola (uremic musculoskeletal pain)
CHIRAKAARI VRIKKA-NISHKRIYATA — Etiopathogenesis (Samprapti)
NIDANA:
├── Ahara: Guru-Snigdha-Sheeta-Abhisyandi (heavy, oily, cold, congestive) foods
│ → Kapha/Meda vitiation; Ati-lavana-amla-teekshna → Rakta-Pitta vitiation
├── Vihara: Sedentary lifestyle, day-sleep (Divaswapna → Kapha accumulation)
├── Vyadhi: Madhumeha (diabetes), Raktachapa (hypertension), Mutrashmari (calculi),
│ repeated AKI episodes, Beejadushti (genetic factors / ADPKD)
└── Manasika: Chronic stress → Vata derangement
↓
SAMPRAPTI:
Nidana Sevana
↓
Tridosha vitiation (Vata-Kapha predominant)
↓
Rakta + Meda Dushti (primary dhatu affected — kidney's origin)
↓
Medovaha + Mutravaha Sroto Dushti (Srotosanga + Srotodushti)
↓
Agnimandya → Ama Utpatti (toxic metabolic byproducts)
↓
Progressive Vrikka Kshaya (nephron loss / fibrosis)
↓
Kleda accumulation (uraemic toxins, fluid retention)
↓
RUPA: Pandu (anaemia), Shopha (oedema), Aruchi, Chardi,
Mootravaha srotas dushti (oliguria/polyuria), Sarvangavedana,
Twaka rukshata (dry skin), Hrudroga (cardiovascular), Daurbalya
↓
Yapya/Asadhya (incurable/palliable) stage = ESKD
AYURVEDIC TREATMENT PRINCIPLES
Chikitsa Sutra (Treatment Goals)
Break the Samprapti → Achieve: Ama pachana + Sroto shodhana + Rakta prasadana + Kleda-medososhana + Doshic balance + Rasayana chikitsa
SHODHANA CHIKITSA (Bio-Purification / Panchakarma)
Indicated when the patient has adequate bala (strength); best in early-to-moderate stages.
1. Purva Karma (Preparatory Procedures)
| Procedure | Detail |
|---|---|
| Snehana (Internal/External Oleation) | Medicated ghee/oil (e.g., Mahatiktaka ghrita, Dhanwantaram taila) — liquefies and mobilises Ama |
| Swedana (Sudation) | Avgaha Sweda (medicated sitz bath with Punarnava kwatha, dashamoola) — particularly suited to renal conditions; opens Srotas, promotes elimination through skin |
2. Pradhana Karma (Main Procedures)
| Panchakarma | Relevance to Vrikka-Nishkriyata |
|---|---|
| Virechana (Purgation) | For Pitta-predominant/inflammatory AKI; eliminates Ama, Pitta; uses Trivrut leha, Eranda taila; clears Mutravaha srotas indirectly via Pakwashaya shodhana |
| Basti (Medicated Enema) | MOST IMPORTANT — Vata's primary seat is Pakwashaya (colon); Basti pacifies Vata, the dominant dosha in both AKI/CRF; achieves systemic Shodhana without over-taxing kidneys |
| → Niruha Basti (Kashaya Basti) | Punarnava Kwatha Basti; Dashamoola Kwatha Basti — decoction enema for Srotoshodhana |
| → Anuvasana Basti (Sneha Basti) | Dhanwantaram oil; Ksheerabala oil — nourishes, lubricates, Vata-shamaka |
| Abhyanga (Medicated Oil Massage) | Dhanwantaram taila, Ksheerabala taila — promotes circulation, Vata pacification |
| Virechana + Basti (Yoga Basti cycle) | 8-day cycle: 3 Anuvasana + 5 Niruha Basti — standard protocol in CRF management |
Note: Vamana (emesis) is generally contraindicated in severe renal failure with hypovolaemia. Raktamokshana (bloodletting — jalauka/leech therapy) may be considered in Pitta-dominant/inflammatory cases.
SHAMANA CHIKITSA (Palliative / Conservative Treatment)
Used alone in debilitated patients; used after Shodhana as maintenance.
