Haw to test of Fertility, pregnancy problem
Reading File
Finding Sources
Finding Sources
Searching PubMed
"infertility" AND "diagnosis" AND "evaluation"
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have rich, comprehensive data from authoritative textbooks. Let me compile the complete answer.
Tests for Fertility and Pregnancy Problems
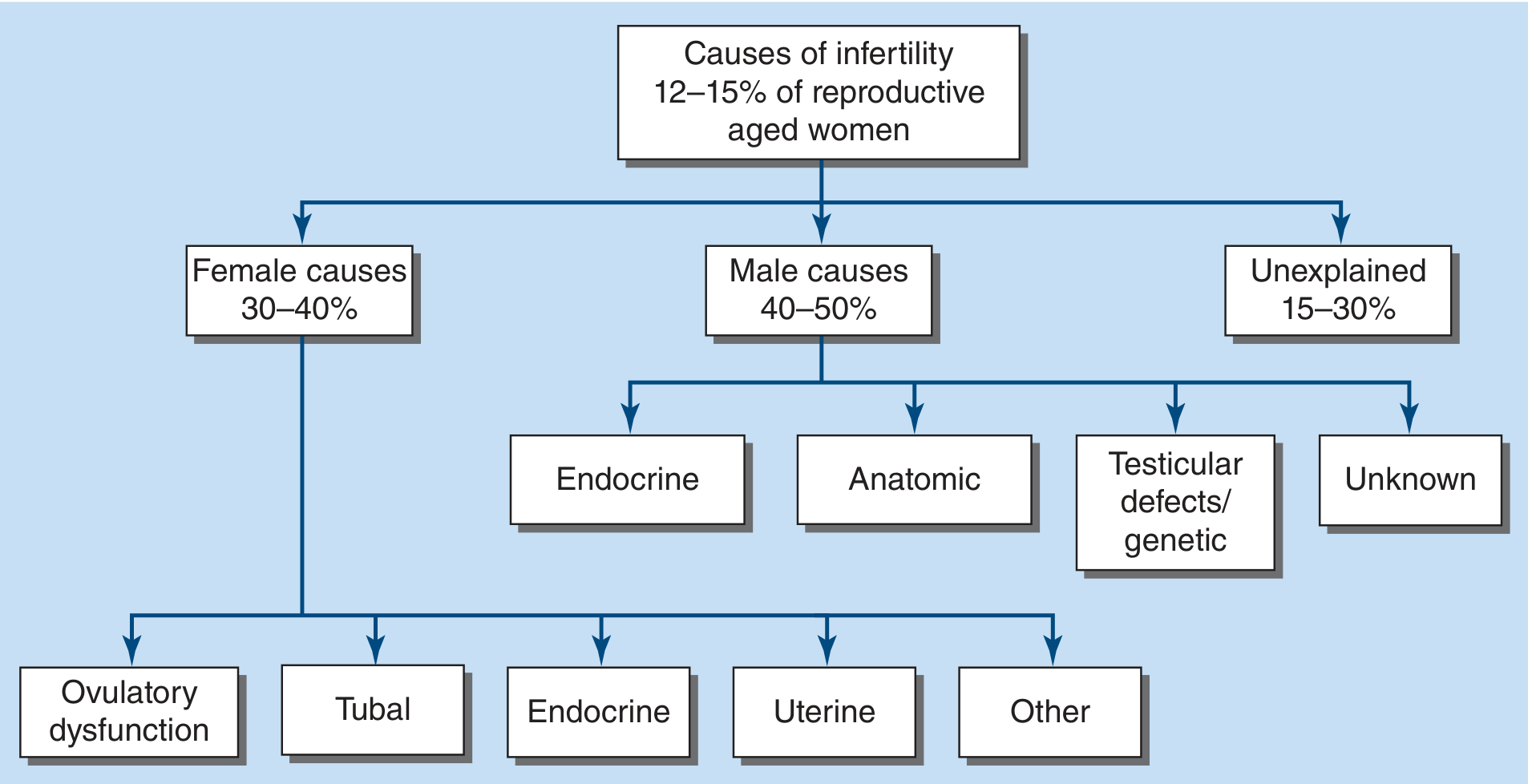
Figure: Causes of infertility - affects 12-15% of reproductive-aged women (Harrison's Principles of Internal Medicine, 22nd Ed.)
What is Infertility?
According to the WHO, infertility is "a disease of the reproductive system defined by the failure to achieve a clinical pregnancy after 12 months or more of regular unprotected sexual intercourse." It affects ~48-72 million couples worldwide (~17.5% globally).
- Primary infertility - couple has never achieved a pregnancy
- Secondary infertility - infertility after at least one prior pregnancy
When to seek evaluation:
- After 12 months of unprotected intercourse (general population)
- After 6 months if the woman is age 35 or older
- Immediately if the woman is age 40 or older, or if known risk factors exist
Causes of Infertility
| Category | Proportion |
|---|---|
| Male factors | 40-50% |
| Female factors | 30-40% |
| Both male + female | 20-30% |
| Unexplained | 15-30% |
In ~1/3 of couples, more than one cause contributes.
