Allergic rhinitis. Ms ent University exam pattern for 20 marks.
Allergic Rhinitis - University Exam Answer (20 Marks)
Definition
Classification (ARIA Guidelines)
- Intermittent AR - symptoms <4 days/week OR <4 consecutive weeks
- Persistent AR - symptoms ≥4 days/week AND ≥4 consecutive weeks
- Mild - no impairment of sleep, daily activities, school, or work
- Moderate-Severe - one or more of the above impaired
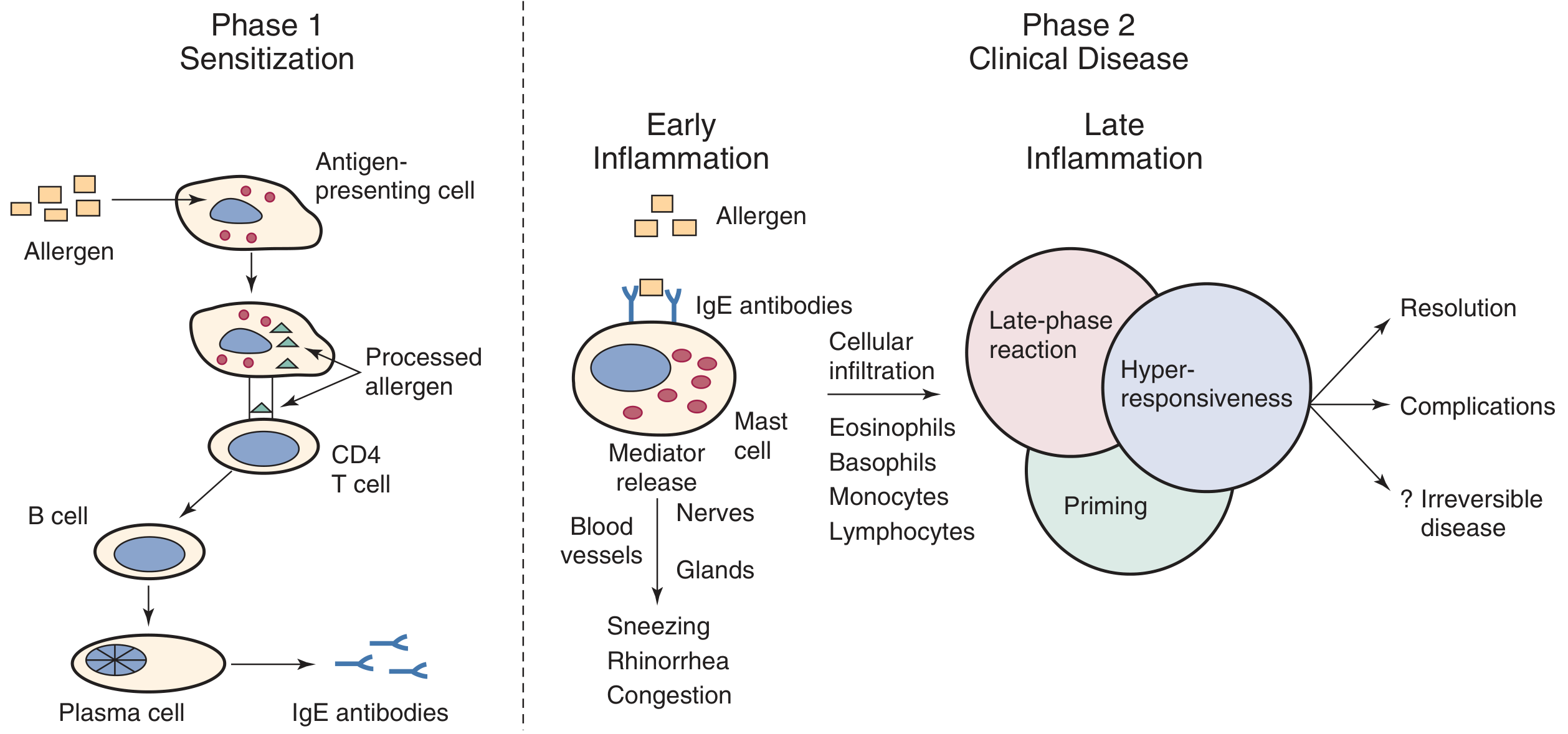
Pathophysiology
Phase 1 - Sensitization
- An inhaled allergen is deposited on the nasal mucosa
- Antigen-presenting cells (macrophages, dendritic cells, Langerhans cells) engulf and process the antigen, presenting it on MHC class II molecules to naive TH0 helper T cells
- Mucosal epithelial cells secrete TSLP, which induces TH2-polarizing dendritic cells
- TH0 cells differentiate into TH2 lymphocytes under IL-4 and IL-13 signaling
- TH2 cells activate B cells via CD40L-CD40 interaction, class-switching to produce IgE
- IgE binds to high-affinity Fc-epsilon-RI receptors on mast cells and basophils in the nasal mucosa
- The patient is now sensitized - no symptoms yet
Phase 2 - Clinical Disease (Re-exposure)
- Re-exposure to the same allergen cross-links IgE on mast cells
- Mast cell degranulation releases preformed mediators: histamine, tryptase, kinins
- Newly synthesized mediators: prostaglandin D2 (PGD2), leukotrienes (LTC4, LTD4, LTE4), platelet-activating factor
- Histamine acts on H1 receptors → sneezing, itching, rhinorrhoea
- Congestion is driven primarily by leukotrienes and PGD2
- Recruitment of eosinophils, basophils, monocytes, T lymphocytes to the nasal mucosa
- Sustained inflammation, nasal hyperresponsiveness, and priming (reduced threshold for subsequent allergen triggers)
- Responsible for nasal congestion and prolonged symptoms
Aetiology / Common Allergens
| Type | Examples |
|---|---|
| Seasonal (intermittent) | Tree pollen (spring), grass pollen (summer), weed pollen (autumn) |
| Perennial (persistent) | House dust mite (Dermatophagoides pteronyssinus), cockroach, pet dander (cat, dog), mold spores |
| Occupational | Latex, grain dust, animal proteins, wood dust |
Clinical Features
Symptoms (Cardinal tetrad):
- Nasal pruritus (itching) - often extends to palate, eyes, throat
- Paroxysmal sneezing - often in runs of 10-20 sneezes
- Watery rhinorrhoea - clear, thin, profuse
- Nasal congestion/obstruction - most bothersome symptom; worse lying down
- Ocular: itching, lacrimation, conjunctival injection (allergic conjunctivitis - in up to 80%)
- Anosmia/hyposmia
- Post-nasal drip → throat clearing, cough
- Sleep disturbance, fatigue, decreased concentration ("brain fog")
- Eustachian tube dysfunction → ear fullness, clicking
Signs on Examination:
- "Allergic salute" - transverse nasal crease from repeatedly rubbing the nose upward with the palm
- "Allergic shiners" - infraorbital dark circles from venous stasis
- "Dennie-Morgan lines" - extra fold of skin below lower eyelid
- Mouth breathing, "adenoid facies" in chronic childhood cases
- Nasal mucosa: pale, bluish/violaceous, boggy, edematous (no appearance is pathognomonic)
- Inferior turbinates: enlarged, coated with thin clear secretions
- Watery discharge on the nasal floor
- Nasal polyps (in chronic/eosinophilic disease)
Investigations
1. Allergy Skin Prick Test (SPT) - Gold standard
- Allergen extract applied epicutaneously with a 1 mm lancet
- Positive control: histamine; Negative control: diluent
- Positive = wheal ≥3 mm greater than negative control at 15-20 min
- Sensitivity 80-100%, specificity 70-90%
- Advantages: cheap, quick, multiple allergens tested simultaneously, low anaphylaxis risk
- Contraindications: severe eczema, dermographism, beta-blocker use, pregnancy, recent antihistamine use (stop antihistamines 5-7 days prior)
2. Intradermal Testing
- More sensitive but less specific than SPT
- Higher risk of systemic reactions; not used as first-line
