
100693.jpg
Female 2w old complained about this with itching for 2 weeks
analyse_media
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed to give a complete clinical answer.
Clinical Assessment
Most likely diagnosis: Prurigo Nodularis
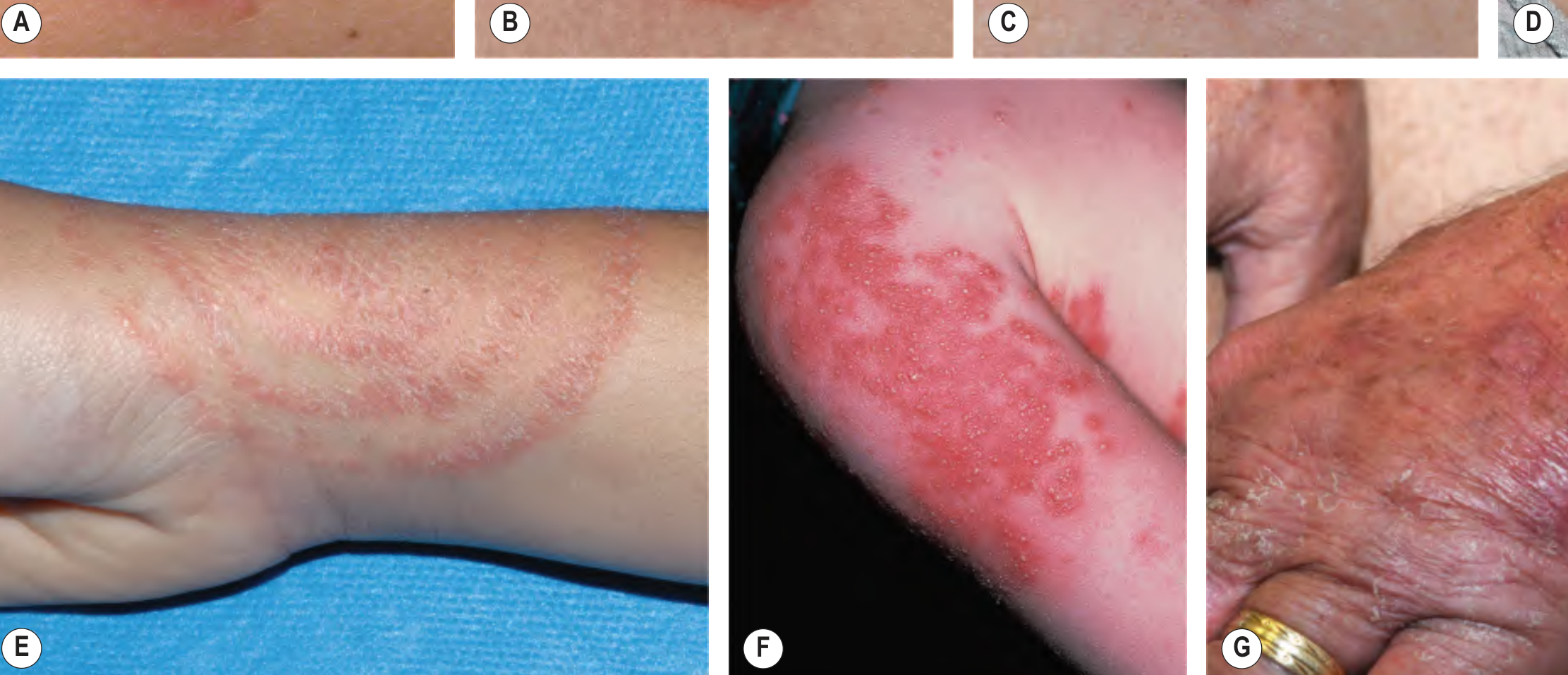
The image shows discrete, firm, hyperpigmented nodules (5 mm to ~2 cm) scattered along the extensor surface of the forearm with excoriation marks - a classic presentation of prurigo nodularis (PN).
