Chronic abdominal conditions
Reading File
Asking for Preferences
Details lecture
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive material from authoritative textbooks. Let me compose the full detailed lecture.
Chronic Abdominal Conditions — Detailed Lecture
1. Definition & Framework
Chronic abdominal pain is defined as pain that has been present constantly or intermittently for at least 6 months. This distinguishes it from:
- Acute pain: days or less
- Subacute pain: days to less than 6 months
The core clinical challenge is distinguishing organic (structural) disease from functional GI disorders (FGIDs). Both can co-exist, and the approach must remain vigilant to avoid missing a treatable structural cause.
- Sleisenger & Fordtran's Gastrointestinal and Liver Disease, Chapter 12
2. Classification of Causes
Structural (Organic) Disorders
| Category | Examples |
|---|---|
| Inflammatory | IBD (Crohn's, UC), celiac disease, diverticular disease, eosinophilic gastroenteritis |
| Neoplastic | Colorectal cancer, gastric cancer, pancreatic cancer |
| Obstructive | Biliary tract disease, chronic mesenteric ischemia |
| Metabolic/Endocrine | Diabetic radiculopathy, Addison's disease, porphyria |
| Vascular | Chronic mesenteric ischemia |
| Musculoskeletal | Nerve entrapment, slipping rib syndrome |
| Gynecologic | Endometriosis, ovarian cysts |
| Pancreatic | Chronic pancreatitis |
| Peptic | Peptic ulcer disease |
Functional Disorders (FGIDs)
- Irritable Bowel Syndrome (IBS)
- Centrally Mediated Abdominal Pain Syndrome (CAPS) - formerly functional abdominal pain syndrome
- Functional dyspepsia
- Narcotic Bowel Syndrome
"Alarm" features that always suggest organic disease:
- Fever, severe pain, significant weight loss
- Jaundice, progressive dysphagia, recurrent vomiting
- Nocturnal pain or diarrhea
- Bloody stools or fecal occult blood positive
- Age >50 years, new onset symptoms
- Abnormal labs: anemia, leukocytosis, elevated CRP, low albumin, low vitamins A/D/B12
- Goldman-Cecil Medicine, Chapter 316
3. Approach to the Patient
History
Key elements:
- Site - visceral pain is diffuse, midline (bilateral innervation); parietal pain is localized
- Onset and chronicity
- Character - colicky, burning, cramping, constant
- Radiation - referred pain shares spinal dermatomes with the visceral source
- Relieving/aggravating factors - relation to meals, defecation, posture, menstrual cycle
- Associated symptoms - weight loss, diarrhea, vomiting, bleeding, fever
Important: Patients with chronic conditions (especially IBS) often show distorted pain patterns compared to healthy subjects, possibly due to spinal sensitization of convergent pathways. This makes anatomical localization less reliable.
Physical Examination
- Vital signs: less likely disturbed in chronic conditions
- Look for jaundice, skin rashes (erythema nodosum, pyoderma gangrenosum in IBD; dermatitis herpetiformis in celiac disease)
- Organomegaly, masses, ascites, hernias
- Signs of malnutrition (sarcopenia, edema)
- "Closed eyes" sign - seen in CAPS/functional pain
- Carnett's test - to detect abdominal wall pain origin:
- Palpate area of maximal tenderness, then ask patient to raise legs (tensing abdominal muscles)
- Positive (worse pain) = abdominal wall source
- Negative (less pain) = intraabdominal process
- Yamada's Textbook of Gastroenterology, 7th ed.