3. In Vitro Serum Specific IgE (ImmunoCAP / RAST)
- Measures allergen-specific IgE levels in serum
- Used when SPT is not possible (extensive eczema, dermographism, can't stop antihistamines, high anaphylaxis risk)
- Slightly less sensitive than SPT but equivalent overall
- Results reported in kU/L (class 0-6)
4. Total Serum IgE
- Non-specific; elevated in atopy but also in parasitic infection, eczema
- Not useful for diagnosis alone
5. Nasal Cytology / Biopsy
- Nasal smear showing >20% eosinophils supports allergic diagnosis
- Rarely used in routine practice
6. Nasal Endoscopy
- To rule out polyps, septal deviation, tumour, central compartment atopic disease
7. Other (if indicated)
- Full blood count: peripheral eosinophilia (non-specific)
- CT paranasal sinuses: to evaluate complications (sinusitis, polyps)
Differential Diagnosis
| Condition | Distinguishing Feature |
|---|---|
| Non-allergic (vasomotor) rhinitis | Triggered by cold air, irritants, exercise; no IgE sensitization |
| Infectious rhinitis | Purulent discharge, fever, unilateral |
| NARES (Non-allergic rhinitis with eosinophilia) | Nasal eosinophilia, negative skin testing |
| Drug-induced rhinitis (rhinitis medicamentosa) | History of prolonged oxymetazoline use |
| Hormonal rhinitis | Pregnancy, hypothyroidism |
| Nasal polyps/tumour | Unilateral, bloody discharge |
| CSF rhinorrhoea | Unilateral, clear, salty; halo test, beta-2-transferrin |
Treatment
Step 1 - Allergen Avoidance
- Identify specific allergens via testing; implement avoidance strategies
- For house dust mite: mattress covers, washing bedding at 60°C, reducing humidity
- For pollen: stay indoors on high-count days, wear glasses outdoors
- For pets: remove animal from home (most effective)
Step 2 - Pharmacotherapy
- Most effective single agent for all symptoms including congestion
- Examples: Mometasone furoate, fluticasone propionate, budesonide, beclomethasone
- Onset: 3-7 days for full effect; must use regularly
- Preferred over antihistamines for moderate-severe AR
- Examples: Cetirizine, loratadine, fexofenadine, levocetirizine, desloratadine
- Effective for itching, sneezing, rhinorrhoea; less effective for congestion
- Non-sedating; no anticholinergic effects
- First-generation antihistamines (chlorphenamine) cause sedation - avoid for driving
- Azelastine, olopatadine - faster onset than oral, effective for sneezing, itching
- Can be used as monotherapy or combined with INCS
- Pseudoephedrine (oral), oxymetazoline (nasal)
- Effective for congestion; short-term use only (max 3-5 days for nasal)
- Prolonged use → rhinitis medicamentosa (rebound congestion)
- Montelukast - especially useful when AR coexists with asthma
- Less effective than INCS as monotherapy
- Mast cell stabilizer; poor bioavailability; requires dosing 4-6x/day
- Safe in children and pregnancy; largely replaced by INCS
- Anticholinergic; reduces rhinorrhoea specifically; no effect on other symptoms
- Short courses (5-7 days) only for severe, refractory AR before important events
Step 3 - Allergen Immunotherapy (AIT) - Disease-modifying treatment
- Induces allergen-specific immune tolerance
- Shifts the TH2-dominant response toward TH1/Treg responses
- Increases production of blocking IgG4 antibodies that compete with IgE for allergen binding
- Induces IL-10 and TGF-beta producing regulatory T cells (Tregs)
- Reduces mast cell and basophil responsiveness
- Decreases IgE production over time
- Confirmed IgE-sensitized AR (positive SPT/serum IgE)
- Inadequate control with pharmacotherapy or patient preference to avoid long-term drugs
- Comorbid allergic asthma
- Multiple allergies with limited avoidance options
- Subcutaneous Immunotherapy (SCIT) - traditional; injections build-up phase (weekly for 3-6 months) then maintenance (monthly for 3-5 years). Risk of systemic reactions - must be given in clinic with 20-30 min observation.
