ICP & IOP
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
I now have comprehensive textbook content on both ICP and IOP. Let me compile the full answer.
Intracranial Pressure (ICP) & Intraocular Pressure (IOP)
INTRACRANIAL PRESSURE (ICP)
Physiology & Normal Values
The cranial vault is a rigid bony structure containing three compartments:
- Brain - 80%
- Blood - 12%
- CSF - 8%
Normal ICP is ≤10 mmHg (supratentorial, measured in lateral ventricles or over cerebral cortex). In the lateral recumbent position, lumbar CSF pressure normally approximates supratentorial pressure.
Monro-Kellie Doctrine
Since total intracranial volume is fixed, any increase in one compartment must be offset by a decrease in another - otherwise ICP rises. The major compensatory mechanisms are:
- Displacement of CSF from cranial to spinal compartment
- Increased CSF absorption
- Decreased CSF production
- Decreased cerebral blood volume (primarily venous)
The compliance curve is initially flat (good compensation), but once reserves are exhausted, even small volume additions cause precipitous ICP rises - the curve becomes exponential:
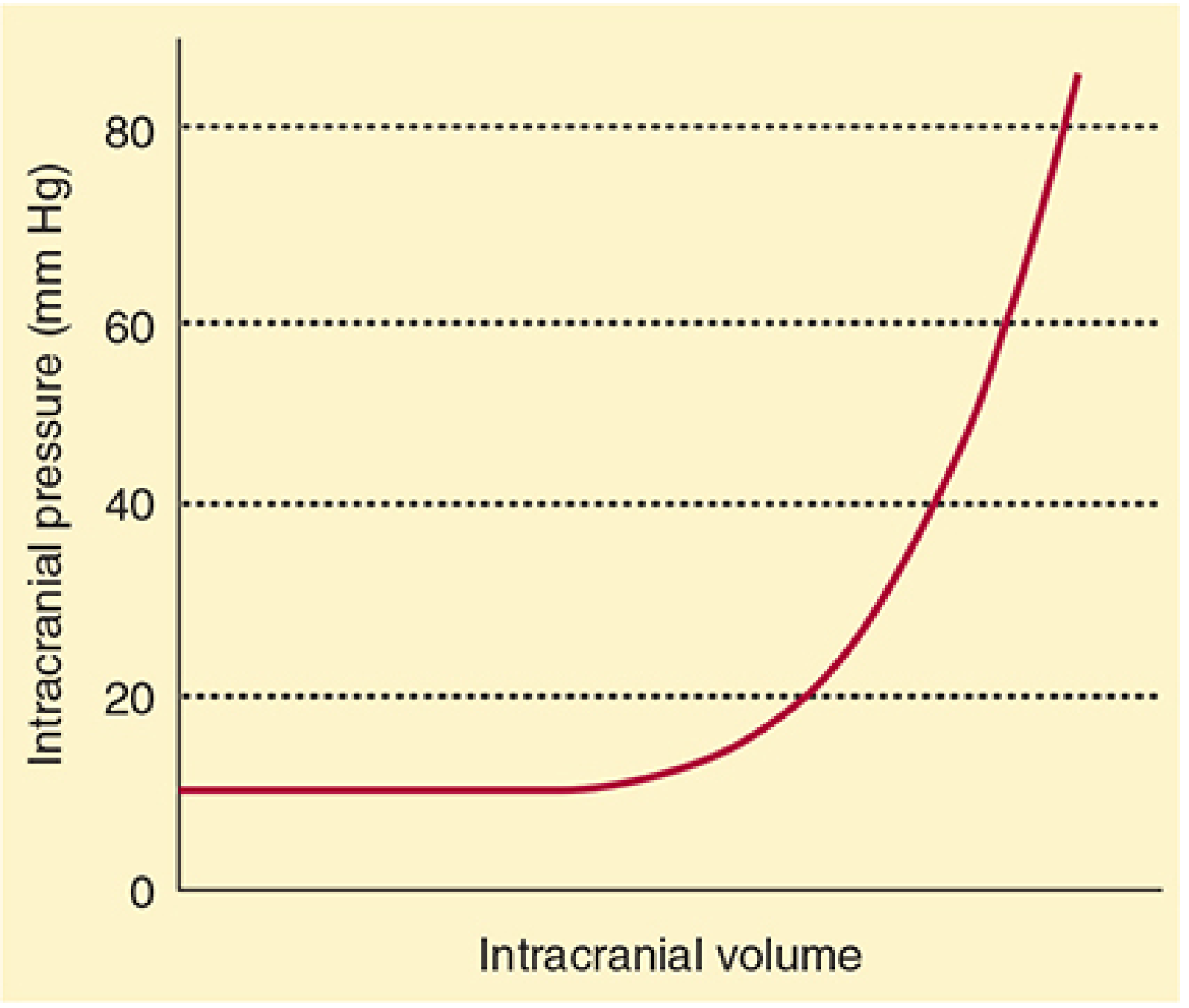
Figure: Normal intracranial elastance curve. The flat portion reflects compensation; beyond the "elbow," pressure rises steeply with any further volume increase. - Morgan and Mikhail's Clinical Anesthesiology, 7e
Cerebral Perfusion Pressure (CPP)
CPP = MAP - ICP
Adequate CPP must be maintained to support brain perfusion. ICP monitoring targets maintaining CPP, not just controlling ICP in isolation.
