Headd and Neck manifestation of HIV disease in detail for 20 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
HIV "head and neck" manifestations otolaryngology
HIV oral manifestations candidiasis hairy leukoplakia
HIV otolaryngology HAART antiretroviral therapy outcomes
HIV oral candidiasis hairy leukoplakia Kaposi sarcoma
HIV neck lymphadenopathy sinus disease recent advances
HIV associated lymphoma head neck non-Hodgkin
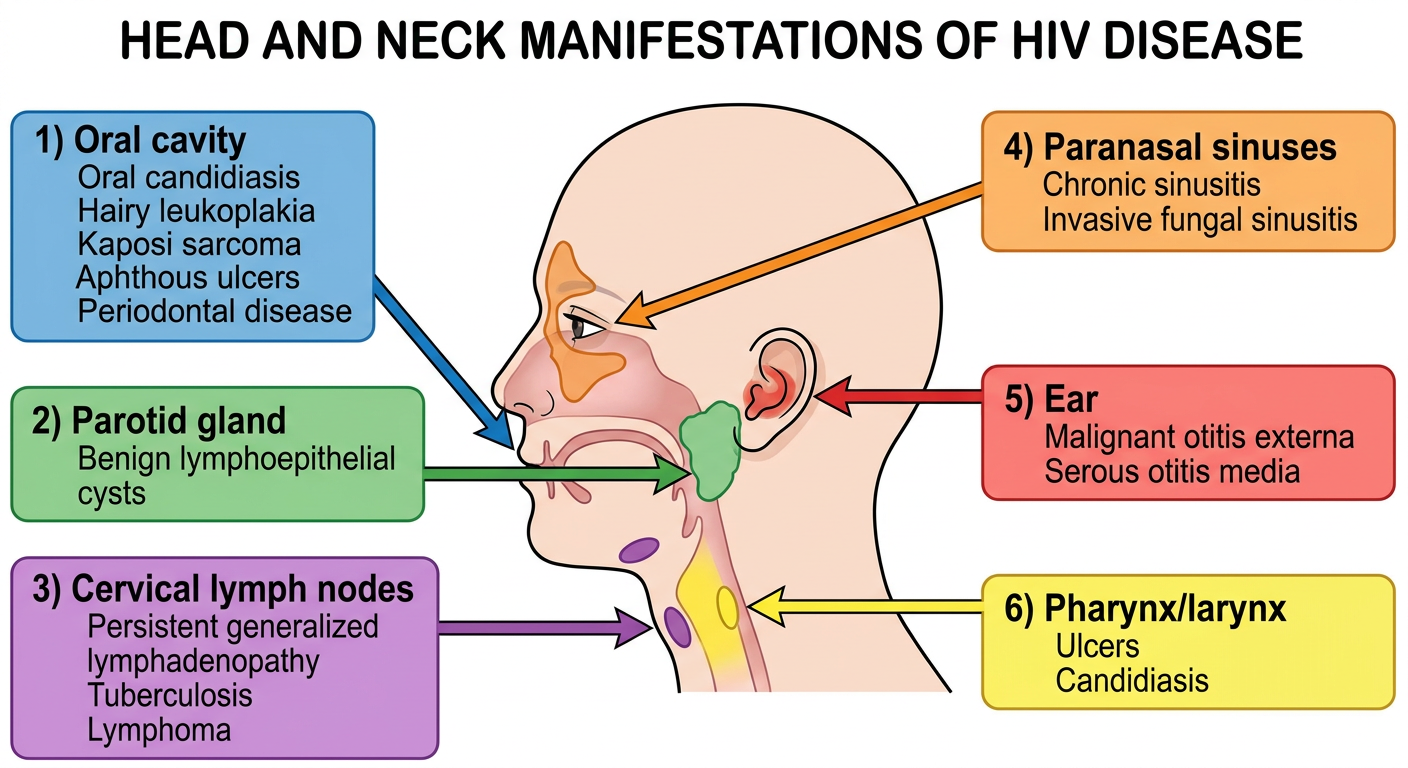
Medical diagram showing head and neck manifestations of HIV disease. Anatomical diagram of a human head and neck in profile view with labeled arrows pointing to different sites: 1) Oral cavity - showing oral candidiasis, hairy leukoplakia, Kaposi sarcoma, aphthous ulcers, periodontal disease. 2) Parotid gland - benign lymphoepithelial cysts. 3) Cervical lymph nodes - persistent generalized lymphadenopathy, tuberculosis, lymphoma. 4) Paranasal sinuses - chronic sinusitis, invasive fungal sinusitis. 5) Ear - malignant otitis externa, serous otitis media. 6) Pharynx/larynx - ulcers, candidiasis. Clean medical illustration style with colored text boxes and connecting lines, white background, educational medical poster format.
