# Gross Anatomy of the Abdominal Cavity and Peritoneum: A Comprehensive Guide
---
## PART 1: THE ABDOMINAL CAVITY
### 1.1 Definition and Boundaries
The abdominal cavity is the largest cavity in the body, extending from the thoracic diaphragm superiorly to the pelvic inlet (pelvic brim) inferiorly. It is continuous inferiorly with the pelvic cavity; together they form the **abdominopelvic cavity**.
#### Boundaries:
- **Superior:** Thoracic diaphragm (separates it from the thoracic cavity). The dome of the diaphragm reaches as high as the 5th intercostal space on the right (due to the liver) and the 5th rib on the left. This means a significant portion of the abdominal viscera (liver, spleen, stomach fundus, kidneys) are tucked under the thoracic cage.
- **Anterior:** Anterior abdominal wall muscles (external oblique, internal oblique, transversus abdominis, rectus abdominis) and their aponeuroses.
- **Posterior:** Lumbar vertebrae (L1-L5), posterior abdominal wall muscles (psoas major, psoas minor, quadratus lumborum, iliacus, transversus abdominis), thoracolumbar fascia, and the diaphragmatic crura.
- **Lateral:** Lateral parts of the anterior abdominal wall musculature (the three flat muscles).
- **Inferior:** Open into the pelvic cavity through the pelvic inlet (superior pelvic aperture), bounded by the sacral promontory posteriorly, the iliopectineal lines laterally, and the pubic symphysis anteriorly.
> **Clinical Note – Thoracoabdominal Injuries:** Because the diaphragm rises to the level of the 4th-5th intercostal space, penetrating injuries to the lower chest (below the nipple line anteriorly and below the tip of the scapula posteriorly) can injure abdominal organs. A stab wound at the 6th intercostal space in the midclavicular line can lacerate the liver on the right or the spleen on the left, even though the wound appears "thoracic."
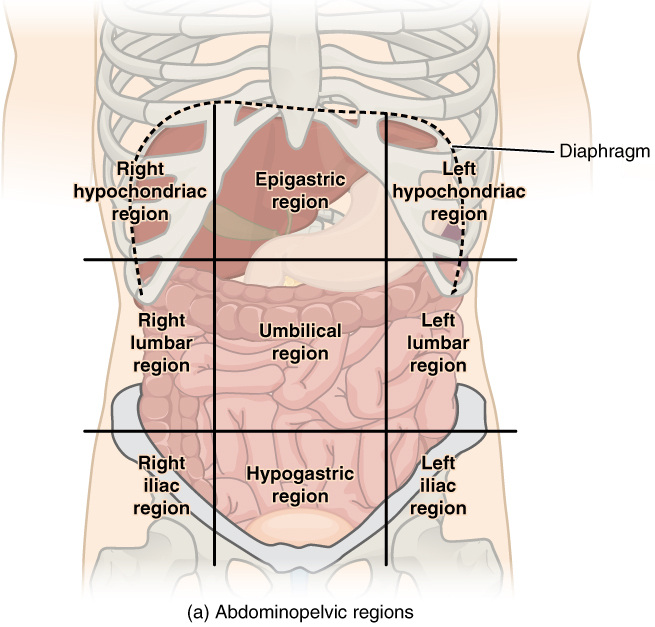
### 1.2 Regions of the Abdomen
The abdomen is divided into regions for clinical description and localization of pain, tenderness, and organs.
#### A. Nine-Region Scheme (Used in Anatomy)
Two vertical lines (midclavicular lines/lateral lines) and two horizontal lines (subcostal plane at L3 and transtubercular/intertubercular plane at L5/iliac tubercles) divide the abdomen into nine regions:
| **Right** | **Midline** | **Left** |
|---|---|---|
| Right Hypochondrium | Epigastrium | Left Hypochondrium |
| Right Lumbar (Flank) | Umbilical | Left Lumbar (Flank) |
| Right Iliac Fossa (Inguinal) | Hypogastrium (Suprapubic) | Left Iliac Fossa (Inguinal) |
**Contents by Region:**
1. **Right Hypochondrium:** Right lobe of liver, gallbladder, right colic (hepatic) flexure, right kidney (upper pole), right suprarenal gland.