Diagnostic Algorithm
Here is the standard clinical approach:
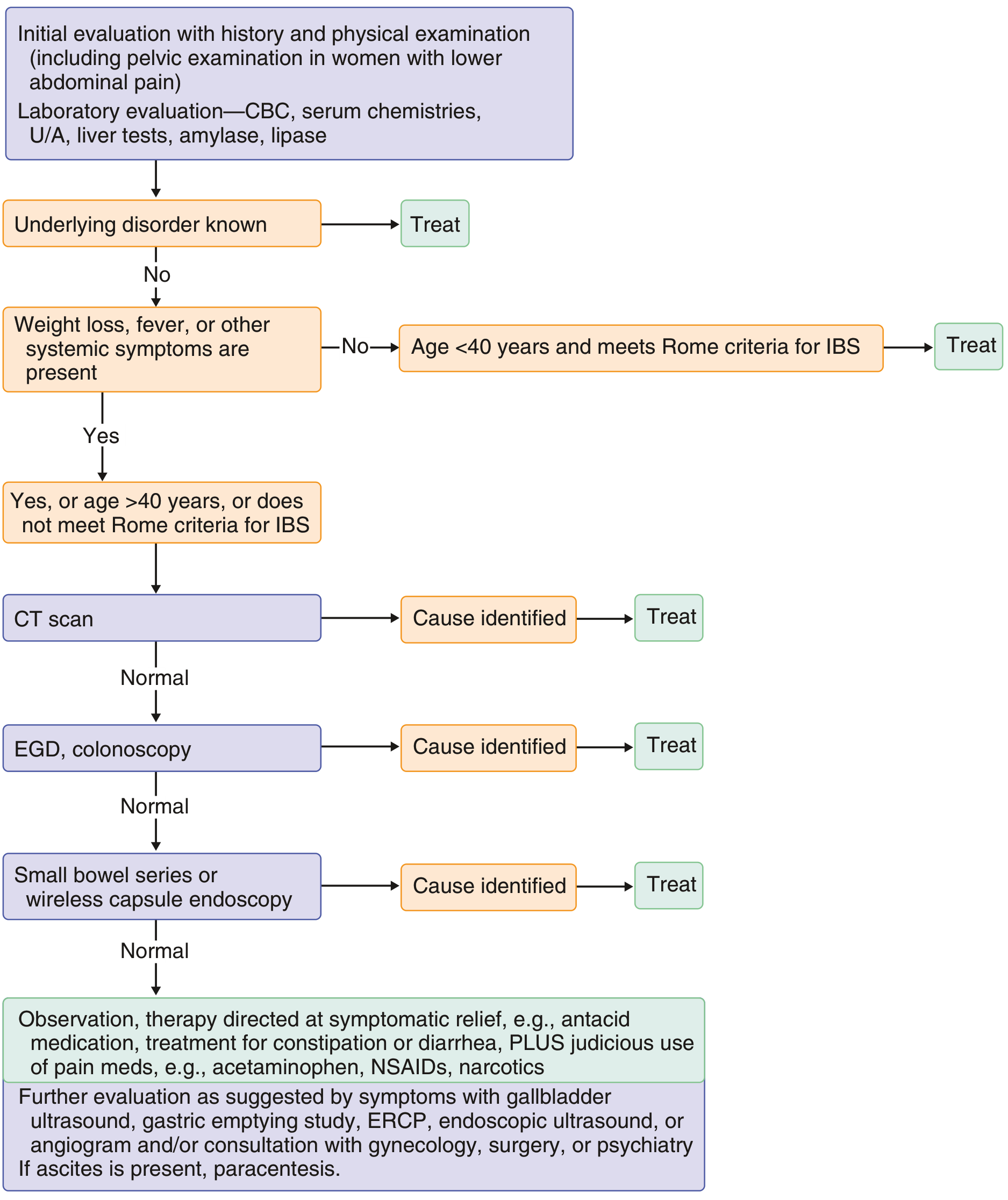
Step-by-step:
- History + physical examination + basic labs (CBC, chemistries, liver tests, amylase/lipase, U/A)
- If underlying disorder known → treat
- If no alarm symptoms + age <40 + meets Rome criteria → treat as IBS
- If alarm features OR age >40 → CT scan
- CT normal → EGD + Colonoscopy
- Still normal → small bowel series or capsule endoscopy
- All normal → symptomatic management (antacids, laxatives, judicious analgesia) + further targeted workup as needed
- Goldman-Cecil Medicine, Figure 316-3
4. Major Chronic Abdominal Conditions
A. Irritable Bowel Syndrome (IBS)
Epidemiology: Most common functional GI disorder. Prevalence 1-20% worldwide (~7% in the USA). Onset typically late 20s; costs >$20 billion/year in the US in direct and indirect expenditures.