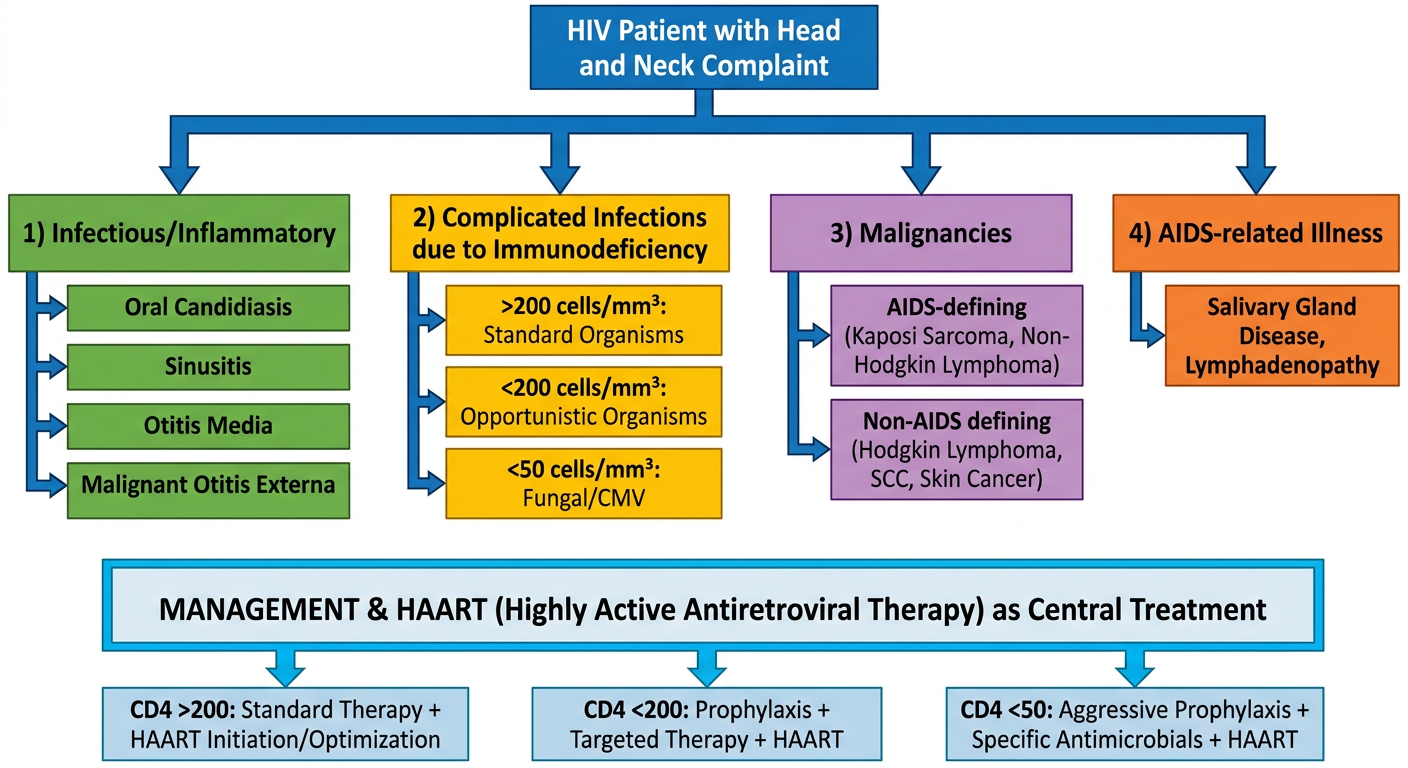
Medical flowchart showing classification and management of HIV Head and Neck Manifestations. Top box: "HIV Patient with Head and Neck Complaint". Branches into 4 categories: 1) Infectious/Inflammatory (oral candidiasis, sinusitis, otitis media, malignant otitis externa), 2) Complicated Infections due to Immunodeficiency (based on CD4 count: >200 cells/mm3 standard organisms, <200 opportunistic organisms, <50 fungal/CMV), 3) Malignancies - AIDS-defining (Kaposi Sarcoma, Non-Hodgkin Lymphoma) and Non-AIDS defining (Hodgkin Lymphoma, SCC, skin cancer), 4) AIDS-related illness. Bottom section showing management based on CD4 count with HAART as central treatment. Clean flowchart with colored boxes and connecting arrows, medical educational style.
