Explain me 10heart disease with ecg changes of those disease
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Searching Images
ECG heart disease ST elevation myocardial infarction STEMI
Searching Images
atrial fibrillation ECG no P waves irregular rhythm
Searching Images
heart block AV block ECG PR interval prolonged
Searching Images
pericarditis ECG saddle shape ST elevation diffuse
Searching Images
pulmonary embolism ECG S1Q3T3 right bundle branch block
Searching Images
Wolff-Parkinson-White syndrome ECG delta wave short PR
Searching Images
hypertrophic cardiomyopathy ECG left ventricular hypertrophy voltage criteria
Searching Images
ventricular tachycardia ECG wide complex tachycardia
Searching Images
complete heart block third degree AV dissociation ECG
I now have comprehensive ECG images and textbook data for all 10 conditions. Let me compile the complete answer.
10 Heart Diseases with ECG Changes
1. ST-Elevation Myocardial Infarction (STEMI)
Pathophysiology: Complete occlusion of a coronary artery causes transmural ischemia and necrosis.
ECG Changes:
- ST elevation ≥1 mm in ≥2 contiguous leads (convex/"tombstone" morphology in large STEMIs)
- Hyperacute T-waves in early phase (tall, peaked, before ST elevation)
- Reciprocal ST depression in opposite leads
- Pathological Q waves (>40 ms wide, >25% of R-wave height) appear within hours — indicate necrosis
- T-wave inversion in evolutionary phase
Localisation:
| Territory | Leads with ST elevation | Artery |
|---|---|---|
| Anterior | V1–V4 | LAD (proximal) |
| Inferior | II, III, aVF | RCA or LCx |
| Lateral | I, aVL, V5–V6 | LCx |
| Posterior | Tall R in V1–V2, ST depression V1–V3 | RCA/LCx |
Source: Tintinalli's Emergency Medicine & Rosen's Emergency Medicine
2. Non-ST-Elevation MI / Unstable Angina (NSTEMI/UA)
Pathophysiology: Partial coronary occlusion or severe subendocardial ischemia without transmural injury.
ECG Changes:
- ST depression ≥0.5 mm (horizontal or downsloping) — most diagnostic
- T-wave inversion (symmetric, deep in "Wellens' syndrome" — indicates critical proximal LAD stenosis)
- No ST elevation; no Q waves (distinguishes from STEMI)
- Normal ECG in up to 1–6% of confirmed NSTEMIs — serial ECGs are mandatory
- New LBBB or paced rhythm with concordant ST elevation should be treated as STEMI-equivalent
3. Atrial Fibrillation (AF)
Pathophysiology: Chaotic disorganized atrial electrical activity with multiple re-entrant wavelets; AV node conducts irregularly.
ECG Changes:
- Absent P waves — replaced by irregular fibrillatory (f) waves (most visible in V1)
- Irregularly irregular RR intervals — the cardinal feature
- Narrow QRS complexes (unless aberrant conduction/accessory pathway present)
- Variable ventricular rate (60–160 bpm depending on AV nodal conduction)
- Coarse f-waves (>1 mm): may indicate mitral valve disease; fine f-waves: more common in lone AF

Source: Guyton & Hall Textbook of Medical Physiology; Tintinalli's Emergency Medicine
4. Complete (Third-Degree) AV Heart Block
Pathophysiology: Complete failure of conduction between atria and ventricles; atria and ventricles beat independently.
ECG Changes:
- Complete AV dissociation — P waves and QRS complexes bear no relationship to each other
- Regular P-P intervals (atrial rate 60–100 bpm) independent of regular RR intervals
- Escape rhythm determines QRS morphology:
- Junctional escape (block in AV node): narrow QRS, rate 40–60 bpm
- Ventricular escape (block in His-Purkinje): wide QRS >120 ms, rate 20–40 bpm
- PR interval varies beat to beat (no fixed PR interval)
- Requires permanent pacemaker even if asymptomatic (Mobitz II, complete block)

Source: Harrison's Principles of Internal Medicine 22E
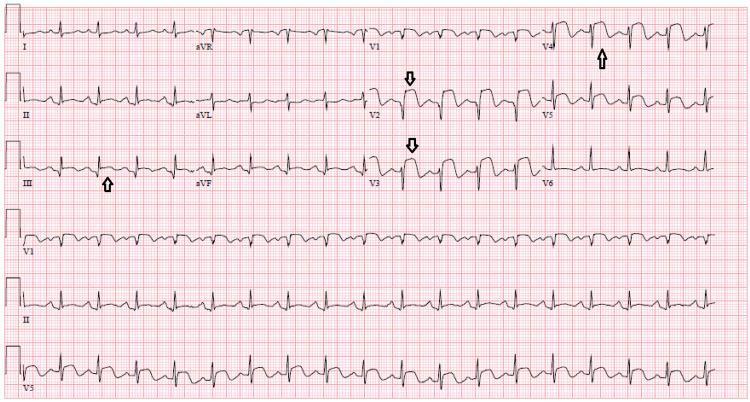
5. Acute Pericarditis
Pathophysiology: Inflammation of the pericardium causes widespread myocardial irritation and superficial epicardial injury.