- Sublingual Immunotherapy (SLIT) - drops or tablets placed under tongue; home-administered; safer profile; FDA-approved tablets for grass, ragweed, dust mite.
Complications
- Rhinosinusitis (chronic sinusitis) - most common; impaired mucociliary clearance
- Nasal polyposis - especially in eosinophilic/aspirin-sensitive disease
- Otitis media with effusion (glue ear) - via Eustachian tube dysfunction
- Asthma - "united airway disease"; AR is a risk factor for developing asthma; ARIA concept of "one airway, one disease"
- Sleep-disordered breathing / obstructive sleep apnea
- Reduced quality of life, academic and occupational impairment
Key Points for Exam
| Aspect | Key Fact |
|---|---|
| Mediator responsible for itch and sneezing | Histamine (H1) |
| Mediator responsible for congestion | Leukotrienes, PGD2 |
| Late phase cell | Eosinophil |
| Gold standard allergy test | Skin prick test |
| Most effective single drug | Intranasal corticosteroid |
| Disease-modifying treatment | Allergen immunotherapy |
| Hallmark mucosal appearance | Pale, bluish, boggy turbinates |
| Skin sign | Allergic salute, allergic shiners |
| ARIA classification basis | Duration (intermittent/persistent) + Severity (mild/moderate-severe) |
| AR + asthma concept | United airway disease |
Anatomy of osteomeatal complex. Ms ent University exam pattern for 20 marks.
Anatomy of the Osteomeatal Complex (OMC) - 20-Mark University Exam Answer
Definition
Location
- Medial: middle turbinate
- Lateral: lamina papyracea (medial orbital wall)
- Superior: fovea ethmoidalis (roof of ethmoid)
- Posterior: basal lamella of the middle turbinate
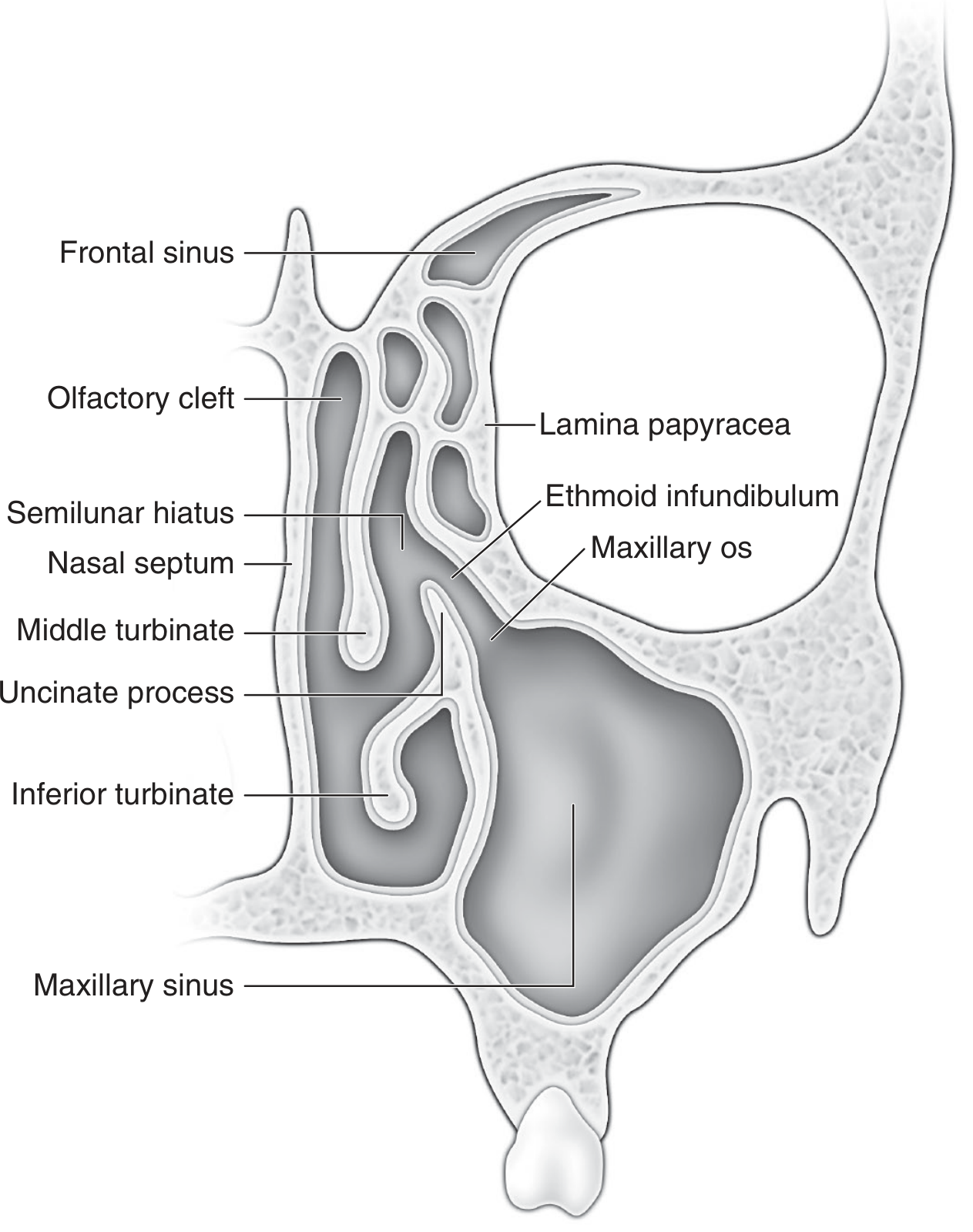
Components of the OMC
1. Middle Turbinate
- The middle turbinate (MT) is a projection of the ethmoid bone forming the medial boundary of the middle meatus
- Anteriorly, it attaches to the cribriform plate superiorly and the lateral nasal wall at the agger nasi
- Posteriorly, it emits the basal lamella, a bony plate running laterally to fuse with the lamina papyracea, dividing the ethmoid into anterior and posterior compartments
- The middle meatus is the air space lateral to the middle turbinate
- Clinical relevance: paradoxical middle turbinate (curving laterally) can obstruct the OMC
2. Uncinate Process
- Hook-like (sickle-shaped), sagittally oriented bone of ethmoid origin
- Dimensions: 3-4 mm wide, 1.5-2 cm long
- Lies in the sagittal plane, running anterosuperior to posteroinferior
- Its posterior free margin forms the anterior boundary of the hiatus semilunaris
- Anterosuperior: to the ethmoidal crest of the maxilla and lacrimal bone (at the lacrimal line)
- Posteroinferior: to the ethmoidal process of the inferior turbinate and palatine bone
- Inferior aspect: contributes to the medial wall of the maxillary sinus; natural ostium of maxillary sinus lies lateral and superior to this portion
| Superior Attachment | Frontal Sinus Drainage Route | Frequency |
|---|---|---|
| Lamina papyracea (LP) | Medial to UP, directly into middle meatus; superior infundibulum forms blind recessus terminalis | 80% (most common) |
| Skull base (fovea ethmoidalis) or middle turbinate | Lateral to UP, directly into ethmoidal infundibulum | 20% |
3. Ethmoidal Infundibulum
- A three-dimensional funnel-shaped trough (not a slit) that channels secretions into the middle meatus
- Functions as the common drainage channel for the maxillary sinus, anterior ethmoid cells, and (in some configurations) the frontal sinus
| Direction | Structure |
|---|---|
| Medial | Uncinate process (free edge) |
| Lateral | Lamina papyracea (medial orbital wall) |
| Posterior | Anterior wall of ethmoid bulla |
| Anterosuperior | Frontal process of maxilla |
| Superolateral | Lacrimal bone |
- Inferiorly: maxillary sinus ostium opens at ~45-degree angle into the inferior infundibulum
- Superiorly: frontal sinus (when uncinate attaches to skull base/MT) or anterior ethmoid cells
- The infundibulum is surgically accessed by passing a probe through the hiatus semilunaris
4. Hiatus Semilunaris
- A two-dimensional, crescent-shaped gap/slit (not a three-dimensional space)
- Lies between the free posterior edge of the uncinate process (anteriorly) and the anterior wall of the ethmoid bulla (posteriorly)