Step 1 - History and Physical Exam (Both Partners)
A detailed history from both partners is the starting point.
For the Female Partner:
- Menstrual history (frequency, flow, dysmenorrhea)
- History of sexually transmitted infections (STIs) or pelvic inflammatory disease (PID)
- Prior endometriosis or pelvic surgery
- Exposure to radiation or cytotoxic drugs
- Family history of early menopause
- Thyroid disease, weight changes, signs of hyperandrogenism
- Frequency and timing of intercourse, use of ovulation detection methods
- Physical exam: weight, blood pressure, thyroid, breast, pelvic exam (uterine size, adnexal masses)
For the Male Partner:
- Injuries or surgery to the reproductive tract
- Mumps orchitis, varicocele, undescended testes (cryptorchidism)
- Exposure to radiation, anabolic steroids, cytotoxic drugs
- Smoking, alcohol, recreational drugs (all reduce sperm quality)
- Sexual dysfunction (erectile, ejaculatory problems)
- Physical exam: BMI, blood pressure, complete testicular exam
Step 2 - Testing the Female Partner
A. Ovulation Assessment
| Method | How it Works |
|---|---|
| Urinary LH strips (OPKs) | Detect the LH surge ~24-36 hrs before ovulation; most practical home test |
| Serum progesterone | Measured 7 days after expected ovulation (mid-luteal phase); level >3 ng/mL confirms ovulation |
| Basal body temperature (BBT) | Temperature rises ~0.2-0.5°C in luteal phase after ovulation; less reliable than LH or progesterone |
| Endometrial biopsy | Rarely used now; shows secretory changes confirming ovulation, taken <3 days before menses |
Regular menstrual cycles of 25-35 days generally indicate ovulatory cycles.
B. Ovarian Reserve Evaluation
These tests assess how many eggs remain and egg quality:
| Test | What it Measures | Normal/Notes |
|---|---|---|
| Serum FSH (Day 2 or 3 of cycle) | High FSH = poor reserve (pituitary working harder) | Elevated FSH suggests diminished reserve |
| Serum Estradiol (Day 2 or 3) | Done alongside FSH; high E2 can suppress FSH falsely | |
| Anti-Mullerian Hormone (AMH) | Produced by ovarian follicles; reflects total follicle pool | Can be drawn any day of cycle; declines with age |
| Antral Follicle Count (AFC) by ultrasound | Count of small resting follicles visible on transvaginal ultrasound | Low count = diminished reserve |
These tests help determine urgency of treatment and starting doses for fertility drugs, but do not directly predict pregnancy rates.
C. Endocrine (Hormone) Blood Tests
For women with irregular cycles or suspected hormonal problems:
| Test | Purpose |
|---|---|
| TSH (Thyroid stimulating hormone) | Hypothyroidism is a common, reversible cause of anovulation |
| Prolactin | Hyperprolactinemia suppresses ovulation |
| Total + free testosterone | Elevated in PCOS, congenital adrenal hyperplasia |
| DHEAS, 17-OH progesterone | Screens for adrenal causes of androgen excess |
| Glucose / Insulin | PCOS is strongly associated with insulin resistance |
D. Imaging - Uterus and Tubes
Hysterosalpingography (HSG)
- An X-ray procedure performed on cycle days 7-12
- Radiopaque dye is injected through the cervix, and X-rays show:
- Uterine cavity shape (polyps, fibroids, adhesions, congenital anomalies)
- Fallopian tube openness (patency) and architecture
- Sensitivity 65%, specificity 83% for tubal patency vs. laparoscopy
- Oil-based contrast (vs. water) has shown higher live birth rates (38% vs. 28%) - likely due to flushing effect on tubes
- Premedicate with ibuprofen; risk of PID is 0.3-3.1% (higher with hydrosalpinges)
Sonohysterography (saline infusion sonography / SIS)
- Agitated saline injected via cervix while performing ultrasound
- Good for identifying intrauterine pathology (polyps, adhesions, fibroids)
- No radiation; can be done in a clinic
- Less accurate than HSG for defining tubal architecture
Transvaginal Ultrasound (TVUS)
- Evaluates uterus (fibroids, adenomyosis, mullerian anomalies)
- Assesses ovaries (endometriomas, polycystic-appearing ovaries)
- Counts antral follicles for ovarian reserve
E. Diagnostic Laparoscopy
- Performed under general anesthesia; most invasive but most definitive
- Directly visualizes pelvis for endometriosis, adhesions, tubal disease
- Done with "tubal dye instillation" (chromopertubation) to confirm tube patency
- Indicated if HSG is abnormal, or if all prior tests are normal but pregnancy not achieved (laparoscopy finds unsuspected pathology in 30-50% of such cases)
Step 3 - Testing the Male Partner
A. Semen Analysis (Most Important Male Test)
Collected by masturbation after 2-3 days of abstinence (2-7 days acceptable). Analyzed within 1 hour of collection.
