Teach me hypersensitive rxn according to microbiology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the content I need. Let me compile the comprehensive answer.
Hypersensitivity Reactions - Microbiology
Hypersensitivity is a condition in which an exaggerated or augmented immune response occurs that is harmful to the host. It requires a presensitized state - reactions typically occur after the second encounter with a specific antigen (allergen).
In 1963, Coombs and Gell classified hypersensitivity into four types:
- Types I, II, III - Antibody mediated
- Type IV - T-cell mediated
Quick Reference Table
| Type | Name | Onset | Mediator | Key Examples |
|---|---|---|---|---|
| I | Immediate / Anaphylactic | < 30 min | IgE, mast cells | Hay fever, asthma, anaphylaxis |
| II | Cytotoxic / Antibody-dependent | < 8 hr | IgG/IgM + complement | Transfusion reactions, Goodpasture syndrome |
| III | Immune Complex | < 8 hr | IgG + complement (complexes) | Serum sickness, post-streptococcal GN |
| IV | Delayed-Type (DTH) | 24-72 hr (up to 1 week) | T cells (CD4 Th1), macrophages | Tuberculin test, contact dermatitis |
(Source: Medical Microbiology 9e, Table 10.5)
Type I: Immediate Hypersensitivity (Allergy / Anaphylactic)
Mechanism
- Sensitization phase: Antigen (allergen) induces formation of IgE antibody, which binds firmly via its Fc portion to high-affinity IgE receptors (FcεRI) on mast cells, basophils, and eosinophils.
- Elicitation phase (second exposure): The allergen cross-links the cell-bound IgE molecules → triggering degranulation and release of pharmacologically active mediators.
- Late-phase reaction (8-12 hours later): Infiltration of eosinophils and CD4 T cells + cytokine reinforcement of inflammation.
Mediators Released
Primary (preformed) mediators:
- Histamine - causes vasodilation, increased capillary permeability, bronchospasm
Secondary (newly formed) mediators:
- Prostaglandins - edema, bronchoconstriction
- Leukotrienes: LTB4 (chemoattractant for leukocytes), LTC4 + LTD4 (vasodilation, vascular permeability)
- TNF-α and IL-4
- Platelet-activating factor, tryptase, kininogenase
Clinical Forms