ECG Changes (4 classic stages):
- Stage 1 (early): Diffuse saddle-shaped (concave) ST elevation in all leads except aVR and V1 + PR depression (most prominent in lead II) + PR elevation in aVR
- Stage 2 (days): ST normalises; T-waves flatten
- Stage 3 (weeks): Diffuse T-wave inversions
- Stage 4: ECG normalises
- Spodick's sign: downsloping TP segment
- Key differentiator from STEMI: Diffuse ST elevation not confined to one vascular territory; no reciprocal changes except in aVR; no Q waves

6. Pulmonary Embolism (PE)
Pathophysiology: Acute right ventricular pressure overload due to pulmonary vascular obstruction; acute cor pulmonale.
ECG Changes (most common: sinus tachycardia alone):
- Sinus tachycardia — most frequent finding (~44%)
- S1Q3T3 pattern: Deep S-wave in lead I, Q-wave in lead III, T-wave inversion in lead III — present in ~20%, specific but not sensitive
- Right axis deviation (acute)
- Right bundle branch block (complete or incomplete) — reflects RV strain
- T-wave inversions V1–V3 — RV strain pattern
- P pulmonale (tall peaked P >2.5 mm in II): right atrial enlargement
- Sinus tachycardia alone in many cases — a normal ECG does NOT exclude PE
7. Hypertrophic Cardiomyopathy (HCM)
Pathophysiology: Asymmetric septal hypertrophy (usually autosomal dominant sarcomere mutation) causing LV outflow tract obstruction, diastolic dysfunction.
ECG Changes (abnormal in ~95% of patients):
- Left ventricular hypertrophy (LVH) voltage criteria:
- Sokolow-Lyon: S(V1) + R(V5/V6) >35 mm
- Cornell: R(aVL) + S(V3) >28 mm (men) / >20 mm (women)
- Deep, symmetric T-wave inversions in lateral leads (V4–V6, I, aVL) — "giant T-wave inversions" especially in apical HCM (Yamaguchi syndrome) in V2–V5
- Septal Q waves in I, aVL, V5, V6 (due to hypertrophied septum)
- Left atrial enlargement (bifid P waves — P mitrale)
- ST depression in lateral leads
- Left axis deviation
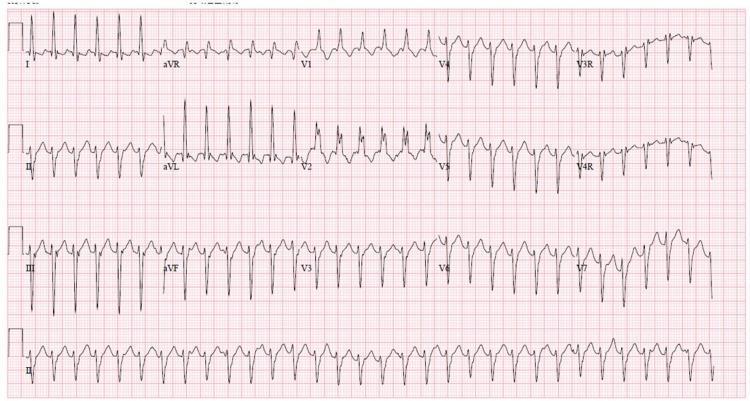
8. Ventricular Tachycardia (VT)
Pathophysiology: Rapid ventricular depolarization from a ventricular ectopic focus or re-entry circuit; often on background of structural heart disease (post-MI scar, cardiomyopathy).
ECG Changes:
- Rate ≥100 bpm, regular
- Wide QRS ≥120 ms (>160 ms strongly favors VT over SVT with aberrancy)
- AV dissociation — P waves march independently through QRS complexes (pathognomonic for VT)
- Fusion beats and capture beats (Dressler beats) — pathognomonic
- Concordance in precordial leads: all positive or all negative V1–V6 (positive concordance = VT)
- Axis deviation (extreme right or northwest axis common)
- Brugada criteria / Wellens criteria help distinguish from SVT with aberrancy
Types:
- Monomorphic VT: uniform QRS morphology (usually re-entry in MI scar)
- Polymorphic VT / Torsades de Pointes: changing QRS axis, triggered by long QT
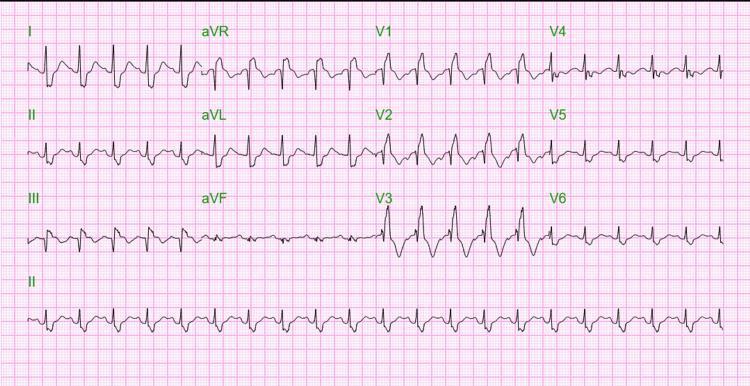
9. Wolff-Parkinson-White (WPW) Syndrome
Pathophysiology: An accessory pathway (Bundle of Kent) bypasses the AV node, causing ventricular pre-excitation. Risk of life-threatening fast AF conducting rapidly to ventricles.