Here is a textbook reference image for comparison:

Key Diagnostic Features in This Case
| Feature | Finding |
|---|---|
| Morphology | Firm, dome-shaped hyperpigmented nodules |
| Distribution | Extensor forearm (classic) |
| Size | 5 mm to 2 cm (pea-sized to larger) |
| Surface | Excoriated/crusted centers - evidence of scratching |
| Arrangement | Scattered; some linear (Koebner-like) |
| Duration | 2 weeks of severe itch |
| Patient | Female (PN more common in women) |
Pathophysiology
PN results from repetitive scratching driving an itch-scratch cycle. Neuronal sensitization occurs with increased dermal nerve fiber density, upregulation of substance P, CGRP, NGF receptors, and pro-inflammatory IL-31. The lesions themselves become the source of ongoing itch, perpetuating the cycle. - Dermatology 2-Volume Set, 5e
Differential Diagnosis to Consider
- Nodular scabies - also intensely pruritic red-brown nodules, but typically in axillary/groin/genital areas; look for burrows and household contacts
- Hypertrophic lichen planus - violaceous, Wickham's striae, often oral lesions
- Pemphigoid nodularis - bullous pemphigoid variant; needs biopsy + immunofluorescence
- Persistent insect bite reactions - similar morphology but usually fewer in number and resolves faster
- Multiple keratoacanthomas - crateriform with keratin plug
Evaluation: Given only 2 weeks' duration, also screen for underlying causes: atopic dermatitis, hepatic/renal dysfunction, HIV, lymphoma, or emotional distress.
Workup
- Skin biopsy (punch): compact hyperkeratosis, irregular acanthosis, perivascular mononuclear infiltrate, dermal fibrosis
- Skin scraping to rule out scabies
- CBC, LFTs, RFTs, HIV - screen for systemic triggers
- IgE level - if atopic background suspected
Treatment (Stepwise)
First line:
- Superpotent topical corticosteroids (e.g. clobetasol) under occlusion
- Intralesional triamcinolone for individual persistent nodules
- Emollients + avoidance of soap to reduce xerosis-triggered itch
- Sedating antihistamine at bedtime (e.g. hydroxyzine or chlorphenamine)
- Topical antipruritic agents: menthol lotion, capsaicin 0.025-0.1% (4-6x/day)
Second line:
- Narrowband UVB or PUVA phototherapy
- Dupilumab (FDA-approved for PN; ~45-50% achieved clear/almost clear skin at 24 weeks in RCTs) - Dermatology 2-Volume Set, 5e
- Nemolizumab (IL-31 receptor inhibitor; proven in RCTs)
- Gabapentinoids (gabapentin, pregabalin)
- Naltrexone (μ-opioid receptor antagonist)
Third line (refractory):
- Cyclosporine, methotrexate
- Thalidomide 50-200 mg/day (highly effective but limited by teratogenicity and neuropathy risk)
- SSRIs or tricyclic antidepressants if psychological component
Important Note
Since this is a 2-week-old female with an acute-to-subacute onset, consider nodular scabies seriously in the differential - it can mimic PN exactly and should be excluded before long-term PN treatment is initiated. A skin scraping and examination of close contacts is warranted.
- Andrews' Diseases of the Skin, Clinical Dermatology
- Dermatology 2-Volume Set, 5e (Bolognia et al.)


99461.jpg
99460.jpg
28 y old guy came with this clinical presentation with itching this condition is present all over lower body since a month
analyse_media
analyse_media
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I have sufficient information. One additional important note: given the widespread lower body distribution in a 28-year-old male and the possibility of T. indotineae (terbinafine-resistant strain increasingly prevalent in South Asia), this is worth flagging.