2. **Epigastrium:** Left lobe of liver, stomach, duodenum (D1 and D2), pancreas (head and body), aorta, celiac trunk, superior mesenteric artery origin.
3. **Left Hypochondrium:** Fundus of stomach, spleen, tail of pancreas, left colic (splenic) flexure, left kidney (upper pole), left suprarenal gland.
4. **Right Lumbar:** Ascending colon, right kidney (lower pole), right paracolic gutter.
5. **Umbilical:** Transverse colon, loops of jejunum and ileum, omentum, aorta (bifurcation at L4), inferior mesenteric artery origin.
6. **Left Lumbar:** Descending colon, left kidney (lower pole), left paracolic gutter.
7. **Right Iliac Fossa:** Cecum, appendix, terminal ileum, right ureter, right psoas muscle, right ovary and tube (females).
8. **Hypogastrium:** Urinary bladder (when distended), uterus (females), ileum, sigmoid colon.
9. **Left Iliac Fossa:** Sigmoid colon, left ureter, left psoas muscle, left ovary and tube (females).
> **Clinical Note – Pain Localization:**
> - **Appendicitis:** Classically begins as periumbilical pain (visceral pain from midgut, referred to T10 dermatome) and later localizes to the right iliac fossa (parietal peritoneal irritation). **McBurney's point** is located one-third of the way from the anterior superior iliac spine (ASIS) to the umbilicus.
> - **Cholecystitis:** Pain in the right hypochondrium, often radiating to the right shoulder (phrenic nerve, C3-C5 dermatome referral via irritation of the diaphragmatic peritoneum).
> - **Splenic rupture:** Pain in the left hypochondrium, with referred pain to the left shoulder tip (**Kehr's sign**) due to blood irritating the left hemidiaphragm.
> - **Peptic ulcer:** Epigastric pain.
> - **Diverticulitis:** Most commonly left iliac fossa pain (sigmoid colon diverticula most common in Western populations). Sometimes called "left-sided appendicitis."
#### B. Four-Quadrant Scheme (Used Clinically)
A vertical line (median plane) and a horizontal line (transumbilical plane at L3/L4) divide the abdomen into:
- Right Upper Quadrant (RUQ)
- Left Upper Quadrant (LUQ)
- Right Lower Quadrant (RLQ)
- Left Lower Quadrant (LLQ)
### 1.3 Important Planes and Landmarks
- **Transpyloric plane (of Addison):** Midway between the jugular notch and the pubic symphysis, at the level of L1. This plane passes through: pylorus of the stomach, fundus of the gallbladder, neck of pancreas, duodenojejunal flexure, hila of the kidneys, origin of the superior mesenteric artery, attachment of the transverse mesocolon, tips of the 9th costal cartilages, origin of the portal vein.
- **Subcostal plane:** Lower border of the 10th costal cartilage, level of L3. Passes through the origin of the inferior mesenteric artery.
- **Supracristal plane:** At the level of the iliac crests, L4. The aortic bifurcation occurs here.
- **Intertubercular plane:** At the level of the iliac tubercles, L5.
- **Umbilicus:** Level of L3-L4 intervertebral disc (varies with body habitus).
> **Clinical Note – Lumbar Puncture:** The supracristal plane (L4) is used as a landmark for lumbar puncture. A line connecting the highest points of the iliac crests passes through L4 spinous process or L4-L5 interspace. This is below the termination of the spinal cord (conus medullaris at L1-L2) and thus safe for needle insertion.
---
## PART 2: THE PERITONEUM
### 2.1 Definition and Overview
The **peritoneum** is the largest serous membrane in the body (total surface area approximately 1.7-2.0 m², roughly equivalent to body surface area). It consists of a single layer of **mesothelial cells** (simple squamous epithelium) supported by a thin layer of loose connective tissue (submesothelial connective tissue containing blood vessels, lymphatics, nerves, and variable amounts of fat).