ICP Monitoring - Indications
ICP monitoring is indicated in:
- Severe TBI (GCS ≤8 with abnormal CT scan)
- Severe TBI with normal CT + ≥2 of: age >40, unilateral/bilateral motor posturing, SBP <90 mmHg
- Acute subarachnoid hemorrhage with coma or neurologic deterioration
- Intracranial hemorrhage with intraventricular blood
- Ischemic MCA stroke
- Fulminant hepatic failure with coma and cerebral edema
- Global cerebral ischemia/anoxia with cerebral edema on CT
Target: ICP <20 mmHg is the standard therapeutic threshold - ICP >20 mmHg is associated with unfavorable outcomes in TBI.
(- Schwartz's Principles of Surgery, 11th Ed)
ICP Monitoring Devices
| Device | Location | Notes |
|---|---|---|
| Ventriculostomy catheter (gold standard) | Lateral ventricle | Measures ICP + allows CSF drainage + CSF sampling |
| Fiberoptic monitor | Parenchymal/subdural | Measurement only |
| Other transducers | Subdural/epidural | Measurement only |
Ventriculostomy complications: infection (5%), hemorrhage (1.1%), malfunction (6.3-10.5%), malposition.
Clinical Features of Raised ICP
Symptoms: headache, nausea/vomiting, drowsiness, ocular palsies, papilledema
- At ICP 25-40 mmHg: patients generally remain mentally alert unless brainstem compressed
- At ICP 40-50 mmHg (acute): cerebral blood flow diminishes - loss of consciousness
- Above this: global ischemia and brain death
- Herniation with ipsilateral pupil dilation typically occurs at ICP 28-34 mmHg
In infants (unfused sutures): head enlarges, eyes protrude (cannot compensate with herniation, compensates with skull expansion instead).
(- Adams and Victor's Principles of Neurology, 12th Ed)
Brain Herniation Syndromes (4 sites)
- Cingulate gyrus under the falx cerebri (subfalcine)
- Uncinate gyrus through the tentorium cerebelli (uncal/transtentorial)
- Cerebellar tonsils through the foramen magnum (tonsillar)
- Transcalvarial - through a skull defect
Management of Elevated ICP
All measures should be administered simultaneously, not sequentially:
| Intervention | Detail |
|---|---|
| Head position | HOB 30°, head neutral (optimize jugular venous drainage) |
| Hyperventilation | Temporizing only - PCO2 25-35 mmHg; never <25 mmHg |
| MAP support | Maintain MAP ≥80 mmHg; use isotonic fluids ± inotropes |
| Mannitol | 0.5-1 g/kg IV over 15 min; replace diuresis with NS |
| Hypertonic saline | Alternative to mannitol; caution in chronic hyponatremia, cardiac instability |
| Sedation/analgesia | Propofol 0.1-5 mg/kg/hr or benzodiazepines; fentanyl 20-200 mcg/hr |
| Barbiturates | Pentobarbital 20 mg/kg load then 1-3 mg/kg/hr (target burst suppression 4-6 bursts/min) |
| CSF drainage | External ventricular drain - can be life-saving |
| Surgical evacuation | Hematoma/mass lesion removal; decompressive craniectomy |
| Steroids | No role in traumatic brain injury |
| Seizure control | Prevent ICP spikes |
Monitor serum Na+ and osmolality in patients on mannitol or hypertonic saline.
(- Plum and Posner's Diagnosis and Treatment of Stupor and Coma; Schwartz's Surgery 11e)
INTRAOCULAR PRESSURE (IOP)
Physiology & Normal Values
| Parameter | Value |
|---|---|
| Normal IOP | 10-21.7 mmHg (average ~15 mmHg) |
| Abnormal threshold | >22 mmHg |
| Diurnal variation | 2-5 mmHg (higher in morning on waking) |
| Cardiac cycle variation | 1-2 mmHg per heartbeat |
(- Barash Clinical Anesthesia 9e; Guyton & Hall Medical Physiology)
Aqueous Humor Dynamics - the Regulator of IOP
Production: Ciliary body (non-pigmented ciliary epithelium) continuously secretes aqueous humor into the posterior chamber at ~2.5 μL/min.
