A 37-year-old primi presented with intermittent per vaginal bleeding at 37 weeks of gestation. On examination, no abdominal tenderness was noted, and she had a blood pressure of 90/60 mmHg and a pulse rate of 110 bpm. What is the next step in the management of this patient? With this also explain the management algorithm for antipartum haemorrhage
Reading File
Finding Sources
Finding Sources
Searching PubMed
"antepartum hemorrhage" AND management
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compose a thorough, well-structured answer.
Clinical Diagnosis & Immediate Next Step
This presentation is classic for Placenta Praevia:
- 37-week primigravida with painless, intermittent per vaginal bleeding
- No abdominal tenderness (contrasting with placental abruption, which causes painful bleeding with a tender, tense uterus)
- Haemodynamic compromise: BP 90/60 mmHg (hypotension) + pulse 110 bpm (tachycardia) — indicating significant blood loss and hypovolaemic shock
⚠️ The Most Critical Rule: DO NOT perform a digital or speculum vaginal examination
The immediate next step is resuscitation + urgent bedside ultrasonography — not a vaginal examination. Performing a digital or speculum exam before confirming placental location by ultrasound can tear marginal placental vessels and precipitate catastrophic, potentially fatal haemorrhage.
Immediate actions (simultaneous):
- Two large-bore IV lines — establish access immediately
- Fluid resuscitation — crystalloids to restore haemodynamic stability
- Urgent bedside ultrasonography — confirm placenta praevia, determine type (complete/partial/low-lying), fetal position, and fetal well-being
- Blood investigations: CBC, coagulation profile (PT, aPTT, fibrinogen, platelet count), type and cross-match
- Continuous fetal heart rate monitoring
- Obstetric consultation — immediate
- Given gestational age of 37 weeks (term): emergency caesarean section is indicated once resuscitation is underway — vaginal delivery is absolutely contraindicated in placenta praevia
If Rh-negative and not yet sensitised: administer 300 µg Rh immunoglobulin within 72 hours.
Complete Placenta Praevia Illustration
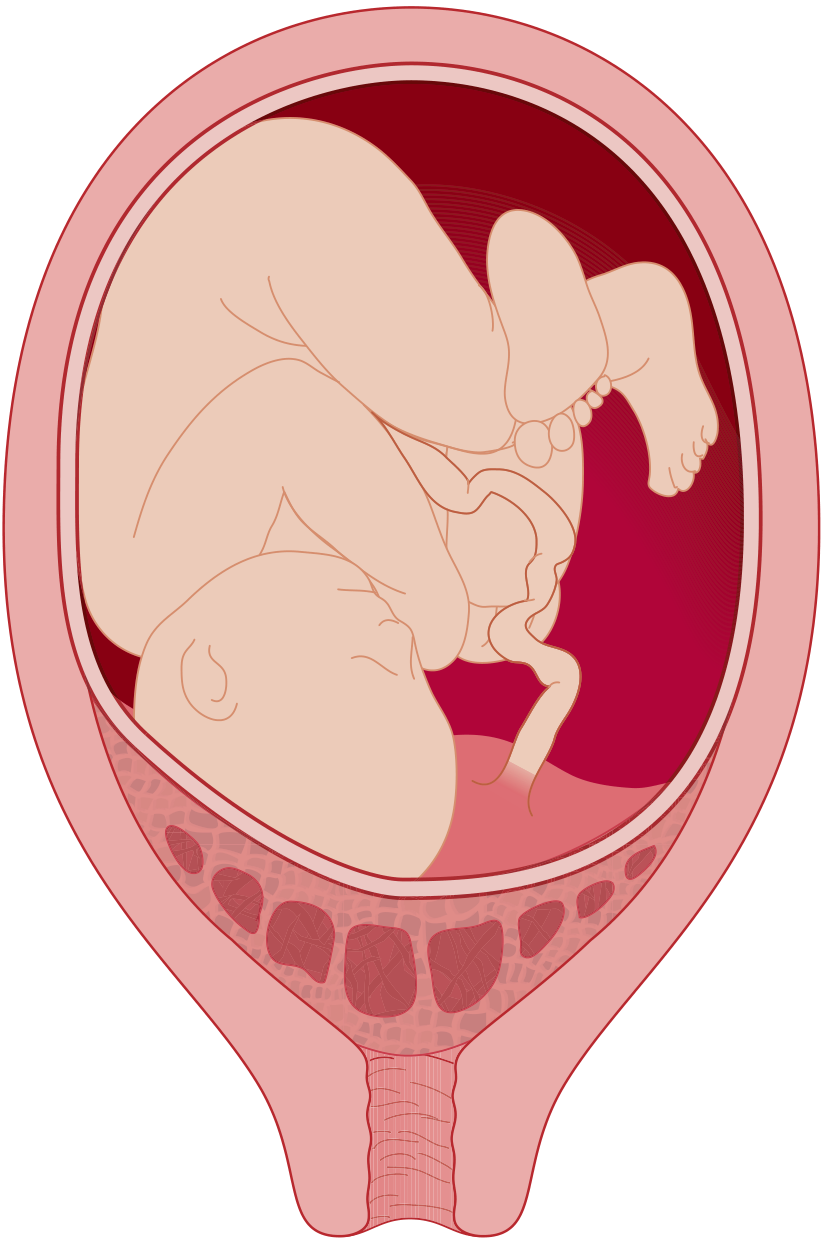
Complete placenta praevia — placenta overlies the internal cervical os (Tintinalli's Emergency Medicine)
Antepartum Haemorrhage (APH): Full Management Algorithm
Definition: Bleeding from the genital tract at or after 24 weeks of gestation, before delivery of the baby.
Incidence: Complicates 3–5% of pregnancies; leading contributor to maternal and perinatal mortality worldwide.
Step 1 — Initial Assessment & Differentiation of Cause
| Feature | Placenta Praevia | Placental Abruption | Other (local/vasa praevia) |