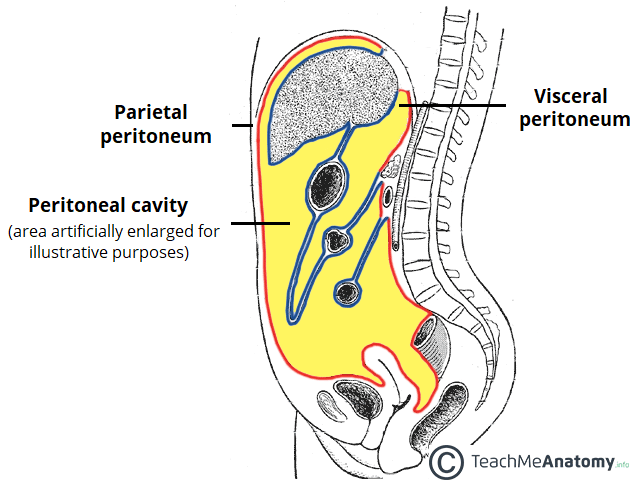
The peritoneum lines the abdominal cavity and covers the abdominal and pelvic viscera to varying degrees. Like all serous membranes (pleura, pericardium), it has two continuous layers:
1. **Parietal peritoneum:** Lines the inner surface of the abdominal and pelvic walls.
2. **Visceral peritoneum:** Covers the abdominal and pelvic organs (viscera).
The **peritoneal cavity** is the potential space between the parietal and visceral layers. Normally, it contains only a thin film (approximately 50-100 mL) of **serous fluid** (peritoneal fluid) that lubricates the surfaces and allows frictionless movement of viscera against each other and against the body wall.
> **Key Point:** The peritoneal cavity is a **closed sac** in males. In females, there is a potential communication with the exterior through the uterine (fallopian) tubes → uterine cavity → vagina. The **ostium of the uterine tube** opens into the peritoneal cavity.
> **Clinical Note – Peritoneal Access in Females:** The opening of the uterine tubes into the peritoneal cavity in females has several clinical implications:
> - **Ectopic pregnancy:** An ovum fertilized at the fimbrial end may implant on the peritoneum or in the tube itself.
> - **Ascending infections:** Pelvic inflammatory disease (PID) caused by *Neisseria gonorrhoeae* or *Chlamydia trachomatis* can spread from the vagina → uterus → tubes → peritoneal cavity, causing **perihepatitis (Fitz-Hugh-Curtis syndrome)** with violin-string adhesions on the liver surface.
> - **Transperitoneal migration of oocytes:** The ovum released from one ovary can theoretically travel through the peritoneal cavity to the contralateral tube.
> - **Hysterosalpingography:** Dye injected into the uterus normally spills into the peritoneal cavity through the tubes, confirming tubal patency (fertility assessment).
### 2.2 Histology and Microanatomy of the Peritoneum
- **Mesothelial layer:** Single layer of flattened mesothelial cells with microvilli on the apical surface. These microvilli increase surface area and help trap a thin layer of peritoneal fluid, reducing friction.
- **Submesothelial connective tissue:** Contains fibroblasts, collagen, elastic fibers, blood vessels, lymphatics, nerves, macrophages, and fat cells (especially in the omentum and mesentery).
- **Stomata (lymphatic openings):** Particularly abundant on the diaphragmatic peritoneum, these are gaps between mesothelial cells that communicate directly with submesothelial lymphatic lacunae. They allow absorption of fluid, particles, bacteria, and cells from the peritoneal cavity into the lymphatic system → thoracic duct → bloodstream.
> **Clinical Note – Peritoneal Absorption:**
> - **Diaphragmatic lymphatic drainage** explains why peritonitis can rapidly lead to bacteremia and sepsis.
> - **Subphrenic abscesses** commonly form because bacteria, inflammatory exudate, and fluid tend to collect in the subphrenic spaces (drawn there by the "suction effect" of respiratory diaphragmatic movements).