Flow path: Posterior chamber → pupil → anterior chamber → trabecular meshwork (iridocorneal angle) → Canal of Schlemm → aqueous veins → blood veins → episcleral veins
IOP regulation depends on the balance between:
- Rate of aqueous production
- Rate of aqueous outflow (trabecular resistance + episcleral venous pressure)
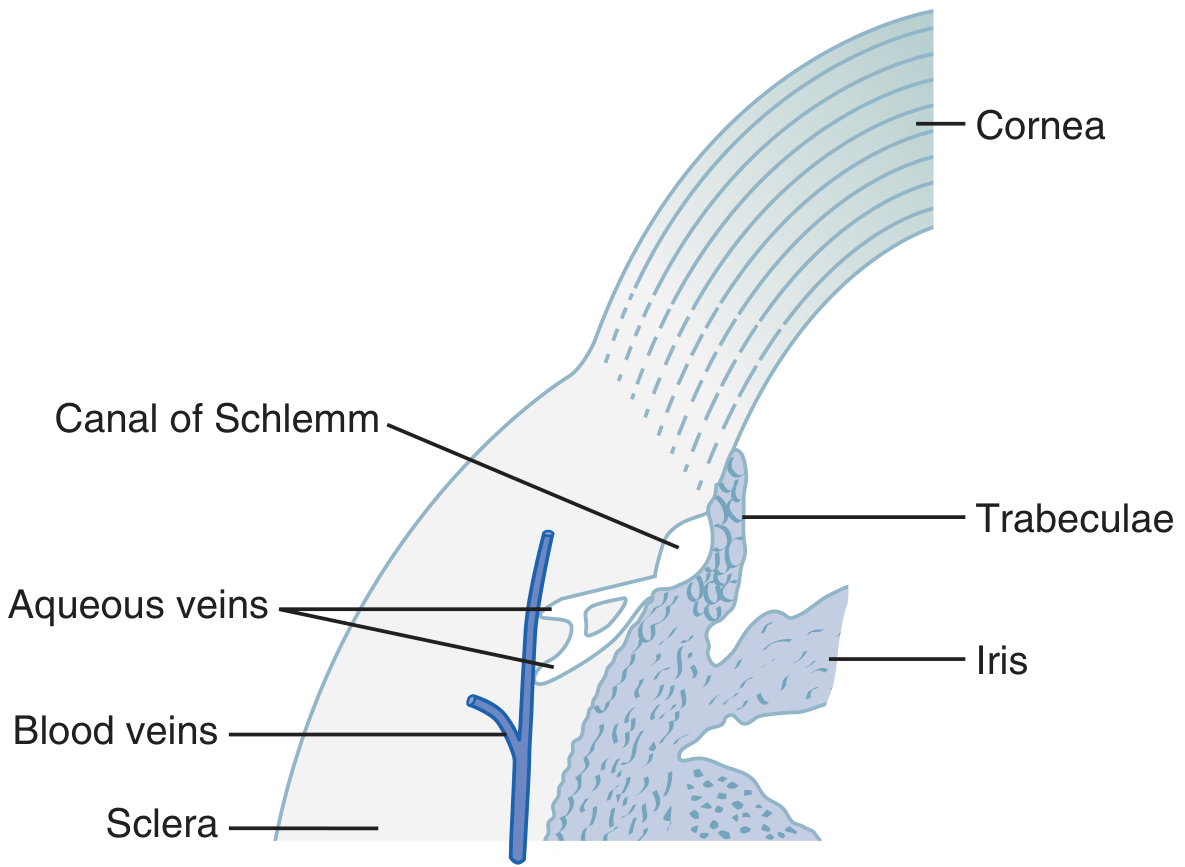
Figure: Iridocorneal angle anatomy showing trabecular meshwork and Canal of Schlemm - the aqueous outflow route. - Guyton & Hall Medical Physiology
The trabecular spaces have openings of only 2-3 micrometers. Fluid flow into the canal increases as pressure rises (pressure-dependent outflow).