- Functions as the communication gateway between the middle meatus medially and the ethmoidal infundibulum laterally
- Secretions from maxillary, frontal, and anterior ethmoid sinuses pass through the hiatus semilunaris to enter the middle meatus
Key distinction: Hiatus semilunaris = 2D slit (opening); Ethmoidal infundibulum = 3D space (channel)
5. Ethmoid Bulla
- The largest and most constant anterior ethmoid air cell
- Lies posterior to the uncinate process and forms the posterior wall of the hiatus semilunaris
- Superiorly: its anterior wall may extend to the skull base, forming the posterior limit of the frontal recess
- Posteriorly: may blend with the basal lamella, or a space called the retrobullar recess may exist between the bulla and basal lamella
- The ethmoid bulla is enclosed laterally by the lamina papyracea
6. Frontal Recess
- The most anterior and superior part of the anterior ethmoid, connecting the frontal sinus to the middle meatus/infundibulum
- An hourglass-shaped drainage tract: frontal sinus → frontal infundibulum → frontal ostium (waist) → frontal recess (narrowest "tight spot") → middle meatus
- Bordered:
- Anteriorly: agger nasi cell (most constant anterior ethmoid cell)
- Posteriorly: anterior wall of ethmoid bulla
- Inferiorly: superior attachment of the uncinate process
7. Maxillary Sinus Ostium
- The natural ostium of the maxillary sinus drains into the inferior aspect of the ethmoidal infundibulum
- Located high on the medial wall of the maxillary sinus (near the roof) - functionally disadvantaged position (gravity works against drainage)
- Mucociliary transport compensates by actively sweeping mucus toward the ostium regardless of gravity
- The ostium lies lateral and superior to the inferior attachment of the uncinate process
8. Lamina Papyracea
- The paper-thin medial orbital wall, forming the lateral boundary of the OMC and the infundibulum
- Separates the ethmoid sinuses from the orbital contents
- Surgical landmark: dehiscences here can result in orbital injury during FESS
9. Agger Nasi Cell
- The most anterior ethmoid air cell, an ethmoturbinal remnant present in the majority of individuals
- Located anterior and inferior to the frontal recess
- Borders the frontal recess anteriorly
- When pneumatized extensively, it can narrow or obstruct the frontal recess
Anatomical Variations of Clinical Importance
| Variation | Description | Clinical Significance |
|---|---|---|
| Concha bullosa | Pneumatization of the middle turbinate | Narrows middle meatus, obstructs OMC |
| Paradoxical middle turbinate | Lateral convexity instead of medial | Obstructs middle meatus/OMC |
| Haller cell (infraorbital cell) | Ethmoid air cell extending inferior to orbit into the roof/lateral wall of maxillary sinus | Narrows infundibulum, predisposes to maxillary sinusitis |
| Onodi cell (sphenoethmoidal cell) | Posterior ethmoid cell extending lateral/posterior to sphenoid | Contains optic nerve - risk of blindness in FESS |
| Deviated nasal septum with high spur | Septal spur at level of middle meatus | Directly obstructs OMC |
| Accessory maxillary ostium | Perforated posterior fontanelle (20-30%) | Recirculation of mucus; not beneficial |
| Agger nasi hyperpneumatization | Enlarged agger nasi cell | Narrows frontal recess |
| Recessus terminalis | Blind superior pouch of infundibulum when uncinate attaches to LP | Frontal sinus drains medial to UP, not into infundibulum |
Three "Tight Spots" of Sinus Drainage (Cummings)
- Frontal recess - narrowest point in frontal sinus drainage
- Ethmoidal infundibulum - drainage channel from maxillary sinus to middle meatus
- Sphenoethmoidal recess - drainage of sphenoid sinus and posterior ethmoid cells
Mucociliary Clearance in the OMC
- Ciliated pseudostratified columnar epithelium lines all sinus mucosa
- Mucus is transported toward the natural ostia by coordinated ciliary beating, irrespective of gravity
- Maxillary sinus cilia beat toward the natural ostium (located superiorly/medially), then secretions pass through the infundibulum, through the hiatus semilunaris, into the middle meatus
- Mucociliary transport rate: 5-10 mm/min
- This explains why accessory ostia, while anatomically patent, do not improve drainage - cilia still direct secretions back to the natural ostium causing recirculation