> - **Peritoneal dialysis** exploits the large surface area and rich vascularity of the peritoneum for solute and fluid exchange (used in end-stage renal disease).
> - **Intraperitoneal chemotherapy** (HIPEC - Hyperthermic Intraperitoneal Chemotherapy) is used for peritoneal carcinomatosis (e.g., from ovarian or colorectal cancer).
### 2.3 Functions of the Peritoneum
1. **Reduces friction:** Serous fluid acts as a lubricant allowing viscera to glide smoothly.
2. **Resists infection:** Peritoneal macrophages and lymphocytes provide immune surveillance. The omentum ("abdominal policeman") migrates to areas of inflammation and walls off infection.
3. **Stores fat:** Especially in the greater omentum, mesenteries, and extraperitoneal tissue.
4. **Absorption and fluid exchange:** Peritoneal dialysis and drug delivery exploit this function.
5. **Supports viscera:** Mesenteries and ligaments suspend organs and provide pathways for vessels, nerves, and lymphatics.
### 2.4 Parietal Peritoneum
#### Characteristics:
- Lines the inner surface of the abdominal wall, diaphragm, and pelvis.
- **Nerve supply:** Somatic nerves — the same nerves that supply the overlying body wall.
- **Anterior and lateral walls:** Thoracoabdominal nerves (T7-T12) and iliohypogastric/ilioinguinal nerves (L1).
- **Diaphragmatic peritoneum:**
- Central portion: Phrenic nerve (C3, C4, C5) — pain referred to the shoulder tip (C3-C4 dermatome, supraclavicular nerves).
- Peripheral portion: Lower intercostal nerves (T7-T12) — pain localized to the abdominal wall.
- **Pelvic peritoneum:** Obturator nerve (L2-L4) — pain referred to the inner thigh.
- **Pain characteristics:** Sharp, well-localized somatic pain. Patient can point to the exact site of pain. Aggravated by movement, coughing, and deep breathing.
- **Blood supply:** From vessels of the adjacent body wall.
- **Sensitivity:** Exquisitely sensitive to pain, temperature, touch, and pressure.
> **Clinical Note – Signs of Parietal Peritoneal Irritation (Peritonism):**
> - **Guarding:** Voluntary or involuntary contraction of abdominal muscles overlying the inflamed area.
> - **Rigidity ("Board-like rigidity"):** Generalized involuntary contraction of all abdominal muscles, indicating diffuse peritonitis (e.g., perforated duodenal ulcer).
> - **Rebound tenderness (Blumberg's sign):** Pain on sudden release of pressure. Indicates inflammation of the parietal peritoneum.
> - **Percussion tenderness:** Gentle percussion causes pain, also indicating peritoneal irritation.
> - **Cough test:** Asking the patient to cough causes localized pain at the site of parietal peritoneal inflammation (e.g., in appendicitis, pain at McBurney's point on coughing).
> - **Rovsing's sign:** Palpation in the left iliac fossa causes pain in the right iliac fossa (in appendicitis), due to transmission of pressure through the peritoneal cavity.
### 2.5 Visceral Peritoneum
#### Characteristics:
- Covers the viscera (organs) directly.
- **Nerve supply:** Autonomic nerves (sympathetic — mainly via the splanchnic nerves and prevertebral plexuses). The visceral peritoneum is **insensitive to touch, cutting, temperature, and laceration**, but is sensitive to **stretching, distension, chemical irritation (bile, blood, gastric acid), and ischemia**.
- **Pain characteristics:** Dull, poorly localized, crampy, colicky pain. Referred to the midline because of the bilateral autonomic innervation.
- **Foregut structures** (stomach, duodenum D1-D2, liver, gallbladder, pancreas, spleen): Pain referred to the **epigastrium** (T5-T9).
- **Midgut structures** (duodenum D3-D4, jejunum, ileum, cecum, appendix, ascending colon, proximal 2/3 of transverse colon): Pain referred to the **periumbilical region** (T10-T11).