Outflow routes (Kanski's Ophthalmology):
- (A) Trabecular - primary route
- (B) Uveoscleral
- (C) Iris
Factors Influencing IOP
Three main categories (Barash Clinical Anesthesia 9e):
-
External pressure on the eye
- Orbicularis oculi contraction
- Extraocular muscle tone
- Venous congestion of orbital veins (vomiting, coughing)
- Orbital tumor
- Neck constriction (tight collar, Trendelenburg position)
-
Scleral rigidity - elderly patients with scleral sclerosis have decreased compliance and increased IOP
-
Intraocular contents
- Aqueous humor (most important)
- Blood volume (choroidal blood volume)
- Vitreous hydration
- Lens changes (size/position)
Venous pressure is particularly critical - straining, vomiting, or coughing can raise IOP by 40 mmHg or more. Laryngoscopy and intubation also elevate IOP even without a visible hemodynamic response.
IOP Measurement
Tonometry - the cornea is anesthetized, the tonometer footplate placed on the cornea, and a small plunger force applied. The displacement is calibrated to IOP values.
Applanation tonometry - gold standard; upper limit of normal is 21 mmHg.
Diurnal variation means the time of day must always be noted alongside IOP readings.
Glaucoma - IOP Dysregulation
Glaucoma = optic neuropathy from impaired aqueous outflow → elevated IOP → optic nerve damage → visual field loss (initially peripheral)
| Type | Mechanism | Notes |
|---|---|---|
| Primary open-angle (POAG) | Trabecular sclerosis → outflow resistance, open anterior angle | Most common type; often asymptomatic until advanced |
| Secondary open-angle | Particulate matter (RBCs, tumor debris) clogging trabecular meshwork | After trauma or necrotic tumor |
| Primary angle-closure | Peripheral iris contacts posterior cornea - mechanical obstruction | Predisposed: hyperopia (shallow anterior chamber) |
| Acute angle-closure | Rapid block; mydriasis worsens it | Urgent - painful eye, hard globe, fixed mid-dilated pupil |
| Secondary angle-closure | Neovascular (VEGF in chronic retinal ischemia), pupillary block from lens swelling | - |
Pathological hallmark: diffuse loss of ganglion cells, thinning of retinal nerve fiber layer, cupped and atrophic optic nerve.
(- Robbins Basic Pathology; Kanski's Clinical Ophthalmology 10e)
Anesthetic/Clinical Considerations for IOP
Agents that raise IOP: succinylcholine (transient), laryngoscopy/intubation, coughing, vomiting, Trendelenburg position, hypercapnia (choroidal congestion), overhydration
Agents that lower IOP: most IV anesthetics (propofol, thiopental), volatile agents, opioids, β-blockers (timolol - reduces aqueous production)
Perioperative concerns:
- A rise in IOP during anesthesia can cause permanent visual loss
- In open-globe surgery: excessive IOP can cause iris/lens prolapse and vitreous loss
- Atropine in standard clinical doses is safe in glaucoma; scopolamine has greater mydriatic effect - avoid in angle-closure glaucoma
- Robotic laparoscopic procedures (Trendelenburg + pneumoperitoneum) can significantly raise IOP
(- Barash Clinical Anesthesia 9e; Miller's Anesthesia 10e)
ICP vs. IOP - Key Comparisons
| Feature | ICP | IOP |
|---|---|---|
| Normal value | ≤10 mmHg | 10-21.7 mmHg (avg ~15) |
| Abnormal threshold | >20 mmHg (TBI target) | >22 mmHg |
| Fluid governing pressure | CSF | Aqueous humor |
| Production site | Choroid plexus | Ciliary body |
| Drainage route | Arachnoid villi/granulations | Canal of Schlemm → episcleral veins |
| Rigidity of container | Rigid skull (adults) | Relatively rigid globe |
| Compliance mechanism | CSF displacement to spine + venous shift | Trabecular resistance modulation |
| Key consequence of elevation | Herniation, brain ischemia | Optic nerve atrophy (glaucoma) |
| Emergency threshold | >40-50 mmHg = imminent death | Acute angle-closure = ophthalmic emergency |
| Connection | Raised ICP can cause papilledema via optic nerve sheath compression; ICP and IOP share venous pressure dependence | Raised IOP does NOT directly raise ICP |
Sources: Morgan and Mikhail's Clinical Anesthesiology 7e | Guyton and Hall Medical Physiology | Kanski's Clinical Ophthalmology 10e | Barash Clinical Anesthesia 9e | Schwartz's Principles of Surgery 11e | Adams and Victor's Principles of Neurology 12e | Robbins Basic Pathology | Plum and Posner's Diagnosis and Treatment of Stupor and Coma | Miller's Anesthesia 10e
This is a shared conversation. Sign in to Orris to start your own chat.