Key Therapeutic Strategies
| Goal | Intervention |
|---|---|
| Ama pachana (Digest toxins) | Ginger (Shunti), Pippali, Haritaki, Trikatu churna |
| Mutral (Diuretic) | Punarnava, Gokshura, Varuna (Crataeva nurvala), Pashanabheda (Bergenia ligulata) |
| Srotoshodhana (Channel cleansing) | Manjistha, Chandana, Ushira (Vetiver) |
| Rakta prasadana (Blood purification) | Manjistha, Neem, Guduchi (Tinospora cordifolia) |
| Vata-Kapha Shamana | Punarnava, Shilajatu, Gokshura |
| Anti-inflammatory / nephroprotective | Guduchi (Tinospora cordifolia), Amalaki, Bhumyamalaki (Phyllanthus niruri) |
| Rasayana (Regenerative/Tonic) | Shilajatu, Chyawanprash, Ashwagandha, Punarnava mandura (for anaemia) |
Key Ayurvedic Formulations
| Formulation | Composition / Use |
|---|---|
| Punarnavashtaka Kashaya | Punarnava, dashamoola, ginger etc. — diuretic, anti-oedematous, Vata-Kapha shamaka |
| Gokshuradi Guggulu | Gokshura, Guggulu, Trikatu — mutral, anti-inflammatory, breaks Srotosanga |
| Varuna / Varunadya Kashaya | Crataeva nurvala — mutra-shodaka (urine purifier), dissolves calculi |
| Chandraprabha Vati | Multi-herbal — urinary tonic, metabolic regulator |
| Punarnava Mandura | Punarnava + Mandura (iron) — anaemia of CKD (renal anaemia / Pandu) |
| Mutrakrichhantaka Rasa | Rasa preparation — acute urinary obstruction/AKI with dysuria |
| Shilajatu (Asphaltum) | Rasayana — improves glomerular function, anti-oxidant, adaptogen |
| Bhumyamalaki (Phyllanthus niruri) | Hepato-nephroprotective — reduces proteinuria, antiviral |
| Guduchi Satva | Tinospora cordifolia extract — immunomodulator, anti-uraemic |
Specific Treatment of Ashu Vrikka-Nishkriyata (AKI)
| Phase | Ayurvedic Approach |
|---|---|
| Acute phase (Initiation/Oliguric) | Shodhana deferred; focus on: Ama pachana (Ginger, Haritaki), Sroto unblocking (Punarnavashtaka), IV fluid equivalent = Yavagu (rice gruel), light easily digestible diet; Vastika dravyas (diuretics) cautiously |
| Diuretic phase | Rasayana + rehydration; Balya (strengthening) therapy begins |
| Recovery | Rasayana (Chyawanprash, Ashwagandha), dietary restoration, Yoga/Pranayama |
Specific Treatment of Chirakaari Vrikka-Nishkriyata (CRF/CKD)
| Stage | Ayurvedic Approach |
|---|---|
| Early (G1-G2) | Nidana Parivarjana (remove causative factors); Pathya Ahara-Vihara; Mutral + Rasayana; Shodhana (if bala adequate) |
| Moderate (G3) | Basti (Yoga basti), Virechana; Shamana — Punarnava, Gokshura, Guduchi, Chandraprabha; Manage Pandu with Punarnava Mandura |
| Advanced (G4-G5) | Primarily Shamana + Rasayana; Basti (Matra Basti with small quantities of medicated oil — safer); Ahara and Vihara adjustments; Integrate with dialysis if on RRT |
| ESKD | Palliative Ayurveda — symptom relief (pruritus: medicated oil massage; nausea: ginger; fatigue: Ashwagandha); supportive alongside RRT/transplant |
Pathya (Recommended Diet & Lifestyle)
- Light, warm, easily digestible food (Laghu, Ushna Ahara)
- Yava (barley), Old rice (Purana shali), Moong dal
- Bitter vegetables (karela/bitter gourd — Tikta rasa cleanses Rakta/Pitta)
- Avoid: Excess salt (Lavana), sour (Amla), heavy (Guru), cold, processed, dairy (Abhisyandi)
- Adequate hydration (unless oliguric)
- Mild Yoga: Pranayama (Anulom-Vilom), Bhujangasana, Setu Bandhasana
- Avoid: Divaswapna (day sleep), holding natural urges, excessive exertion
Summary Comparison Table
| Feature | Ashu Vrikka-Nishkriyata (ARF/AKI) | Chirakaari Vrikka-Nishkriyata (CRF/CKD) |
|---|---|---|
| Onset | Sudden (hours–days) | Gradual (>3 months) |
| Reversibility | Potentially reversible | Usually irreversible; progressive |
| Kidney size (USG) | Normal to enlarged | Small, echogenic |
| Creatinine | Rapidly rising | Chronically elevated |
| Anaemia | Mild/absent (acute) | Prominent (↓ EPO) |
| Osteodystrophy | Absent | Present (secondary HPT) |
| Ayurvedic predominant dosha | Vata-Pitta | Vata-Kapha |
| Primary Shodhana | Basti (Niruha + Anuvasana) | Basti (Yoga Basti) + Virechana |
| Key herbs | Punarnava, Varuna, Gokshura | Punarnava, Gokshura, Guduchi, Shilajatu |
| Rasayana | Post-recovery phase | Central to long-term management |
| RRT equivalent | Acute Basti + Virechana (elimination) | Dialysis + Basti (maintenance) |
Sources: Sabiston Textbook of Surgery 21e, National Kidney Foundation Primer on Kidney Diseases 8e, Brenner & Rector's The Kidney 2-Volume Set, KDIGO AKI Guidelines 2012; Ayurvedic content synthesized from IJCRT 2024 (Pathogenesis of CKD in Ayurveda), WJPLS 2025 (Vrikka Vikara management), DOAJ case reports on Shodhana-Shamana in CKD.
This is a shared conversation. Sign in to Orris to start your own chat.