- **Hindgut structures** (distal 1/3 of transverse colon, descending colon, sigmoid colon, rectum upper part): Pain referred to the **suprapubic/hypogastric region** (T11-L2).
- **Blood supply:** From the same vessels that supply the organ it covers.
> **Clinical Note – Visceral Pain Referral:**
> - **Appendicitis evolution:** The classical history of appendicitis involves initial periumbilical pain (visceral, midgut referral) → migration to the right iliac fossa (parietal peritoneal involvement). This migration of pain is pathognomonic and helps differentiate appendicitis from other causes of abdominal pain.
> - **Biliary colic:** Visceral pain from gallbladder distension → referred to the epigastrium. When the gallbladder wall becomes inflamed (cholecystitis) and touches the parietal peritoneum, pain localizes to the right hypochondrium. **Murphy's sign** (arrest of inspiration during palpation of the right hypochondrium) is positive.
> - **Renal colic:** The kidney is retroperitoneal, but the pain of ureteric colic (ureteral stone) can cause peritoneal irritation → flank pain radiating to the groin (following the course of the ureter and the innervation territory of T11-L2).
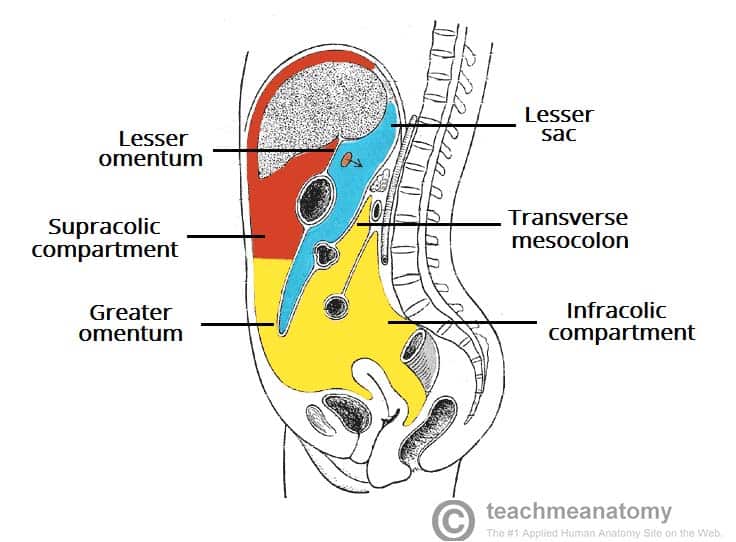
### 2.6 Peritoneal Cavity
The peritoneal cavity is divided into two main compartments by the **transverse mesocolon**:
#### A. Supracolic Compartment
- Above the transverse mesocolon.
- Contains: Stomach, liver, spleen, gallbladder, superior part of duodenum.
- Further subdivided by the liver and its ligaments into right and left subphrenic spaces and right and left subhepatic spaces.
#### B. Infracolic Compartment
- Below the transverse mesocolon.
- Divided into right and left infracolic spaces by the root of the mesentery of the small intestine (runs obliquely from the duodenojejunal flexure at L2 on the left to the ileocecal junction at the right sacroiliac joint).
- Contains: Jejunum, ileum, ascending colon, descending colon, sigmoid colon.
- Communicates with the pelvic cavity inferiorly.
#### C. Pelvic Cavity (Peritoneal component)
- The peritoneum dips into the pelvis, covering the superior surfaces of pelvic organs, creating specific pouches (discussed later).