|---|---|---|---|
| Pain | Painless | Painful (uterine tenderness) | Variable |
| Blood colour | Bright red | Dark, clotted | Variable |
| Uterus | Soft, non-tender | Tense, rigid, tender | Soft |
| Fetal lie | Often abnormal (malpresentation) | Usually normal | Normal |
| Haemodynamic shock | Proportionate to visible blood | May be disproportionate (concealed) | Variable |
| Coagulopathy risk | Moderate | High (DIC) | Low |
Rule of thumb: All patients with painless second-trimester or third-trimester vaginal bleeding should be presumed to have placenta praevia until ultrasound proves otherwise.
Step 2 — Initial Resuscitation (All APH)
- Airway, Breathing, Circulation — ABC assessment
- 2 large-bore IV cannulae (16G or larger)
- Fluid resuscitation: warm crystalloids (normal saline / Ringer's lactate)
- Blood transfusion: packed red cells; fresh frozen plasma if fibrinogen <300 mg/dL or coagulopathy present; platelets if <50,000/µL
- Position: left lateral tilt (to relieve aortocaval compression)
- Oxygen by face mask
- Labs: Full blood count, coagulation screen (PT, aPTT, fibrinogen, D-dimer), urea/electrolytes, LFTs, type and cross-match (hold ≥4 units PRBC)
- Continuous fetal monitoring (CTG)
- Foley catheter — monitor urine output
- DO NOT perform digital vaginal examination until placenta praevia is excluded
Step 3 — Diagnostic Imaging
- Transabdominal ultrasound (first-line): localise placenta, assess fetal well-being, estimate blood loss
- Transvaginal ultrasound (TVU): safe and more accurate for defining the relationship between placental edge and internal cervical os; preferred when transabdominal view is suboptimal — TVU will not precipitate haemorrhage when performed carefully
- Empty the bladder before scanning: a full bladder can falsely elongate the lower uterine segment, leading to overdiagnosis of praevia
Step 4 — Subsequent Management by Cause
A. Placenta Praevia
| Clinical Situation | Management |
|---|---|
| <34 weeks, haemodynamically stable, mild bleeding | Admit, bed rest, corticosteroids (betamethasone 12 mg IM ×2 doses 24h apart for lung maturity), IV access maintained, cross-match available |
| 34–36+6 weeks, stable | Expectant management vs. delivery depending on severity; antenatal corticosteroids |
| ≥37 weeks OR severe haemorrhage at any gestation | Emergency caesarean section |
| Haemodynamic instability / active bleeding at any gestation | Immediate caesarean section under general anaesthesia |
- Vaginal delivery is absolutely contraindicated in confirmed placenta praevia
- Warn of risk of uterine atony and placenta accreta spectrum at time of LSCS