- Systemic anaphylaxis - after IV administration of heterologous proteins, bee stings, penicillin
- Atopy (local reactions) - strong familial predisposition, elevated IgE levels. Includes hay fever, asthma, eczema, urticaria
- Triggered by environmental allergens (pollens, house dust) or food (shellfish)
Treatment
- Acute: Epinephrine, antihistamines, corticosteroids; maintain airway
- Prevention: Identify antigen (skin test or IgE serology), avoid allergen
- Desensitization ("allergy shots"): Induces IgG to bind allergen and prevent allergen binding to IgE
(Source: Jawetz Melnick & Adelberg's Medical Microbiology 28e, p. 152)
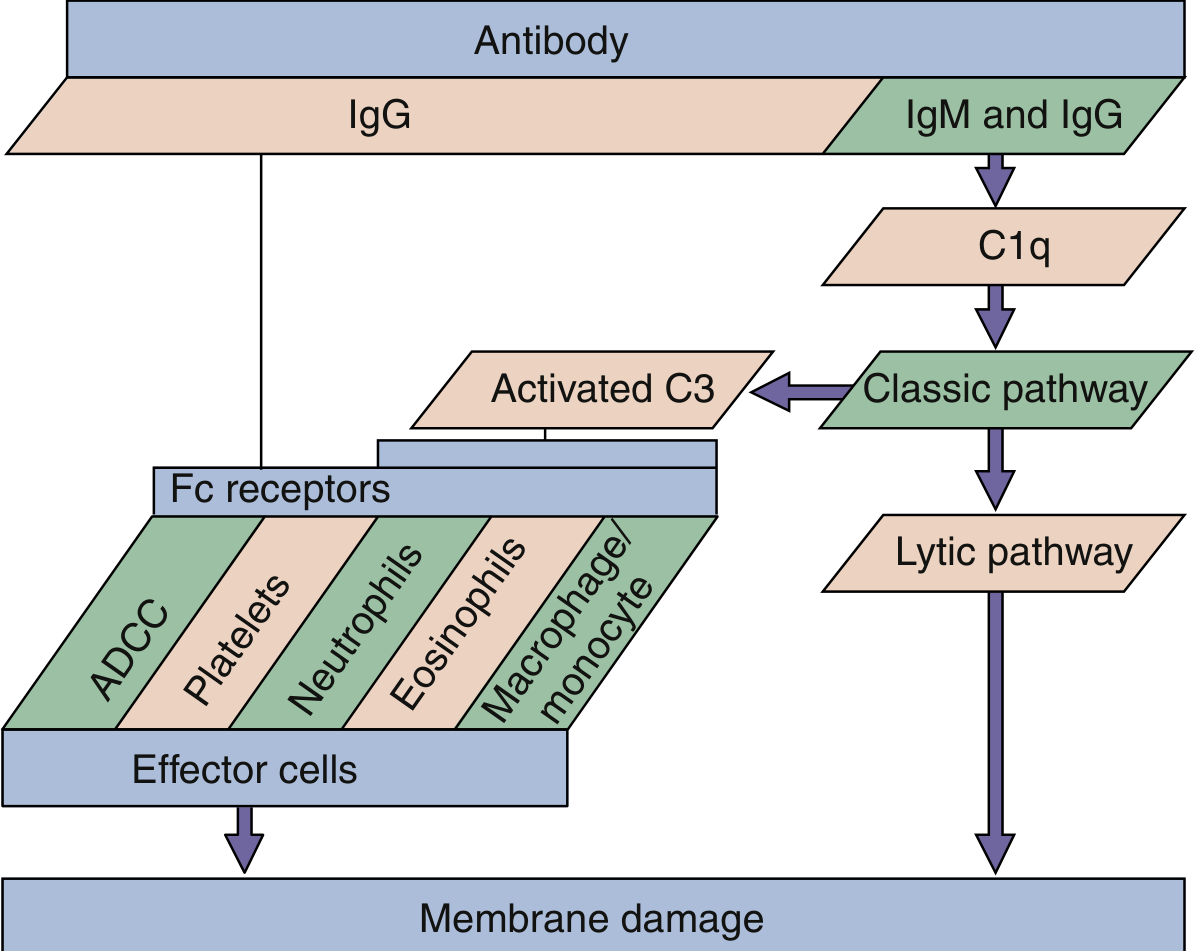
Type II: Cytotoxic / Antibody-Dependent Hypersensitivity
Mechanism
IgG (or IgM) antibodies bind to cell surface antigens or extracellular matrix molecules.
Two pathways of damage:
- Complement activation (IgM and IgG → C1q → classical pathway → lytic pathway) → membrane damage
- ADCC (Antibody-Dependent Cellular Cytotoxicity) - IgG binds target cell; Fc receptors on ADCC effectors (neutrophils, eosinophils, macrophages/monocytes, platelets) engage → membrane damage
Clinical Examples
| Disease | Mechanism |
|---|---|
| ABO transfusion reactions | Anti-A/B IgM → complement-mediated hemolysis of transfused RBCs |
| Hemolytic disease of newborn (Rh incompatibility) | Maternal IgG crosses placenta → destroys fetal RBCs |
| Autoimmune hemolytic anemia | Antibodies to self-RBC antigens |
| Goodpasture syndrome | IgG to basement membranes of kidney and lung → complement activation + leukocyte chemotaxis + severe membrane damage |
| Myasthenia gravis | IgG to acetylcholine receptors on neurons → blocks transmission |
| Graves disease | Autoantibody binds TSH receptor → stimulates thyroid (hyperthyroidism) - no cell injury but altered function |
| Penicillin-induced hemolysis | Penicillin (hapten) attaches to RBC surface proteins → antibody formation → hemolysis |
Note: Graves disease represents a special subtype sometimes called Type V (stimulatory) hypersensitivity in Roitt's classification, where antibody stimulates rather than destroys the target cell.