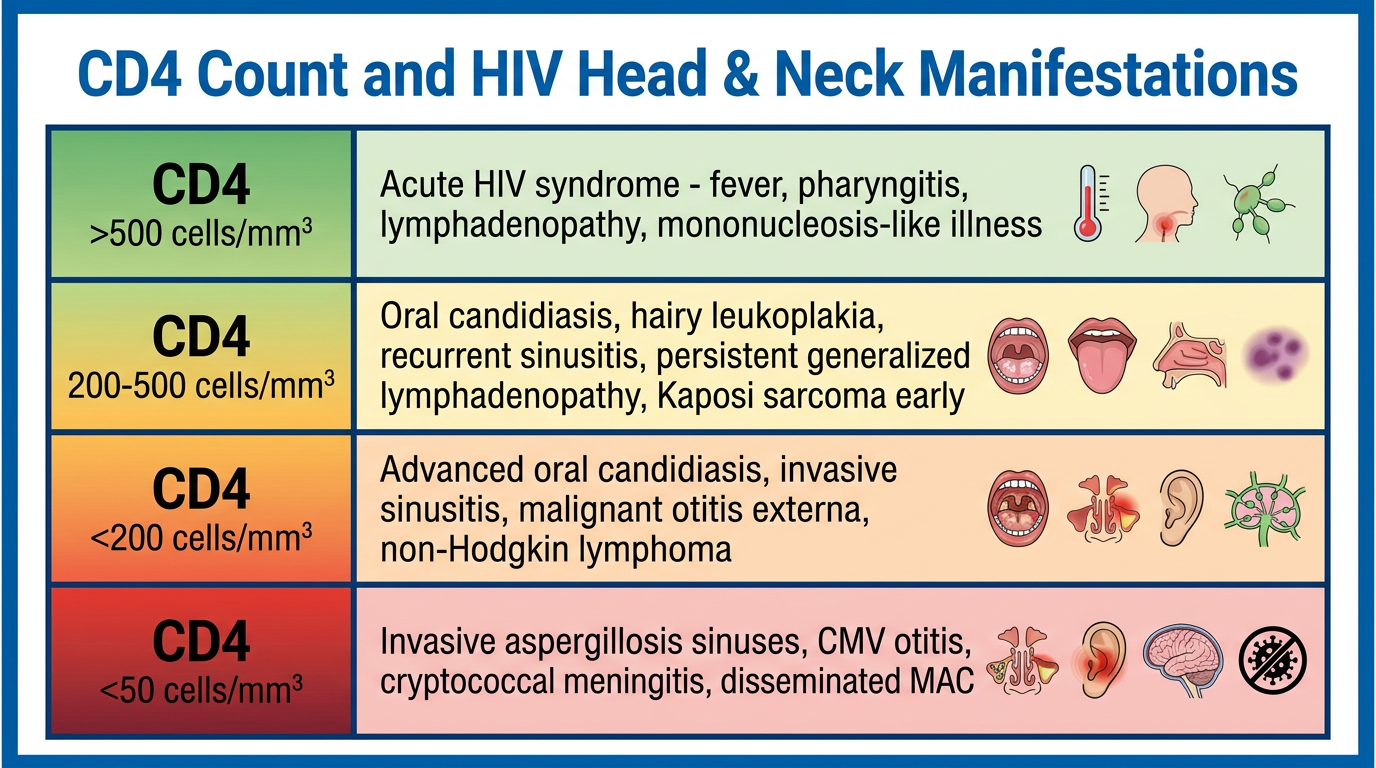
Medical table/diagram: "CD4 Count and HIV Head & Neck Manifestations" - A horizontally organized medical reference chart showing three tiers. Row 1 (CD4 >500 cells/mm3): Acute HIV syndrome - fever, pharyngitis, lymphadenopathy, mononucleosis-like illness. Row 2 (CD4 200-500 cells/mm3): Oral candidiasis, hairy leukoplakia, recurrent sinusitis, persistent generalized lymphadenopathy, Kaposi sarcoma early. Row 3 (CD4 <200 cells/mm3): Advanced oral candidiasis, invasive sinusitis, malignant otitis externa, non-Hodgkin lymphoma. Row 4 (CD4 <50 cells/mm3): Invasive aspergillosis sinuses, CMV otitis, cryptococcal meningitis, disseminated MAC. Each tier in different color gradient from green to red. Clean medical table format with borders and icons.