Pathophysiology (multi-factorial):
- Genetic predisposition
- Disturbed CNS pain processing (brain-gut axis)
- Visceral hypersensitivity
- Mucosal low-grade inflammation
- Abnormal colonic motility (slower in IBS-C, faster in IBS-D)
- Psychosocial stressors
- Anxiety, somatoform disorders, and history of physical/sexual abuse found in 42-61% of IBS patients referred to gastroenterologists
Rome IV Diagnostic Criteria:
Recurrent abdominal pain ≥1 day/week over the last 3 months, associated with ≥2 of:
- Related to defecation
- Change in stool frequency
- Change in stool form/appearance
Subtypes:
- IBS-C (constipation predominant)
- IBS-D (diarrhea predominant)
- IBS-M (mixed)
- IBS-U (unclassified)
Differential Diagnosis: IBD, lactose intolerance, celiac disease, small intestinal bacterial overgrowth, colorectal cancer, thyroid disorders
Management:
- Dietary: low FODMAP diet, fiber supplementation
- Pharmacological:
- IBS-C: linaclotide, lubiprostone, plecanatide
- IBS-D: loperamide, rifaximin, alosetron (women)
- Antispasmodics: dicyclomine, hyoscine
- Neuromodulators: low-dose tricyclic antidepressants (TCAs), SNRIs
- Psychological: CBT, gut-directed hypnotherapy
- Textbook of Family Medicine, 9th ed.; Sleisenger & Fordtran
B. Inflammatory Bowel Disease (IBD)
Overview: Chronic condition requiring long-term maintenance therapy. Two major subtypes: Ulcerative Colitis (UC) and Crohn's Disease (CD). A third, less common form is microscopic colitis.
Epidemiology:
- Incidence: 1.5-8 new cases per 100,000/year
- More common in whites; no clear gender predominance (slight male predominance in CD, female in UC)
- Age of onset: bimodal - 15-25 years and 55-65 years
- First-degree relatives have ~10% lifetime risk of developing IBD
Pathophysiology:
- Genetic factors (NOD2 mutation in Crohn's)
- Dysregulation of immune response to intestinal microbiota
- Environmental triggers (smoking increases CD risk, protective in UC)
Ulcerative Colitis:
- Involves mucosal layer only
- Starts at rectum, spreads proximally in a continuous, symmetric pattern
- Pancolitis with backwash ileitis in severe cases
- Clinical: diarrhea (often bloody), tenesmus, urgency; constitutional symptoms in severe disease
Crohn's Disease:
- Involves entire bowel wall (transmural)
- Any part of GI tract (mouth to anus)
- Most common: terminal ileum
- Discontinuous ("skip lesions"), asymmetric
- Cobblestoning, strictures, fistulas, perianal disease
- Rectum involved in <50%
Extraintestinal Manifestations (both UC and CD):
- Eyes: uveitis, iritis, episcleritis
- Joints: large joint arthropathy, sacroiliitis
- Skin: erythema nodosum, pyoderma gangrenosum
- Liver: primary sclerosing cholangitis (especially UC)
Treatment:
- Steroids: effective for inducing remission - NOT for maintenance
- 5-ASA agents (mesalamine, sulfasalazine): effective in UC for induction and maintenance; largely ineffective in Crohn's disease
- Immunomodulators: azathioprine, 6-mercaptopurine, methotrexate
- Biologics: anti-TNF (infliximab, adalimumab), anti-integrin (vedolizumab), anti-IL-12/23 (ustekinumab)
- Surgery: colectomy may be curative in UC; Crohn's surgery is palliative and reserved for complications
- Textbook of Family Medicine, 9th ed.
C. Peptic Ulcer Disease (PUD)
Epidemiology: Common; affects >4 million Americans per year. Lifetime risk ~10% in males, ~4% in females.