### 2.7 Classification of Organs by Peritoneal Relationship
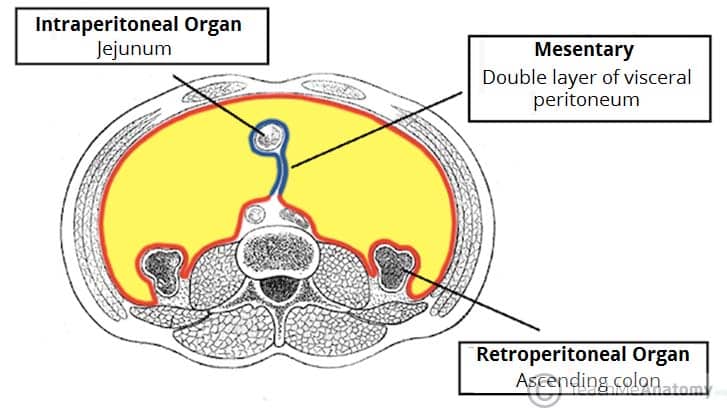
#### A. Intraperitoneal Organs
These organs are (almost) completely covered by visceral peritoneum and are usually suspended by a mesentery or ligament. They are mobile within the peritoneal cavity.
| Organ | Notes |
|---|---|
| Stomach | Completely covered; suspended by greater and lesser omenta |
| First part of duodenum (D1) | Proximal 2-3 cm (duodenal cap); rest is retroperitoneal |
| Jejunum | Suspended by mesentery |
| Ileum | Suspended by mesentery |
| Cecum | Usually intraperitoneal but variable; may have a mesentery |
| Appendix | Has its own mesentery (mesoappendix) |
| Transverse colon | Suspended by transverse mesocolon |
| Sigmoid colon | Suspended by sigmoid mesocolon |
| Liver | Almost completely covered except the bare area |
| Spleen | Completely covered; suspended by lienorenal and gastrosplenic ligaments |
| Ovaries | Intraperitoneal (the only organs that are truly intraperitoneal — the surface epithelium of the ovary is the actual peritoneal surface) |
| Uterine tubes | In the free edge of the broad ligament |
> **Note:** No organ is truly "within" the peritoneal cavity. The term "intraperitoneal" means the organ is wrapped/invaginated by peritoneum, like a fist pushed into a balloon. The organ remains outside the balloon (peritoneal cavity) but is covered by it.
#### B. Retroperitoneal Organs
These organs lie behind the peritoneum, covered by it only on their anterior surface. They are relatively fixed.
**Primary (truly) retroperitoneal** — developed and remained retroperitoneal:
- Kidneys
- Suprarenal (adrenal) glands
- Ureters
- Aorta and inferior vena cava (IVC)
**Secondarily retroperitoneal** — originally intraperitoneal with a mesentery, but became fixed to the posterior abdominal wall during development (mnemonic: **SAD PUCKER**):
- **S** — Second part of duodenum (D2)
- **A** — Ascending colon
- **D** — Descending colon
- **P** — Pancreas (head, neck, body; tail remains intraperitoneal in splenorenal ligament)
- **U** — Upper part not included (some use different mnemonics)
- **C** — (Included in ascending/descending colon)
- **K** — Not kidney (that's primary)
- **E/R** — (Varies by mnemonic)
More commonly, the secondarily retroperitoneal organs are listed as:
- Duodenum (D2, D3, D4)
- Pancreas (head, neck, body)
- Ascending colon
- Descending colon
- Rectum (upper third has peritoneum on front and sides; middle third on front only; lower third has no peritoneum)
> **Clinical Note – Surgical Significance of Peritoneal Relationships:**
> - **Retroperitoneal organs** can be accessed without entering the peritoneal cavity. **Nephrectomy** can be performed through a posterior or flank approach.
> - **Kocher's maneuver:** The secondarily retroperitoneal duodenum (D2) can be mobilized by incising the peritoneum along its lateral border and reflecting it medially along with the head of the pancreas. This is used to access the IVC, right renal vessels, and the posterior aspect of the duodenum (e.g., in duodenal ulcer surgery or trauma).
> - **Mobilization of colon:** During colectomy, the ascending or descending colon can be mobilized by incising the peritoneum at the "white line of Toldt" (the avascular plane where the secondarily retroperitoneal colon fused with the posterior body wall during development).