Clinical Significance / Pathophysiology of Rhinosinusitis
- Mucosal oedema (from viral URI, allergy, pollution) causes swelling of OMC structures, particularly the uncinate process and middle turbinate mucosa
- This obstructs the hiatus semilunaris and infundibulum
- Ostial obstruction → impaired mucociliary clearance → stasis of secretions
- Reduced O2 tension within the sinuses → favors bacterial overgrowth
- Infection and inflammation → further oedema → vicious cycle
- Because all three sinuses (maxillary, frontal, anterior ethmoid) drain through this common pathway, a single point of obstruction can cause multisinus disease
Radiological Assessment - CT Paranasal Sinuses
- Coronal CT is the gold standard for evaluating OMC anatomy and pathology
- Shows the uncinate process, infundibulum, ethmoid bulla, middle turbinate, and their relationships
- Assessed before FESS to identify:
- Anatomical variants (Haller cell, concha bullosa, Onodi cell)
- Sites of disease/obstruction
- Lamina papyracea dehiscence
- Skull base height (low lying = risk of CSF leak)
- Lund-Mackay scoring system: grades each sinus (0-2) and the OMC (0-2) for CT opacification; maximum score 24
Relevance to FESS (Functional Endoscopic Sinus Surgery)
- Uncinectomy - removal of uncinate process; opens infundibulum
- Middle meatal antrostomy - enlarges natural maxillary ostium
- Anterior ethmoidectomy - removes anterior ethmoid cells including ethmoid bulla
- Frontal recess dissection - opens frontal drainage pathway
- (If needed) Posterior ethmoidectomy → Sphenoidotomy
Summary Table - OMC Components
| Structure | Type | Key Relations | Drainage/Function |
|---|---|---|---|
| Middle turbinate | Ethmoid bone projection | Lateral = middle meatus | Medial boundary of OMC |
| Uncinate process | Ethmoid bone, sickle-shaped | Post. free edge = hiatus | Medial wall of infundibulum |
| Ethmoidal infundibulum | 3D funnel space | Medial = UP; Lateral = LP; Post = EB | Drains maxillary + anterior ethmoid (± frontal) |
| Hiatus semilunaris | 2D crescent slit | Ant = UP; Post = EB | Gateway from infundibulum to middle meatus |
| Ethmoid bulla | Largest anterior ethmoid cell | Post = basal lamella; Lat = LP | Post boundary of hiatus |
| Frontal recess | Most ant/sup anterior ethmoid | Ant = agger nasi; Post = EB | Frontal sinus drainage |
| Maxillary ostium | Natural sinus opening | Opens into inf. infundibulum | Drains maxillary sinus |
| Lamina papyracea | Medial orbital wall | Lat boundary of infundibulum | Separates orbit from ethmoid |
Anatomy of osteomeatal complex. Ms ent University exam pattern for 20 marks as per book by renuka bradoo
Renuka Bradoo ENT textbook osteomeatal complex anatomy
osteomeatal complex anatomy uncinate process infundibulum hiatus semilunaris ethmoid bulla
osteomeatal complex anatomy uncinate process middle meatus infundibulum frontal recess
Bradoo "anatomical principles endoscopic sinus surgery" osteomeatal complex lateral nasal wall uncinate infundibulum "ground lamella"
Bradoo "anatomical principles endoscopic sinus surgery" "four lamellae" "hiatus semilunaris" "bulla ethmoidalis" "frontal recess" lateral nasal wall chapter 3
Anatomy of the Osteomeatal Complex
As per Bradoo's "Anatomical Principles of Endoscopic Sinus Surgery: A Step by Step Approach"
University Exam Answer - 20 Marks
Introduction / Definition
Embryological Basis - The Four Lamellae Concept (Bradoo's Foundation)
| Lamella | Structure Formed |
|---|---|
| 1st lamella | Uncinate process |
| 2nd lamella | Anterior wall of bulla ethmoidalis |
| 3rd lamella | Ground lamella (basal lamella) of middle turbinate |
| 4th lamella | Superior turbinate |
- The furrow between the 1st and 2nd lamellae (between uncinate and bulla) gives rise to the ethmoidal infundibulum, into which the maxillary, frontal, and anterior ethmoid sinuses pneumatize
- The furrow between 2nd and 3rd lamellae gives rise to the sinus lateralis of Grunwald
- The furrow between 3rd and 4th lamellae gives rise to the posterior ethmoid cells
- The 5th lamella (supreme turbinate) persists in only 15% of people
Bradoo's key teaching: Understanding the four lamellae means understanding the entire OMC - each structure can be traced back to its embryological origin.