Etiology (causes mucosal defense-offense imbalance):
- H. pylori infection - present in >70% of PUD cases; only 5-10% of infected individuals develop ulcers
- NSAID/aspirin use - increasingly the most common cause of gastric ulcers as H. pylori rates fall
- Zollinger-Ellison syndrome - gastrin-secreting tumor causing massive acid production, multiple ulcers in stomach/duodenum/jejunum
- Other cofactors: smoking (reduces mucosal blood flow), corticosteroids, alcohol-related cirrhosis, COPD, chronic renal failure, hyperparathyroidism (hypercalcemia stimulates gastrin)
Locations:
- Gastric antrum
- First portion of duodenum (most common)
- Esophagus (in GERD / ectopic gastric mucosa)
Pathogenesis:
- Hyperacidity (H. pylori → parietal cell hyperplasia; Zollinger-Ellison → constitutive gastrin)
- Reduced mucosal defense (prostaglandin depletion by NSAIDs)
Clinical features:
- Epigastric burning/gnawing pain
- Gastric ulcer: pain worsens with meals
- Duodenal ulcer: pain relieved by meals, worse 2-3 hours after eating, nocturnal pain
- Complications: bleeding, perforation, gastric outlet obstruction, malignant transformation (gastric ulcers)
Management:
- Test and treat H. pylori (urea breath test, stool antigen, or biopsy-based tests)
- Proton pump inhibitors (PPIs) as mainstay
- H2 receptor antagonists
- Triple therapy for H. pylori: PPI + clarithromycin + amoxicillin (or metronidazole)
- Avoid NSAIDs; use PPIs prophylactically if NSAIDs essential
- Robbins & Kumar Basic Pathology; Costanzo Physiology 7th ed.
D. Chronic Pancreatitis
Definition: Permanent pathological damage to the pancreas, characterized by progressive fibrosis and inflammation.
Etiology:
- Chronic alcohol abuse (most common in adults)
- Idiopathic (second most common)
- Hereditary (PRSS1, CFTR, SPINK1 gene mutations)
- Autoimmune pancreatitis
- Recurrent acute pancreatitis
Pathology:
- Pancreatic calcifications visible on plain X-ray and CT
- Ductal strictures and dilatation ("chain of lakes" on MRCP/ERCP)
- Fibrosis replacing acinar tissue
Clinical Features:
- Chronic epigastric pain radiating to back; worse after meals/alcohol
- Exocrine insufficiency: steatorrhea, malabsorption, weight loss
- Endocrine insufficiency: diabetes mellitus (pancreatogenic)
- Complications:
- Pseudocyst formation
- Abscess
- Fistula (pseudocyst to gut, peritoneal cavity)
- Mesenteric venous thrombosis
- Arterial pseudoaneurysm
- Pancreatic ascites (disrupted ductal system)
- Increased risk of pancreatic cancer
Management:
- Abstinence from alcohol (slows progression)
- Pain: analgesics (non-opioid first), neuromodulators, ERCP for ductal decompression, surgery (Whipple/Frey procedure) in selected patients
- Exocrine insufficiency: pancreatic enzyme replacement with each meal
- Endocrine insufficiency: insulin therapy
- Nutritional support, fat-soluble vitamin supplementation
- Textbook of Family Medicine, 9th ed.; Sleisenger & Fordtran
E. Centrally Mediated Abdominal Pain Syndrome (CAPS)
Formerly called: Functional abdominal pain syndrome
Pathophysiology:
- Central sensitization of pain pathways
- Loss of descending inhibitory pain modulation
- High comorbidity with anxiety, depression, PTSD, history of abuse
Diagnosis: Rome IV criteria - abdominal pain present >6 months:
- Continuous or nearly continuous pain
- No/only occasional relation to gut function
- Some loss of daily functioning
- Pain is not feigned
Key feature: "Closed eyes" sign during examination (patients close eyes during palpation, suggesting a central/psychogenic component)
Treatment:
- Multidisciplinary team: gastroenterologist, pain specialist, psychiatrist/psychologist, nutritionist
- Neuromodulators (preferred term to avoid stigma):
- Low-dose TCAs (amitriptyline) - affect afferent pain signaling
- SNRIs (duloxetine, venlafaxine)
- Low-dose SSRIs
- Gabapentin/pregabalin (for neuropathic component)
- Cognitive behavioral therapy (CBT)
- Biofeedback, mindfulness
- Avoid opioids - risk of narcotic bowel syndrome
F. Narcotic Bowel Syndrome (NBS)
A paradoxical condition where opioid use worsens abdominal pain over time.
