Deltoid ligament
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information from four authoritative textbooks. Here is a detailed synthesis:
Deltoid Ligament
The deltoid ligament (also called the medial collateral ligament of the ankle) is the primary stabilizer of the medial ankle. It is large, strong, and triangular in shape, with its apex attached to the medial malleolus above and its broad base spreading across the navicular, talus, and calcaneus below.
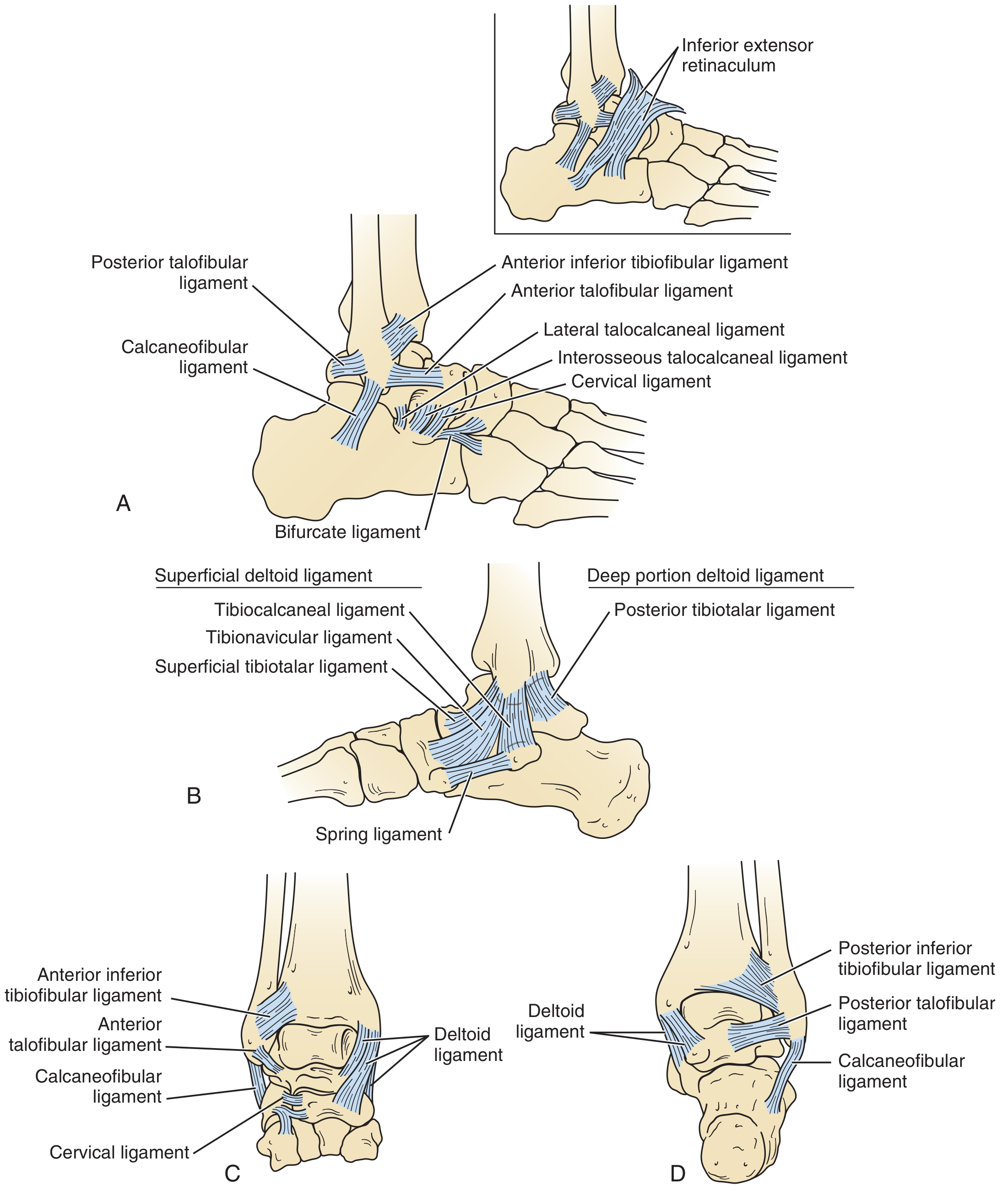
Anatomy and Components
The deltoid ligament is organized into two layers - superficial and deep - with a total of five to six named components depending on the classification used.