HEAD AND NECK MANIFESTATIONS OF HIV DISEASE
(20-Mark Answer - RGUHS Standard)
INTRODUCTION
DIAGRAM 1: Anatomical Sites of HIV Head and Neck Manifestations
CLASSIFICATION (KJ Lee's / Cummings)
- Infectious/Inflammatory conditions as a result of immunodeficiency
- Complicated infections as a result of immunodeficiency
- Malignancy related to immunodeficiency
- AIDS-related illness (systemic conditions with head and neck involvement)
FLOWCHART: Classification and Management of HIV Head and Neck Manifestations
CD4 COUNT AND CLINICAL STAGING (WHO 2007)
A. ORAL CAVITY MANIFESTATIONS
1. Oral Candidiasis (Thrush)
- Pseudomembranous form (thrush): White plaques on buccal mucosa, tongue, palate - easily wiped off leaving erythematous base
- Erythematous (atrophic) form: Red patches on hard/soft palate and dorsal tongue
- Angular cheilitis: Cracking and erythema at oral commissures
- Caused by Candida albicans
- Treatment: Topical nystatin or clotrimazole; systemic fluconazole for refractory cases
- Presence of oral candidiasis in an otherwise healthy adult is an indicator for HIV testing (Scott-Brown's Vol 1)
2. Oral Hairy Leukoplakia (OHL)
- White, corrugated/hairy lesions on the lateral borders of the tongue - cannot be wiped off (unlike candida)
- Caused by Epstein-Barr Virus (EBV) reactivation
- A pathognomonic indicator of HIV infection - occurrence strongly suggests CD4 count <300
- Virtually diagnostic: biopsy shows hyperparakeratosis with "hair-like" projections and koilocytic cells
- Treatment: Responds to HAART; topical retinoids or acyclovir for symptom relief
- Dhingra (Diseases of Ear, Nose and Throat): Listed as a hallmark opportunistic oral lesion in AIDS patients
3. Aphthous Ulcers
- Major aphthous ulcers - larger (>1 cm), deeper, more painful, more frequent in HIV
- Classified as: Minor (<1 cm), Major (>1 cm), and Herpetiform
- Etiology unclear; may relate to immune dysregulation
- Treatment: Topical corticosteroids (triamcinolone paste), thalidomide for severe/refractory cases
4. Periodontal Disease
- Linear Gingival Erythema (LGE): Fiery red band at the gingival margin, out of proportion to plaque, persists despite scaling
- Necrotizing Ulcerative Gingivitis/Periodontitis/Stomatitis (NUG/NUP/NUS): Progressive recession, bleeding, tissue sloughing, malodor, loss of interdental papillae - a spectrum of the same pathology
- Management: Chlorhexidine + nystatin mouthwash topically; dental referral; debridement of necrotic tissue; systemic metronidazole for failure
B. SALIVARY GLAND MANIFESTATIONS
Benign Lymphoepithelial Cysts (BLECs) / Parotid Cysts
- Most common parotid lesion in HIV patients (approximately 75% of parotid lesions)
- Parotid is most commonly affected due to intraparotid lymph nodes (KJ Lee's, p. 236)
- Particularly prevalent in pediatric HIV patients - up to 18% of presenting complaints
- Bilateral in up to 80% of cases (though may present unilaterally clinically)
- Etiology: viral inflammation causing cystic transformation of intraparotid lymph nodes