ECG Changes (classic triad):
- Short PR interval <120 ms — AV node is bypassed
- Delta wave — slurred upstroke at onset of QRS (slow antegrade conduction via accessory pathway)
- Wide QRS >120 ms — broadened by delta wave
- Secondary ST-T changes: ST depression and T-wave inversion in direction opposite delta wave
- Pseudoinfarction pattern: negative delta waves in inferior leads can mimic pathological Q waves
- Accessory pathway localisation by delta wave polarity in various leads
| WPW Type A | WPW Type B |
|---|---|
| +ve delta in V1 | −ve delta in V1 |
| Left posterior pathway | Right-sided pathway |

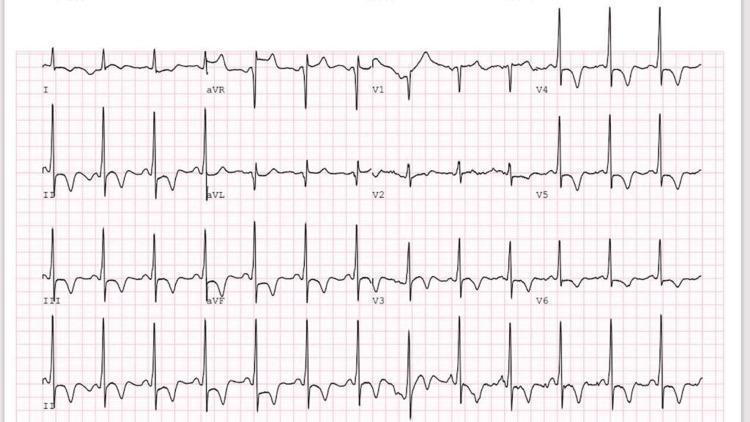
10. First-Degree AV Block
Pathophysiology: Slowed but uninterrupted conduction through the AV node (usually benign; can occur with myocarditis, inferior MI, digoxin, beta-blockers, hyperkalemia, aging).
ECG Changes:
- Prolonged PR interval >200 ms (>5 small squares) on every beat — constant
- All P waves are followed by QRS complexes (1:1 conduction maintained)
- Normal P-wave morphology and axis
- Normal QRS unless coexisting bundle branch block
- Often asymptomatic; rarely requires treatment
(Compare: Mobitz I / Wenckebach = PR progressively lengthens then a QRS drops; Mobitz II = fixed PR then sudden dropped QRS without warning — requires pacing)
Source: Harrison's Principles of Internal Medicine 22E, Fuster & Hurst's The Heart 15e
Quick Reference Summary Table
| # | Disease | Key ECG Finding | Rate | Rhythm |
|---|---|---|---|---|
| 1 | STEMI | ST elevation + Q waves (regional) | Usually normal | Regular |
| 2 | NSTEMI/UA | ST depression, T-wave inversion | Normal–fast | Regular |
| 3 | Atrial Fibrillation | No P waves, irregular RR | Variable | Irregularly irregular |
| 4 | Complete Heart Block | AV dissociation, escape rhythm | Slow (20–60) | Regular but dissociated |
| 5 | Pericarditis | Diffuse saddle ST elevation, PR depression | Normal–fast | Regular |
| 6 | Pulmonary Embolism | S1Q3T3, RBBB, RV strain | Fast | Regular |
| 7 | HCM | LVH voltage, giant T inversions, septal Q waves | Normal | Regular |
| 8 | Ventricular Tachycardia | Wide QRS ≥120 ms, AV dissociation | Fast (≥100) | Regular |
| 9 | WPW Syndrome | Short PR, delta wave, wide QRS | Normal | Regular (± paroxysmal SVT) |
| 10 | 1st-Degree AV Block | PR >200 ms, all P waves conducted | Normal | Regular |
Sources: Harrison's Principles of Internal Medicine 22E (2025), Tintinalli's Emergency Medicine, Fuster & Hurst's The Heart 15e, Guyton & Hall Medical Physiology, Goldman-Cecil Medicine.
This is a shared conversation. Sign in to Orris to start your own chat.