Rome IV Criteria (must fulfill all for >3 months, onset ≥6 months prior):
- Chronic or frequently recurring abdominal pain treated with high-dose/chronic narcotics
- Pain NOT explained by a current/previous GI diagnosis
- Plus ≥2 of:
- Pain worsens or incompletely resolves with continued/escalating opioids
- Marked worsening when dose wanes, improvement when reinstated ("soar and crash")
- Progressive increase in frequency, duration, and intensity of pain episodes
Management: Gradual opioid taper (inpatient detoxification often needed), neuromodulators, psychological support
- Yamada's Textbook of Gastroenterology, 7th ed.
5. Abdominal Wall Pain
Often misdiagnosed as visceral pain. Causes include:
| Cause | Notes |
|---|---|
| Anterior cutaneous nerve entrapment (ACNES) | Along lateral edge of rectus sheath; positive Carnett's |
| Slipping rib syndrome | Lower rib hypermobility |
| Myofascial pain syndrome | Trigger points in abdominal musculature |
| Thoracic nerve radiculopathy | T6-T12 dermatomal distribution |
| Endometriosis | Cyclic pain, laparoscopy for diagnosis |
| Hernia | CT/ultrasound |
| Diabetic radiculopathy | Acute truncal pain T6-T12 |
Diagnosis of abdominal wall pain: Carnett's test positive; response to local anesthetic infiltration confirms the diagnosis and may also be therapeutic.
6. Management Principles for Chronic Abdominal Pain
General Strategy
- Make a confident working diagnosis
- Treat the underlying cause when possible
- Multidisciplinary approach for functional/refractory cases
- Progress from least invasive to more invasive interventions
Pharmacological Options
| Drug Class | Examples | Use |
|---|---|---|
| Antispasmodics | Hyoscine, dicyclomine | IBS, biliary spasm |
| Neuromodulators (TCAs) | Amitriptyline, nortriptyline | CAPS, IBS, neuropathic pain |
| SNRIs | Duloxetine, venlafaxine | CAPS, IBS |
| Gabapentinoids | Gabapentin, pregabalin | Neuropathic/centrally sensitized pain |
| Antidepressants (SSRIs) | Fluoxetine, paroxetine | Comorbid anxiety/depression |
| Opioids | Tramadol, opiates | Last resort only; risk of NBS |
Non-Pharmacological
- CBT - strongest evidence for functional GI disorders
- Gut-directed hypnotherapy
- Biofeedback
- Exercise programs
- Dietary modification (low FODMAP, gluten-free for celiac)
Interventional
- Celiac plexus block (chronic pancreatitis, cancer pain)
- ERCP (biliary/pancreatic ductal decompression)
- Trigger point injections (abdominal wall pain)
- Nerve ablation techniques
7. Key Differentiating Points: Organic vs Functional
| Feature | Organic | Functional |
|---|---|---|
| Age at onset | Any age; new onset >50 warrants workup | Usually <40 years |
| Nocturnal awakening | Common | Uncommon |
| Weight loss | Present | Absent |
| Bloody stools | Possible | Absent |
| Fever | May be present | Absent |
| Lab abnormalities | Common | Normal |
| Response to food | Variable and specific | Often non-specific |
| Psychological comorbidity | Less prominent | Often prominent |
Summary
Chronic abdominal conditions form a broad spectrum from structural diseases (IBD, PUD, chronic pancreatitis, cancer) to centrally mediated functional disorders (IBS, CAPS). The key to management is:
- Systematic evaluation to exclude organic disease before labeling functional
- Recognize alarm features that mandate urgent investigation
- Disease-specific therapy for structural conditions
- Multidisciplinary biopsychosocial approach for functional conditions
- Avoid over-reliance on opioids - risk of NBS and worsening outcomes
Sources:
- Sleisenger & Fordtran's Gastrointestinal and Liver Disease, Chapter 12 (Chronic Abdominal Pain)
- Goldman-Cecil Medicine, Chapter 316 (Chronic Abdominal Pain)
- Yamada's Textbook of Gastroenterology, 7th ed., Chapter 34
- Textbook of Family Medicine, 9th ed., Chapter 38
- Robbins & Kumar Basic Pathology (Peptic Ulcer Disease)
This is a shared conversation. Sign in to Orris to start your own chat.