(Source: Jawetz 28e, p. 152; Medical Microbiology 9e, p. 120)
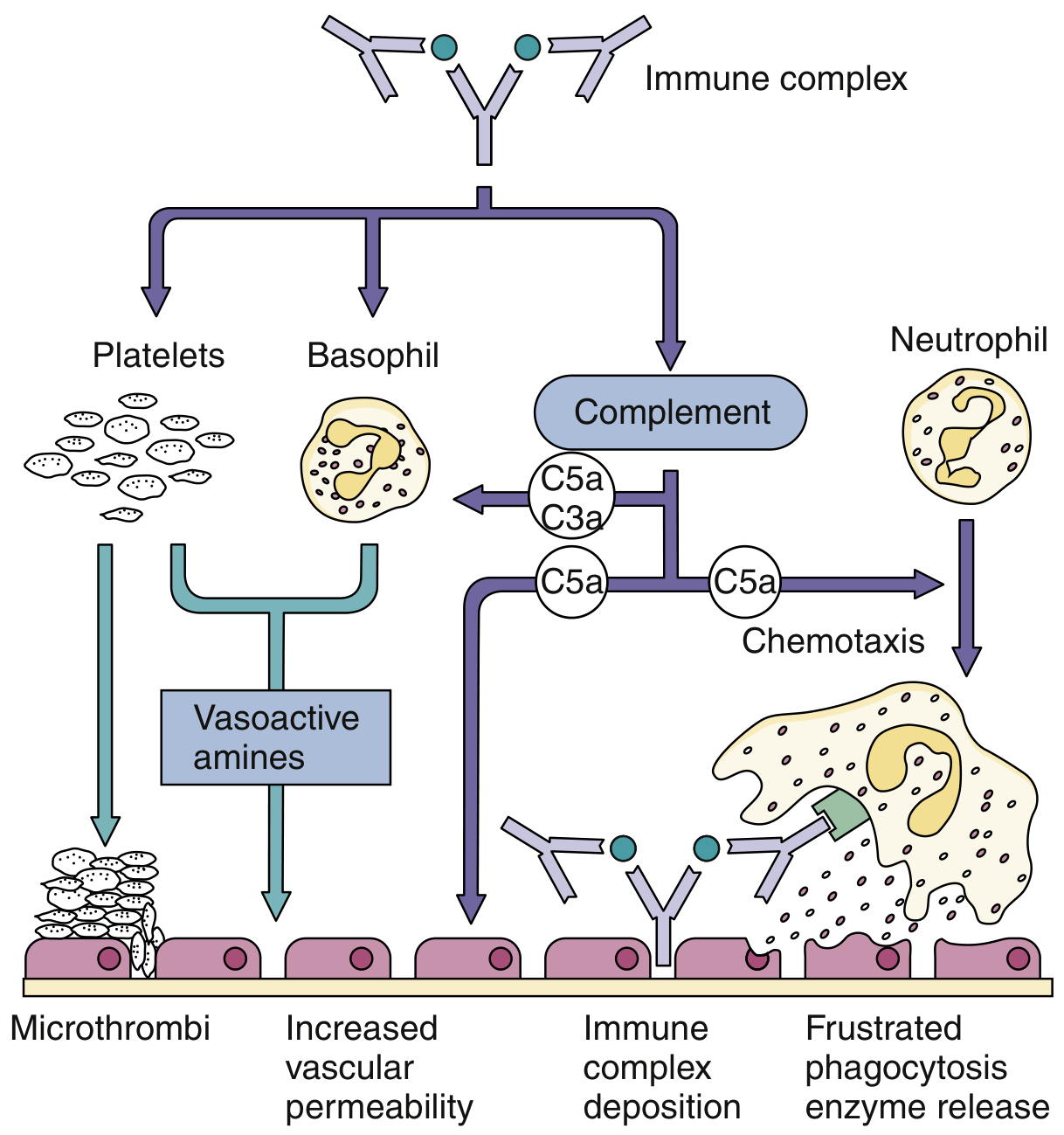
Type III: Immune Complex Hypersensitivity
Mechanism
When antibody (IgG) combines with specific soluble antigens → immune complexes form. Normally cleared, but if they persist and deposit in tissues (especially kidneys, joints, blood vessels), they activate the complement cascade → inflammation and tissue injury.