Superficial Layer
Spans both the tibiotalar and subtalar joints. It consists of:
| Component | Proximal Attachment | Distal Attachment | Primary Function |
|---|---|---|---|
| Tibionavicular | Anterior colliculus of medial malleolus | Dorsomedial navicular (anteriorly) | Resists eversion / valgus tilt |
| Tibiospring (tibioligamentous) | Medial malleolus | Spring ligament (plantar calcaneonavicular ligament) | Supports medial longitudinal arch |
| Tibiocalcaneal | Medial malleolus | Sustentaculum tali of calcaneus | Resists valgus/eversion |
| Superficial posterior tibiotalar | Medial malleolus | Medial surface of talus | Secondary restraint |
Deep Layer
Spans only the tibiotalar joint. Both components are intraarticular but extrasynovial:
| Component | Attachment | Primary Function |
|---|---|---|
| Deep anterior tibiotalar | Undersurface of medial malleolus | Medial talar body |
| Deep posterior tibiotalar | Undersurface of medial malleolus | Medial tubercle of talus |
The posterior deep tibiotalar ligament is the strongest component of the entire deltoid complex. - Campbell's Operative Orthopaedics 15th Ed.
Biomechanical Functions
- Primary stabilizer of the medial ankle during stance phase
- The deep layer primarily resists lateral talar translation and external rotation
- The superficial layer primarily resists valgus/eversion forces (talar tilt)
- Both layers act as secondary restraints against anterior translation of the talus
- Contributes to ankle mortise integrity alongside the syndesmosis
Clinical Relevance
Injury Pattern
- Isolated partial ruptures are reported; isolated complete ruptures are rare
- Deltoid injury most commonly occurs alongside:
- Lateral malleolar fractures (bimalleolar or trimalleolar pattern)
- Syndesmotic injuries
- Lateral ankle sprains (72% of lateral instability cases have concomitant deltoid injury)
- Osteochondral lesions
- 43% of ankle instability patients have injury to both deep and superficial components
- Incidence of deltoid lesions significantly increases with complete rupture of the anterior talofibular ligament (ATFL)
Diagnosis
- Stress radiographs: valgus/varus stress views showing medial clear space widening (>4 mm is pathological)
- MRI: gold standard to define extent and location of injury; comparison views useful
- On physical exam: tenderness over medial malleolus, pain with eversion stress
Treatment
Non-operative:
- Isolated complete disruption without fracture: below-knee non-weight-bearing cast
Operative (acute repair indications):
- Active patients with complete rupture demonstrated on MRI or with abnormal talar tilt/shift in mortise
- Concomitant fibula fracture with lateral talar shift (classic "bimalleolar equivalent")
- Technique: direct repair with imbrication using suture anchors, restoring tibionavicular and tibiocalcaneal attachments
Deltoid ligament reconstruction (chronic instability):
- Indicated for failed conservative management, chronic medial instability, or valgus ankle deformity
- Secondary reconstruction often needed when unstable valgus hindfoot is corrected (e.g., flatfoot reconstruction, subtalar arthrodesis) - removing hindfoot valgus unmasks deltoid incompetence
Association with Hindfoot Deformity
Deltoid incompetence is closely associated with adult-acquired flatfoot deformity (posterior tibial tendon dysfunction). Once a valgus hindfoot is made rigid by arthrodesis, increased valgus stress is transmitted through the incompetent deltoid, necessitating concurrent reconstruction.
Sources:
- Gray's Anatomy for Students, p. 5229-5239
- Campbell's Operative Orthopaedics 15th Ed. (2026), pp. 5087-5102, 5594-5656
- Miller's Review of Orthopaedics 9th Ed., p. 375-383
- Imaging Anatomy - Bones, Joints, Vessels and Nerves, pp. 579-588
This is a shared conversation. Sign in to Orris to start your own chat.