- Present asymptomatically; compression of parotid ducts can cause pain/sialadenitis
- Cervical lymphadenopathy is present in up to 70-80% of cases simultaneously
- Diagnosis: FNA (cytology), CT/MRI, ultrasound
- Treatment: HAART leads to regression; aspiration for cosmesis; sclerotherapy; surgery rarely required
- Must exclude: lymphoma, Kaposi sarcoma, metastatic cutaneous malignancy
Diffuse Infiltrative Lymphocytosis Syndrome (DILS)
- CD8+ lymphocytic infiltration of salivary glands causing bilateral parotid swelling
- Associated with sicca symptoms (dry mouth, dry eyes)
- Differs from Sjogren's syndrome serologically (anti-Ro, anti-La negative)
C. CERVICAL LYMPHADENOPATHY
- Defined as lymphadenopathy >1 cm in 2 or more extra-inguinal sites, lasting >3 months
- Cervical nodes most commonly involved
- Nodes: small, symmetrical, non-tender
- Biopsy reveals follicular hyperplasia - no specific treatment required
- Occurs in up to 70% of patients in the asymptomatic phase (Scott-Brown's Vol 1, p. 278)
- Non-Hodgkin's lymphoma (NHL)
- Hodgkin's lymphoma
- Tuberculosis (the most important opportunistic infection to exclude in India)
- Kaposi's sarcoma nodal involvement
- Syphilis
- Metastatic solid organ malignancy
D. NOSE AND PARANASAL SINUS MANIFESTATIONS
Rhinitis and Nasal Obstruction
- Adenoidal hypertrophy can cause nasal obstruction and recurrent otitis media
- Any non-pediatric patient with adenoid hypertrophy should be tested for HIV (Scott-Brown's)
- Hypertrophy of any Waldeyer's ring tissue may occur
- KS and Non-Hodgkin's lymphoma can arise in the nasal cavity/nasopharynx
- KS can also arise from the nasal septum
Sinusitis - CD4-dependent microbiology:
| CD4 Count | Predominant Organisms | Management |
|---|---|---|
| >200 cells/mm3 | S. pneumoniae, H. influenzae, M. catarrhalis (same as immunocompetent) | Standard antibiotics |
| <200 cells/mm3 | S. aureus, P. aeruginosa, anaerobes added | Broadened antibiotics |
| <50 cells/mm3 | Aspergillus (most common), CMV, Microsporidia, Acanthamoeba castellani, Legionella | Antifungals (IV amphotericin B) |
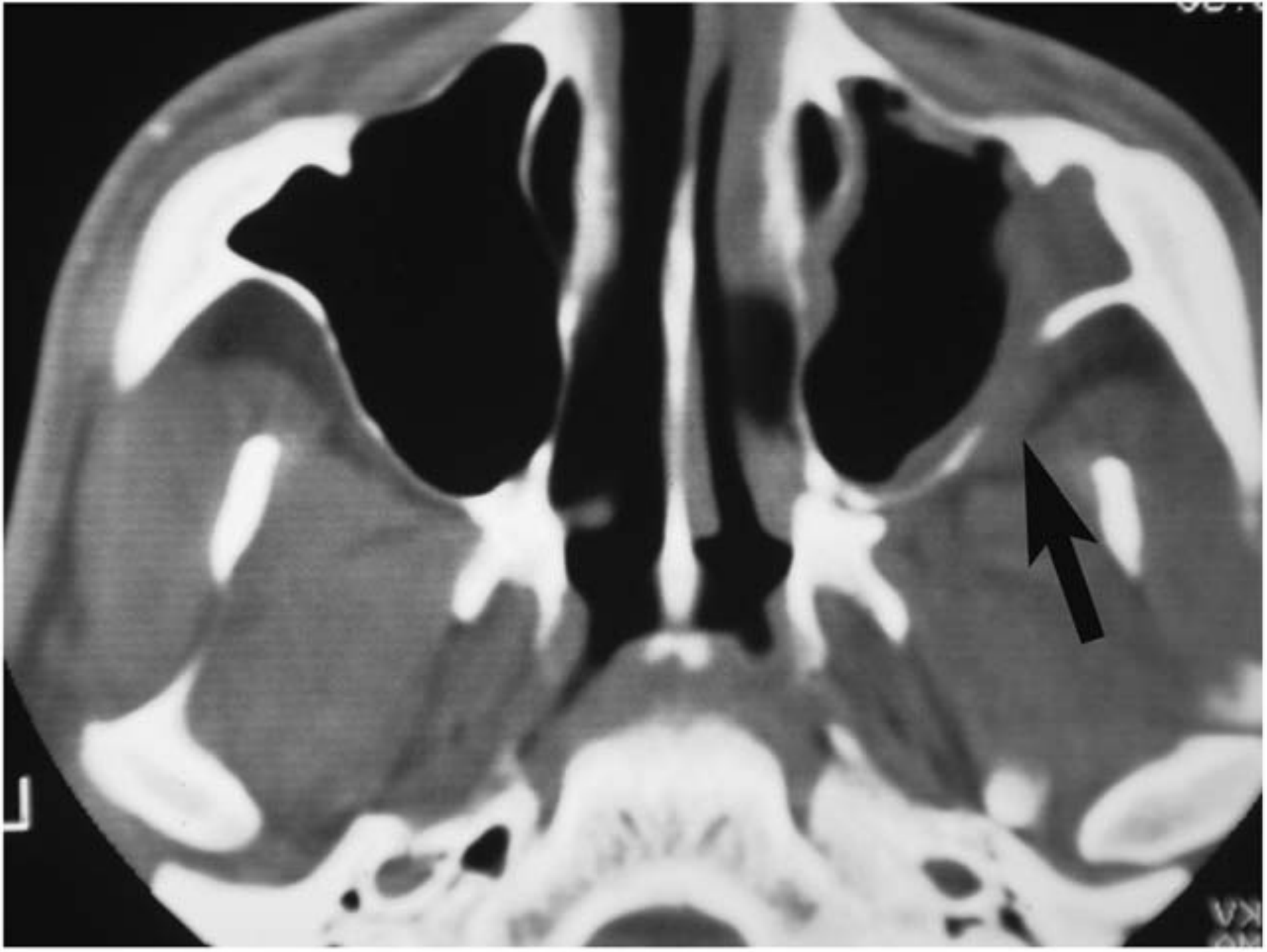
Invasive Fungal Sinusitis
- Occurs with CD4 <50 cells/mm3
- Most feared sinonasal complication - can be rapidly fatal
- Presents with facial pain, proptosis, periorbital swelling, cranial nerve palsies
- CT shows subtle bony erosion with extension into infratemporal fossa (see image below)
- Treatment: IV amphotericin B + aggressive surgical debridement
CT Scan - Invasive Fungal Sinusitis in Advanced HIV:
E. OTOLOGIC MANIFESTATIONS
External Ear
- Osteomyelitis of skull base causing facial nerve/cranial nerve dysfunction
- Causative agent: Pseudomonas aeruginosa (most common)
- In very low CD4 count: Aspergillus - invasive and potentially fatal
- Diagnosis: CT temporal bone or Technetium-99m bone scan
- Treatment: Pseudomonas: 6-8 weeks antipseudomonal antibiotics (3rd-gen cephalosporin + ciprofloxacin or aminoglycoside); Aspergillus: IV amphotericin B + surgical debridement