- Neuraxial anaesthesia is preferred if haemodynamically stable (less blood loss than GA)
B. Placental Abruption
| Severity | Features | Management |
|---|---|---|
| Grade I (Mild) | <100 mL blood loss, no fetal distress, no coagulopathy | Observation; amniotomy + oxytocin augmentation if in labour |
| Grade II (Moderate) | Fetal distress present, maternal tachycardia | Urgent delivery; CTG monitoring; correct coagulopathy |
| Grade III (Severe) | Maternal shock ± fetal death | Emergency LSCS (if fetus alive); vaginal delivery may be attempted if fetus already dead and mother stable |
- Key: Monitor fibrinogen closely — <150 mg/dL with fetal demise signals severe DIC
- Replace coagulation factors (FFP, cryoprecipitate, platelets) aggressively
- If fetal demise occurs, cautious vaginal delivery is acceptable if mother is haemodynamically stable
C. Vasa Praevia
- Rare but catastrophic: umbilical vessels cross the cervical os; fetal exsanguination occurs rapidly with membrane rupture
- Treatment: immediate operative delivery
Step 5 — Definitive Delivery Decision (Summary)
APH Confirmed
│
├─ Haemodynamically UNSTABLE ──→ Emergency CS (regardless of gestation)
│
└─ Haemodynamically STABLE
│
├─ Gestation < 34 weeks ──→ Expectant management + corticosteroids
│ (unless bleeding worsens)
│
├─ Gestation 34–37 weeks ──→ Individualise (severity, praevia vs. abruption)
│
└─ Gestation ≥ 37 weeks ──→ Deliver
│
├─ Placenta praevia ──→ CAESAREAN SECTION
└─ Abruption (stable) ──→ Vaginal delivery may be considered
Key Points for the Presented Case
| Clinical Feature | Interpretation |
|---|---|
| Painless PV bleeding | Placenta praevia (not abruption) |
| No abdominal tenderness | Supports praevia over abruption |
| BP 90/60, PR 110 | Haemodynamic compromise — significant haemorrhage |
| 37 weeks gestation | Term — delivery is indicated |
| Primigravida | Lower risk for accreta vs. prior CS |
Management in this specific patient: Simultaneously resuscitate (IV fluids, cross-match, correct anaemia) + confirm praevia on ultrasound + proceed to emergency lower-segment caesarean section under neuraxial or general anaesthesia depending on haemodynamic status. Avoid any digital vaginal examination at all times.
Sources: Rosen's Emergency Medicine 10e, p. 3355–3356; Tintinalli's Emergency Medicine 8e, p. 1739–1740; Barash, Cullen & Stoelting's Clinical Anesthesia 9e, p. 3515–3516; Morgan & Mikhail's Clinical Anesthesiology 7e, p. 1639–1640; Creasy & Resnik's Maternal–Fetal Medicine 8e, Chapter 27
Create a clinical management flowchart/poster for antepartum hemorrhage
Reading File
Reading File
Reading File
Running Command
Running Command
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.