Clinical Assessment
Most likely diagnosis: Widespread Tinea Corporis + Tinea Cruris (Dermatophytosis)
Searching sources... The images show:
- Image 1 (leg/ankle): Confluent hyperpigmented lichenified plaques with raised scaly margins around the ankle/lower leg - classic chronic tinea
- Image 2 (ankle close-up): Clear annular lesions with raised, scaly, active advancing borders and central relative clearing, with polycyclic/serpiginous patterns where multiple rings have merged - pathognomonic for dermatophytosis
Morphological Clues Confirming Diagnosis
| Feature | Finding |
|---|---|
| Lesion type | Annular/polycyclic plaques with raised scaly active border |
| Central clearing | Present - "ringworm" pattern |
| Color | Hyperpigmented (darkly pigmented skin type) with violaceous/erythematous active margins |
| Lichenification | Present - chronic rubbing/scratching |
| Distribution | Widespread lower body - legs, ankle region; extends to lower extremities |
| Duration | 1 month |
| Patient | 28-year-old male (tinea cruris more common in men) |
| Symptom | Intense pruritus |
Pathophysiology
Dermatophytes invade the stratum corneum and spread centrifugally from the point of skin invasion. The advancing border is the active fungal front; the center clears as the immune response suppresses fungal growth there. In T. rubrum infections (most common cause), chronic anthropophilic infection produces persistent leathery, lichenified lesions. Hair follicles act as reservoirs, making treatment more difficult in hairy skin. - Dermatology 2-Volume Set, 5e
⚠️ Important Clinical Alert: T. indotineae (Terbinafine-Resistant Tinea)
Given the widespread distribution involving the entire lower body in a young male from South/Southeast Asia, consider Trichophyton indotineae - a recently emerging terbinafine-resistant dermatophyte causing large, widespread annular lesions. Standard topical terbinafine or short courses will fail.
T. indotineae features per Dermatology 5e:
- Suede-like white front, yellow-brown reverse on culture
- Causes large, widespread, treatment-resistant tinea corporis
- Terbinafine resistance is a key characteristic
Differential Diagnosis
| Condition | How to Distinguish |
|---|---|
| Nummular eczema | No active raised border; KOH negative; responds to topical steroids |
| Erythema annulare centrifugum | Trailing scale (inner edge); no KOH positivity |
| Subacute lupus erythematosus | Photodistributed; ANA/anti-Ro positive |
| Granuloma annulare | Non-scaly; not pruritic; no KOH positivity |
| Psoriasis | Silvery micaceous scale; nail changes; no annular clearing |
| Stasis dermatitis | Varicosities; edema; medial ankle distribution |
Investigations
- KOH preparation (skin scraping from active border) - shows branching septate hyphae - first-line, rapid test
- Fungal culture on Sabouraud dextrose agar - identifies species (critical if treatment-resistant)
- Wood's lamp - limited use (T. rubrum does not fluoresce, unlike Microsporum species)
- Consider: PCR-based species identification if clinically extensive/resistant (to detect T. indotineae)
- Rule out: tinea pedis and onychomycosis (common co-existing sources, especially in young men)
- Rule out: tinea cruris - examine groin/inner thighs, scrotum (scrotum spared in tinea cruris)
Treatment
For localized tinea corporis:
- Topical antifungals: terbinafine 1% cream, clotrimazole, miconazole, oxiconazole BID for 2-4 weeks
- Terbinafine can be used once daily; 1-week course may suffice for limited disease
- Avoid combination steroid-antifungal products (e.g. clotrimazole/betamethasone) - cause widespread tinea and fungal folliculitis
For this patient (extensive, widespread lower body involvement):
- Oral antifungals are required given the extent of disease
- Terbinafine 250 mg/day for 2-4 weeks (first choice for Trichophyton species)
- Itraconazole 200 mg/day for 2-4 weeks (effective for both Trichophyton and Microsporum; preferred if T. indotineae suspected)
- Fluconazole 150-300 mg weekly is an alternative
- Griseofulvin is better for Microsporum species
If T. indotineae resistant strain is confirmed:
- Itraconazole (200 mg/day) is the drug of choice
- Avoid terbinafine monotherapy
Preventive measures:
-
Wear loose-fitting clothing; dry skin thoroughly after bathing
-
Treat concomitant tinea pedis/onychomycosis (reinfection source)
-
Launder contaminated clothing and bedding
-
Avoid sharing towels
-
Andrews' Diseases of the Skin, Clinical Dermatology
-
Dermatology 2-Volume Set, 5e (Bolognia et al.)
This is a shared conversation. Sign in to Orris to start your own chat.