- Can infect external auditory canal, middle ear, and mastoid bone
- Presents as cyst or polyp; may occlude EAC or spread to middle cranial fossa
- Diagnosis: Biopsy
- Treatment: Trimethoprim/sulphamethoxazole ± dapsone
Middle Ear
- Most common otologic entities: serous and recurrent otitis media
- Etiologies: Eustachian tube dysfunction, nasopharyngeal neoplasms, adenoid hypertrophy, sinusitis/allergy
- Chronic otitis media and tympanic membrane perforations more prevalent in HIV-positive children in Sub-Saharan Africa
- Conductive and sensorineural hearing loss reported
Sensorineural Hearing Loss (SNHL)
- Multifactorial in HIV:
- Direct viral neurotoxicity to cochlea/auditory nerve
- Opportunistic infections (CMV, cryptococcal meningitis)
- Ototoxic medications (especially aminoglycosides, cisplatin used in treatment)
- CNS lymphoma
- Up to 49% of HIV-positive patients may have some degree of hearing loss
F. PHARYNGEAL AND LARYNGEAL MANIFESTATIONS
Pharyngitis
- A common presentation of acute HIV seroconversion syndrome (2-4 weeks post-exposure)
- Exudative or non-exudative pharyngitis mimicking EBV mononucleosis
- Associated with: fever, cervical lymphadenopathy, maculopapular rash, oropharyngeal ulcers, meningoencephalitis
- Heterophile antibody test (Monospot) is usually negative (key distinguishing feature)
- Any mononucleosis-like illness: offer HIV test (UK guidelines)
Larynx
- Candidal laryngitis - hoarseness, odynophagia, dysphonia
- KS of larynx - can cause airway compromise
- SCC of larynx - increased risk in HIV patients
- Herpes simplex laryngitis, CMV laryngitis in advanced disease
G. HIV-ASSOCIATED MALIGNANCIES OF THE HEAD AND NECK
1. AIDS-DEFINING MALIGNANCIES
Kaposi's Sarcoma (KS)
- Caused by Human Herpesvirus 8 (HHV-8)
- Incidence in HIV patients ~5%; 70% of all KS lesions occur in the head and neck
- Cummings Table (10.4): Most common sites: skin, oral mucosa, lymph nodes
- Clinical features:
- Skin: violaceous/brownish-red macules, papules, nodules - painless initially
- Oral mucosa: classically raised, red lesions on hard palate; may ulcerate
- Lesion size variable (mm to cm); may be flat, raised, or nodular
- Diagnosis: Clinical + biopsy (shows spindle cells, vascular spaces, HHV-8 staining)
- Treatment:
- HAART is the mainstay - immune recovery leads to regression
- Advanced disease: localized radiotherapy (good control, but HIV patients more prone to radiation side effects)
- Surgical excision for local control (recurrence common even with clear margins)
- Other options: topical retinoids, intralesional chemotherapy, laser coagulation, cryotherapy
- Marked decrease in incidence since introduction of HAART (Cummings, p. 4178)
AIDS-Related Non-Hodgkin Lymphoma (NHL)
- Head and neck involved in two-thirds of cases of AIDS-NHL
- Extranodal disease twice as common in AIDS-NHL compared to non-HIV-associated NHL
- Extranodal head and neck sites: oral cavity, sinonasal tract, salivary glands, Waldeyer's ring
- More likely to have advanced disease at presentation