Lateral Nasal Wall - Overall Structure
Middle Turbinate - Attachments (Three-Plane Concept)
- Anterior vertical attachment - to the lateral border of the cribriform plate (sagittal plane); most anterior portion
- Middle oblique attachment (Ground Lamella) - runs obliquely from the lateral nasal wall to the lamina papyracea (coronal plane); divides ethmoid into anterior (drain to middle meatus) and posterior (drain to superior meatus) compartments
- Posterior horizontal attachment - along the lamina papyracea and perpendicular plate of palatine bone to the posterior choana (horizontal plane)
Ground lamella (Bradoo's preferred term = basal lamella in other texts) is the critical surgical landmark separating anterior from posterior ethmoid cells. It must be breached to access posterior ethmoid cells in FESS.
Components of the Osteomeatal Unit (as per Bradoo)
1. Uncinate Process (1st Lamella)
- Lies in the sagittal plane, running anterosuperiorly to posteroinferiorly
- Anterior articulation: lacrimal bone (at the lacrimal/maxillary line)
- Posterior end: inferior turbinate and perpendicular plate of palatine bone
- Its posterior free margin forms the anterior boundary of the hiatus semilunaris inferioris
- Forms the medial wall of the ethmoidal infundibulum
| Superior Attachment of UP | Frontal Sinus Drainage | Comment |
|---|---|---|
| Lamina papyracea (most common - 80%) | Medial to UP, directly into middle meatus; superior infundibulum ends as blind recessus terminalis | A blue probe through HSI cannot enter frontal sinus (Bradoo's probe demonstration, Fig. 3.10) |
| Skull base (fovea ethmoidalis) or middle turbinate (20%) | Lateral to UP, drains into ethmoidal infundibulum | Probe through HSI can access frontal sinus |
2. Ethmoidal Infundibulum
| Wall | Structure |
|---|---|
| Medial | Uncinate process (free posterior edge) |
| Lateral | Lamina papyracea (medial orbital wall) |
| Posterior | Anterior wall of bulla ethmoidalis |
| Anterosuperior | Frontal process of maxilla |
| Superolateral | Lacrimal bone |
- Maxillary sinus ostium - opens into its inferior aspect; drains maxillary sinus
- Anterior ethmoid cells - drain into its walls
- Frontal sinus (in 20% where UP attaches to skull base/MT)
3. Hiatus Semilunaris Inferioris (HSI)
Bradoo's specific terminology: "Hiatus Semilunaris Inferioris" (distinguishes it from the HSS above)
- A two-dimensional, crescent-shaped slit/gap (not a three-dimensional space)
- Lies between the posterior free margin of the uncinate process (anteriorly) and the anterior wall of the bulla ethmoidalis (posteriorly)
- Connects the middle meatus medially with the ethmoidal infundibulum laterally
- Secretions from the infundibulum enter the middle meatus through this slit
- The infundibulum is accessed surgically by passing a probe through the HSI
Key distinction (Bradoo): HSI = 2D slit; Infundibulum = 3D space. The HSI is the "door" to the "room" (infundibulum).