WHO Reference Limits (2010) for a fertile sample:
| Parameter | Lower Reference Limit |
|---|---|
| Semen volume | ≥ 1.5 mL |
| Total sperm number | ≥ 39 million per ejaculate |
| Sperm concentration | ≥ 15 million per mL |
| Total motility | ≥ 40% |
| Progressive motility | ≥ 32% |
| Vitality (live sperm) | ≥ 58% |
| Normal morphology (Kruger strict criteria) | ≥ 4% |
Semen abnormality terminology:
| Term | Meaning |
|---|---|
| Oligozoospermia | Low sperm count (mild-moderate: 5-20 M/mL; severe: <5 M/mL) |
| Asthenozoospermia | Reduced motility |
| Teratozoospermia | Increased abnormal sperm forms |
| Azoospermia | No sperm in ejaculate |
| Necrozoospermia | All sperm dead or non-motile |
| Leucocytospermia | Elevated white cells (infection) |
If abnormal, the test should be repeated after ~6 weeks before concluding male factor infertility, as individual samples vary considerably.
B. Hormone Tests for Men
| Test | Purpose |
|---|---|
| FSH | Low = hypogonadotropic hypogonadism (treatable); high = testicular failure |
| LH | Supports FSH interpretation |
| Total testosterone | Low T can impair spermatogenesis |
| Prolactin | Hyperprolactinemia suppresses gonadotropins |
| TSH | Hypothyroidism affects sperm production |
C. Further Male Investigations (Selected Cases)
Testicular Biopsy - Indicated in azoospermic or severely oligospermic men:
- Fine-needle aspiration (FNA) under local anesthesia, or open biopsy
- Normal biopsy + normal FSH in an azoospermic man = likely obstructive cause (surgically correctable)
- Identifies patterns: hypospermatogenesis, germ cell arrest, Sertoli-cell-only syndrome
- Sperm harvested for ICSI (intracytoplasmic sperm injection)
Y Chromosome Microdeletion Testing - Indicated in:
- Nonobstructive azoospermia or severe oligozoospermia (<5 million/mL)
- PCR of blood DNA for AZFa, AZFb, AZFc regions
- Helps predict likelihood of sperm retrieval and guides genetic counseling
Karyotype / Chromosomal Analysis - For Klinefelter syndrome (47,XXY), other chromosomal anomalies
Scrotal Ultrasound - Identifies varicocele, testicular masses, epididymal cysts
Step 4 - Causes of Pregnancy Loss (Recurrent Miscarriage)
Women with recurrent pregnancy loss (RPL - typically ≥2 losses) undergo additional testing:
| Cause | Test |
|---|---|
| Antiphospholipid syndrome | Lupus anticoagulant, anticardiolipin IgG/IgM, anti-β2 glycoprotein |
| Chromosomal (parental) | Karyotype of both partners |
| Uterine anomalies | HSG, sonohysterography, MRI (septum, bicornuate uterus) |
| Thyroid disease | TSH, thyroid antibodies |
| Thrombophilias | Factor V Leiden, prothrombin gene mutation (controversial for RPL) |
| Male sperm DNA fragmentation | Elevated fragmentation linked to miscarriage (role still being defined) |
| Endometriosis | Possible association with increased miscarriage risk via IVF |
Summary - Quick Reference
BOTH PARTNERS
├── Detailed history and physical exam
├── STI screening (chlamydia, gonorrhea)
FEMALE PARTNER
├── Ovulation: LH urine strips, serum progesterone, BBT
├── Ovarian reserve: AMH, Day-3 FSH + E2, antral follicle count (US)
├── Hormones: TSH, prolactin, androgens
├── Uterus + tubes: Transvaginal ultrasound, HSG or sonohysterography
└── Pelvis (if indicated): Diagnostic laparoscopy
MALE PARTNER
├── Semen analysis x2 (if 1st is abnormal)
├── Hormones: FSH, LH, testosterone, prolactin, TSH
├── Genetics (if severe oligo/azoo): Y microdeletions, karyotype
└── Testicular biopsy (if azoospermic)
Key Points
- Evaluation of both partners simultaneously is recommended from the start, since 20-30% of couples have combined causes
- ~30% of couples have unexplained infertility even after a complete workup
- Fertility declines significantly in women after age 35 - fecundability is reduced 53% at age 40-41 compared to age 30-31
- Some causes (hypothyroidism, hyperprolactinemia, varicocele, tubal obstruction) are treatable and fertility may be restored
- If all basic tests are normal, laparoscopy may reveal occult endometriosis or pelvic adhesions
Sources:
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025), Chapter 408 - Fertility Evaluation
- Goldman-Cecil Medicine, International Ed. - Chapter 218, Infertility Diagnosis
- Berek & Novak's Gynecology - Semen Analysis, HSG, Tubal Assessment
- WHO Semen Analysis Reference Values (2010)
This is a shared conversation. Sign in to Orris to start your own chat.