- Plasmablastic lymphoma: A rare aggressive B-cell lymphoma strongly associated with HIV, primarily arises in oral cavity - reviewed by Xu et al., 2025 in Head Neck journal (PMID: 41025371)
- Treatment: R-CHOP chemotherapy; HAART continuation
2. NON-AIDS-DEFINING MALIGNANCIES
Hodgkin Lymphoma (HL)
- Nearly universal cervical lymph node involvement
- More aggressive course in HIV
- Treatment: ABVD + HAART
Squamous Cell Carcinoma (SCC)
- HIV patients have a 3-fold higher age-standardized incidence of HPV-associated and HPV-negative head and neck SCC compared to the general population (Goldman-Cecil Medicine)
- Sites: larynx, oral cavity, oropharynx
- Lip SCC considered a distinct cutaneous risk
- A recent study from New York showed HIV infection in 5% of head and neck cancer patients; in patients under 45, HIV was present in >20%
- More aggressive course compared to immunocompetent patients
Nonmelanoma Skin Cancer (NMSC)
- HIV patients more likely to develop BCC
- Transplant recipients more likely to develop cutaneous SCC
- Both: more aggressive course
H. NEUROLOGICAL MANIFESTATIONS IN HEAD AND NECK
- Facial nerve palsy: Bilateral facial nerve palsies reported; usually represent systemic disease
- Work-up: serology for syphilis, CMV, HSV, HZV, EBV; MRI brain + CSF analysis
- Cranial neuropathies: From skull base osteomyelitis (MOE), CNS lymphoma, cryptococcal meningitis
- Patients with low CD4 count may present with CNS disease with few/ambiguous clinical signs - low threshold for neuroimaging and lumbar puncture
I. HIV TESTING IN OTOLARYNGOLOGY PRACTICE
- Unexplained oral candidiasis
- Hairy leukoplakia of the tongue
- Atypical head and neck cancers
- Parotid cysts
- Cervical lymphadenopathy
- Chronic parotitis
- Pyrexia of unknown origin
- Non-pediatric adenoid hypertrophy
J. TREATMENT - HAART AND IMPACT ON HEAD AND NECK DISEASE
- NRTIs (Nucleoside Reverse Transcriptase Inhibitors): Terminate proviral DNA replication (e.g., zidovudine, tenofovir) - backbone of therapy
- NNRTIs (Non-Nucleoside RTIs): Bind directly to reverse transcriptase active site (e.g., efavirenz, nevirapine)
- Protease Inhibitors (PIs): Block viral particle maturation; complex absorption kinetics (e.g., lopinavir/ritonavir)
- Integrase Inhibitors: Block viral DNA integration (e.g., dolutegravir, raltegravir)
- Entry/Fusion Inhibitors: Reserved for intolerant patients or resistant infection
- Marked decrease in AIDS-defining malignancies (KS, NHL) since HAART introduction
- Resolution of BLECs and parotid disease with immune reconstitution
- However, non-AIDS-defining malignancies (head and neck SCC, lung, liver) continue to rise
- Immune Reconstitution Inflammatory Syndrome (IRIS) - paradoxical worsening of conditions after HAART initiation (e.g., tuberculous lymphadenitis flare)
RECENT ADVANCES (2021-2026)
-
Plasmablastic Lymphoma: Growing recognition of this oral cavity-predominant, HIV-associated aggressive B-cell lymphoma. Xu et al. Head Neck 2025 (PMID 41025371) document rising case series; strongly EBV and HIV co-associated.