4. Bulla Ethmoidalis (2nd Lamella)
- The largest and most constant anterior ethmoid air cell, formed from the 2nd lamella
- Lies posterior to the uncinate process
- Its anterior wall forms the posterior boundary of the hiatus semilunaris inferioris
- Laterally: enclosed by the lamina papyracea
- Superiorly: anterior wall may extend to skull base, or a suprabullar recess may exist above it
5. Hiatus Semilunaris Superioris (HSS)
Bradoo's unique and distinguishing contribution - she describes two hiatus semilunaris openings
- A semilunar cleft above and behind the bulla ethmoidalis, opposite in orientation to the HSI
- The HSI and HSS are thus oriented in opposite directions
- The HSS leads into the Sinus Lateralis of Grunwald, while the HSI leads into the ethmoidal infundibulum
6. Sinus Lateralis of Grunwald (Retrobullar/Suprabullar Space)
Bradoo specifically names and describes this structure, which is often omitted in other texts
- The space above and behind the bulla ethmoidalis
- Opens into the middle meatus by the hiatus semilunaris superioris
| Wall | Structure |
|---|---|
| Roof | Ethmoid fovea (skull base) |
| Floor | Ethmoid bulla |
| Posterior | Ground lamella of middle turbinate |
| Anterior | Opens into the frontal recess |
| Lateral | Lamina papyracea |
| Medial | Middle turbinate |
7. Frontal Recess
- The most anterior and superior part of the anterior ethmoid, connecting the frontal sinus to the middle meatus
- Continuous anteriorly with the sinus lateralis of Grunwald
- Bounded:
- Anteriorly: agger nasi cell
- Posteriorly: anterior wall of ethmoid bulla
- Laterally: lamina papyracea
- Medially: middle turbinate
| Type | Description |
|---|---|
| Type I | Single cell above the agger nasi cell |
| Type II | Two or more cells above the agger nasi cell |
| Type III | Large cell extending well into the frontal sinus, mimicking the frontal sinus itself ("frontal bulla") |
| Type IV | Isolated "loner cell" separately within the frontal sinus |
8. Agger Nasi Cell
- Most anterior ethmoid cell, lying anterior and lateral to the frontal recess
- Forms the anterior boundary of the frontal recess
- When large, narrows the frontal recess and may obstruct frontal sinus drainage
- Important surgical landmark in endoscopic frontal sinus surgery
9. Maxillary Sinus Ostium
- The natural ostium opens into the inferior aspect of the ethmoidal infundibulum
- Located high on the medial wall of the maxillary sinus - a functionally disadvantaged position
- Mucociliary transport (not gravity) drives secretions toward this ostium
- The uncinate process partially covers/shields it medially
- Nasal fontanelles: areas of bony dehiscence in the lateral nasal wall surrounding the ostium:
- Anterior fontanelle: anterior to UP articulation with inferior turbinate
- Posterior fontanelle: posterior to horizontal process of UP (site of accessory ostia in up to 30%)
- Accessory ostia (perforated posterior fontanelle, 20-25%) cause mucus recirculation - secretions from the maxillary sinus re-enter through the accessory ostium, creating a vicious cycle
Drainage Patterns (Bradoo's Fig. 3.13 concept)
| Sinus Group | Drainage Pathway | Final Destination |
|---|---|---|
| Maxillary sinus | Natural ostium → infundibulum → HSI | Middle meatus |
| Bulla ethmoidalis | Into sinus lateralis → HSS | Middle meatus |
| Frontal sinus | Frontal recess → sinus lateralis → HSS (or medial to UP) | Middle meatus |
| Sphenoid sinus | Natural sphenoid ostium → sphenoethmoidal recess | Superior meatus |
Summary of OMU Components (Bradoo's Classification)
- Middle meatus (space)
- Uncinate process
- Ethmoidal infundibulum
- Hiatus semilunaris inferioris (HSI)
- Bulla ethmoidalis
- Hiatus semilunaris superioris (HSS) + Sinus lateralis of Grunwald
- Frontal recess (+ agger nasi, frontal cells)
Radiological Anatomy of OMC (Bradoo - Chapter 5)
- Coronal CT PNS is the standard investigation
- Shows the OMC from anterior to posterior in sequential slices