Key sequence:
- Abundant soluble antigen in bloodstream
- Large antigen-antibody complexes form
- Complexes trapped in capillaries (especially kidney, joints, vessel walls)
- Classical complement cascade activated → C3a and C5a generated
- Chemotaxis of neutrophils and macrophages to site
- Phagocytosis frustrated by deposited complexes → enzyme release → tissue damage
- Microthrombi formation, increased vascular permeability
Two Major Forms
| Form | Description |
|---|---|
| Arthus reaction (localized) | Low dose antigen injected into skin → local IgG production + complement activation → mast cells + neutrophils release mediators → vascular permeability ↑ (within 12 hours) |
| Serum sickness (generalized) | Systemic disease; occurs after receiving animal immunoglobulin (e.g., antisnake venom) on multiple occasions |
Clinical Examples
- Acute poststreptococcal glomerulonephritis - streptococcal Ag-Ab complexes filtered by glomeruli → complement fixation → neutrophil influx → kidney damage. Low complement levels; "lumpy" IgG + C3 deposits on glomerular basement membrane (seen on immunofluorescence)
- Serum sickness
- Hepatitis B-associated polyarteritis nodosa (viral antigen complexes)
- Malaria, staphylococcal endocarditis (microbial antigen complexes)
- SLE, Rheumatoid arthritis (autoimmune complexes)
- Hypersensitivity pneumonitis (persistent inhalation of mold, plant, or animal antigens)
(Source: Jawetz 28e, p. 152; Medical Microbiology 9e, p. 121)
Type IV: Cell-Mediated (Delayed-Type) Hypersensitivity (DTH)
Mechanism
T-cell-mediated response - no antibody involvement.
- Antigen is processed and presented to circulating CD4 Th1 cells (via MHC class II on APCs)
- Sensitized T cells recognize antigen upon re-exposure
- T-cell proliferation + release of cytokines (IFN-γ, IL-2)
- Macrophage activation → inflammatory response
- Onset: typically 24-72 hours after antigen contact
Key: It takes 24-48 hours for antigen to be presented to T cells, for them to migrate to the site, and then activate neutrophils and macrophages.
Two Major Forms
A. Contact Hypersensitivity
- Sensitizing agents: simple chemicals (nickel, formaldehyde, poison ivy/oak), topical medications (sulfonamides, neomycin), cosmetics, soaps
- Mechanism: small molecules (haptens) enter the skin → attach to body proteins → form complete antigens → Langerhans cells in epidermis interact with CD4 Th1 cells
- Re-exposure: erythema, itching, vesication, eczema, or necrosis of skin within 12-48 hours

B. Tuberculin-Type Hypersensitivity (Classic DTH)
- Tuberculin (PPD) skin test is the classic example
- Small amount of tuberculin injected intradermally
- Little immediate reaction, then induration and redness peak at 24-72 hours
- Mononuclear cells (especially CD4 Th1) accumulate in subcutaneous tissue
- Positive test = prior exposure to M. tuberculosis (not necessarily active disease)
- A change from negative to positive = recent infection, possible current activity
C. Granulomatous Hypersensitivity (Chronic DTH)
- Occurs when intracellular organism cannot be cleared (persistent stimulation)
- Diseases: tuberculosis, leprosy, schistosomiasis, sarcoidosis, Crohn disease
- Granulomas = epithelioid cells (chronically activated macrophages) + multinucleated giant cells + surrounding lymphocytes + fibrosis
- Require sustained CD4 T cell-derived IFN-γ to restrict spread of M. tuberculosis
(Source: Jawetz 28e, p. 153; Medical Microbiology 9e, p. 121)
Summary: Key Distinguishing Features
| Feature | Type I | Type II | Type III | Type IV |
|---|---|---|---|---|
| Mediator | IgE | IgG/IgM | IgG + soluble Ag | CD4 Th1 cells |
| Complement | No | Yes (classical) | Yes (classical) | No |
| Onset | Seconds-30 min | Hours | Hours | 24-72+ hr |
| Effector cells | Mast cells, basophils | Complement, ADCC cells | Neutrophils | Macrophages, T cells |
| Antigen type | Soluble (allergen) | Cell-surface bound | Soluble (in complexes) | Intracellular / contact |
| Transfer | Serum (IgE) | Serum (IgG) | Serum | Cells (T cells) |
| Key test | Skin prick test | Direct Coombs test | Serum complement levels | Tuberculin (PPD) test |
Sources:
- Jawetz Melnick & Adelberg's Medical Microbiology 28e pp. 151-153 - Hypersensitivity chapter
- Medical Microbiology 9e pp. 120-122 - Hypersensitivity Responses
This is a shared conversation. Sign in to Orris to start your own chat.