-
EBV-HIV co-infection in Head and Neck Lymphomas: Xoki et al., Oral Surg Oral Med 2026 (PMID 40975699) demonstrated the incidence and role of EBV and HIV in head and neck lymphomas, confirming synergistic oncogenic roles.
-
HIV-HPV interaction in Head and Neck SCC: Growing evidence that HIV-infected individuals have 3-fold higher incidence of HPV-associated oropharyngeal SCC. Vaccination against HPV (Gardasil 9) is now recommended for all HIV-positive patients regardless of age.
-
Dolutegravir-based regimens are now first-line globally (WHO 2023 guidelines), offering better tolerability and higher barrier to resistance compared to older HAART regimens, leading to improved head and neck disease control.
-
Pre-Exposure Prophylaxis (PrEP): Tenofovir/emtricitabine daily use has significantly reduced new HIV infections in high-risk populations, with attendant reduction in head and neck HIV manifestations in high-income countries.
-
Oral Microbiome: Recent research shows HIV-positive patients have a dysbiotic oral microbiome independent of antiretroviral use, contributing to periodontal disease severity.
-
Hearing Loss Screening: Updated recommendations for formal audiological screening in all HIV-positive patients given the high prevalence (up to 49%) of subclinical SNHL from combined viral, opportunistic, and drug-related ototoxicity.
SUMMARY TABLE: Head and Neck Manifestations of HIV
| Region | Manifestation | CD4 Threshold | Key Feature |
|---|---|---|---|
| Oral cavity | Pseudomembranous candidiasis | Any stage, worsens <200 | Most common oral manifestation |
| Oral cavity | Hairy leukoplakia | <300 | Lateral tongue, EBV-driven |
| Oral cavity | Kaposi sarcoma | <200 | HHV-8, hard palate |
| Oral cavity | Aphthous ulcers | Any stage | Major form in HIV |
| Periodontal | NUG/NUP | <200 | Rapid bone loss |
| Salivary glands | Benign lymphoepithelial cysts | Any stage | Bilateral parotid cysts |
| Neck | PGL | Early/any stage | Follicular hyperplasia |
| Neck | NHL/HL | Late stage | Extranodal disease |
| Sinuses | Acute/Chronic sinusitis | >200 | Same organisms as normal |
| Sinuses | Invasive fungal sinusitis | <50 | Aspergillus, bony erosion |
| Ear | Malignant OE | Late stage | Pseudomonas/Aspergillus |
| Ear | Serous otitis media | Any stage | Eustachian tube dysfunction |
| Pharynx | Exudative pharyngitis | Seroconversion | Monospot negative |
| Larynx | Candidal laryngitis | <200 | Hoarseness |
REFERENCES (Standard Textbooks for RGUHS)
- Scott-Brown's Otorhinolaryngology Head and Neck Surgery, 8th Edition - Vol 1, Chapter 23: HIV and the ENT Surgeon, pp. 277-282
- Cummings Otolaryngology Head and Neck Surgery, 7th Edition - Chapter 10: Immunodeficiency and ENT, Table 10.3-10.4, pp. 4141-4180
- KJ Lee's Essential Otolaryngology, 11th Edition - Chapter 11: Head and Neck Manifestations of HIV, pp. 233-244
- Dhingra PL, Dhingra S - Diseases of Ear, Nose and Throat and Head and Neck Surgery - Chapter on AIDS and ENT Manifestations
- Hazarika P - Textbook of Ear, Nose and Throat and Head and Neck Surgery - HIV manifestations section
- Zakir Hussain - ENT Short Cases - OSCE preparation chapter on AIDS/HIV
- Stell and Maran's Head and Neck Surgery - Immune-mediated head and neck disease chapter
- Goldman-Cecil Medicine, 27th Edition - Human Immunodeficiency Virus section
- Xu A et al. Oral Plasmablastic Lymphoma: Case Series and Literature Review. Head Neck. 2025 Dec. PMID: 41025371
- Xoki B et al. The incidence and role of EBV and HIV in head and neck lymphomas. Oral Surg Oral Med Oral Pathol Oral Radiol. 2026 Jan. PMID: 40975699