- Coronal sections: demonstrate uncinate, infundibulum, maxillary ostium, ethmoid bulla, ground lamella, lamina papyracea, middle turbinate
- Axial sections: demonstrate agger nasi, frontal recess, sphenoid sinus, relationships of OMC to orbit
- Mucosal thickening at OMC = key diagnostic criterion for rhinosinusitis
- Lund-Mackay scoring system: includes OMC scoring (0-2)
Anatomical Variations Affecting OMC (Bradoo - Chapter 6)
| Variation | Effect on OMC |
|---|---|
| Concha bullosa | Pneumatized middle turbinate narrows middle meatus/OMC |
| Paradoxical middle turbinate | Lateral convexity obstructs middle meatus |
| Deviated uncinate process | Narrows infundibulum |
| Pneumatized uncinate | Narrows infundibulum |
| Large agger nasi | Narrows frontal recess |
| Haller cell (infraorbital ethmoid cell) | Narrows infundibulum; predisposes to maxillary sinusitis |
| Septal deviation/spur at middle meatus level | Obstructs OMC |
| Frontal cells (Type III/IV) | Obstructs frontal recess |
Clinical Significance - Pathogenesis of Rhinosinusitis
- Mucosal oedema (allergy, viral URI, pollutants) → swelling of uncinate process + middle turbinate mucosa
- HSI narrows → infundibulum blocked → maxillary and frontal ostia functionally obstructed
- Sinus ventilation impaired → O₂ tension falls → ciliary motility impaired
- Secretion stasis → bacterial colonization → acute/chronic rhinosinusitis
- Because maxillary, frontal, and anterior ethmoid sinuses all drain through this single common unit → multisinus disease from one focal obstruction
- This is the anatomical and physiological basis for FESS: restore OMU patency rather than radical sinus obliteration
Surgical Anatomy - FESS Step-by-Step (Bradoo - Chapter 7)
| Step | Procedure | Anatomical Target |
|---|---|---|
| 1 | Uncinectomy | Removes UP; opens infundibulum and HSI |
| 2 | Middle meatal antrostomy | Enlarges natural maxillary ostium |
| 3 | Anterior ethmoidectomy | Removes bulla and anterior ethmoid cells |
| 4 | Frontal recess dissection | Opens frontal drainage; preserves agger nasi |
| 5 | Posterior ethmoidectomy | Crosses ground lamella into posterior ethmoid |
| 6 | Sphenoidotomy | Opens sphenoid natural ostium |
Key Points Summary
| Bradoo-Specific Concept | Details |
|---|---|
| Four lamellae | UP → Bulla → Ground lamella → Superior turbinate |
| Ground lamella | Bradoo's term for basal lamella; divides ant/post ethmoid |
| Two hiatus semilunaris | HSI (to infundibulum) and HSS (to sinus lateralis) |
| Sinus lateralis of Grunwald | Above/behind bulla; opens into frontal recess |
| Frontal cells Type I-IV | Cells migrating into frontal recess from anterior ethmoid |
| Recessus terminalis | Blind pouch when UP attaches to LP; frontal drains medial to UP |
| Mucociliary recirculation | Secretion cycling through accessory ostia; treatment by removing mucosa bridge |
Create a labeled diagram of the four lamellae and OMC structures
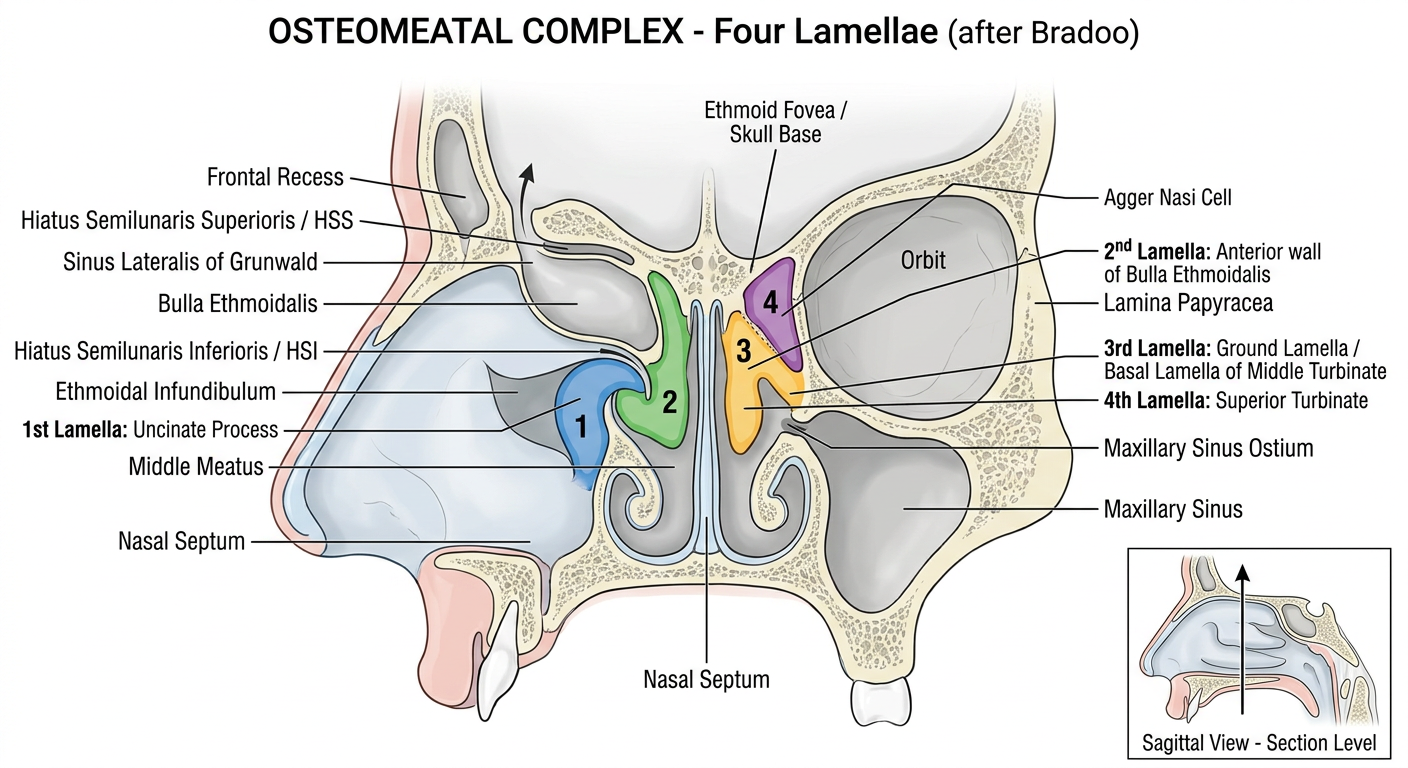
Reading the Diagram
| # | Color | Structure |
|---|---|---|
| 1st | Blue | Uncinate Process |
| 2nd | Green | Anterior wall of Bulla Ethmoidalis |
| 3rd | Yellow/Orange | Ground Lamella of Middle Turbinate |
| 4th | Purple | Superior Turbinate |
- Ethmoidal Infundibulum - the 3D funnel between the uncinate (medially) and lamina papyracea (laterally); drains into middle meatus via HSI
- Hiatus Semilunaris Inferioris (HSI) - 2D crescent slit between free edge of uncinate and anterior wall of bulla; the "door" into the infundibulum
- Hiatus Semilunaris Superioris (HSS) - slit above and behind the bulla; leads into sinus lateralis
- Sinus Lateralis of Grunwald - space above/behind the bulla, bounded by fovea ethmoidalis (roof), bulla (floor), ground lamella (posteriorly), and continuous with the frontal recess anteriorly
- Middle Meatus - the overall space lateral to the middle turbinate within which all OMC structures lie
The ground lamella (3rd lamella) is the surgical watershed - anterior ethmoid cells drain to the middle meatus; posterior ethmoid cells drain to the superior meatus.