> - **Retroperitoneal hemorrhage:** Blood from ruptured kidney, aortic aneurysm, or pelvic fracture can accumulate in the retroperitoneal space. Signs include **Grey Turner's sign** (flank ecchymosis) and **Cullen's sign** (periumbilical ecchymosis), although these are late findings. In acute pancreatitis, retroperitoneal fat necrosis and hemorrhage can also produce these signs.
#### C. Subperitoneal (Infraperitoneal) Organs
Organs in the pelvis that lie below the peritoneum:
- Urinary bladder (only the superior surface is covered by peritoneum)
- Lower rectum
- Prostate
- Uterine cervix
### 2.8 Peritoneal Folds, Ligaments, Mesenteries, and Omenta
The peritoneum forms various structures connecting organs to each other and to the body wall:
#### A. Mesenteries
A **mesentery** is a double layer of peritoneum that suspends an organ from the body wall and conveys blood vessels, lymphatics, and nerves to the organ.
##### 1. Mesentery of the Small Intestine (Mesentery Proper)
- **Attachment (Root):** Runs obliquely from the **duodenojejunal flexure** (left of L2) to the **ileocecal junction** (right iliac fossa, right sacroiliac joint). The root is approximately **15 cm long**.
- **Structures crossed by the root:** Left renal vein, third part of duodenum (D3), aorta, IVC, right ureter, right psoas major, right gonadal vessels.
- **Shape:** Fan-shaped; the intestinal border is approximately **6 meters long** (the length of the small intestine), creating extensive ruffling.
- **Contents:** Superior mesenteric artery and its branches (intestinal arteries, jejunal and ileal branches), superior mesenteric vein and its tributaries, mesenteric lymph nodes (400-500), autonomic nerves (superior mesenteric plexus), fat.
- **Height:** Approximately 20 cm at its maximum.
> **Clinical Note:**
> - **Mesenteric ischemia:** Occlusion of the superior mesenteric artery (SMA) by embolism (usually from atrial fibrillation) or thrombosis leads to acute mesenteric ischemia — catastrophic infarction of the midgut. Presents with severe periumbilical pain "out of proportion to physical findings" in the early stages. Mortality is very high (60-80%) if not treated within 6 hours.
> - **Internal hernias:** Defects in the mesentery can trap bowel loops, causing internal herniation and strangulation. This is an important complication after Roux-en-Y gastric bypass surgery, where mesenteric defects are created.
> - **Mesenteric cysts:** Cystic lymphangiomas or other cysts can occur within the mesentery.
> - **Mesenteric lymphadenitis:** Inflammation of mesenteric lymph nodes (often caused by *Yersinia enterocolitica* in children) can mimic appendicitis. Distinguished by pain that shifts with position (mesenteric nodes are mobile) — **Klein's sign**.
##### 2. Transverse Mesocolon
- Suspends the transverse colon from the posterior abdominal wall.
- **Attachment (Root):** Along the anterior surface of the pancreas (head, neck, body) and the anterior surface of the left kidney. Runs from the right colic (hepatic) flexure to the left colic (splenic) flexure.
- **Contents:** Middle colic artery (branch of SMA), middle colic vein, lymph nodes, autonomic nerves.
- **Significance:** Divides the peritoneal cavity into supracolic and infracolic compartments. Its root crosses the descending part of the duodenum (D2) and the head of the pancreas.
> **Clinical Note:**
> - **Transverse mesocolon as a barrier:** In acute pancreatitis, inflammatory exudate from the pancreas (which lies behind the transverse mesocolon attachment) can spread along the transverse mesocolon, causing thrombosis of the middle colic vessels and potentially colonic ischemia.
> - **Surgical access:** The transverse mesocolon provides a route for the surgeon to access the lesser sac (omental bursa) from below.
##### 3. Sigmoid Mesocolon
- Suspends the sigmoid colon from the posterior pelvic wall.
- **Attachment (Root):** Has an **inverted V-shape** (or lambda Λ shape). The apex of the V is near the bifurcation of the left common iliac artery, overlying the left ureter. The left limb descends along the medial border of the left psoas, and the right limb descends into the pelvis along the rectum.
- **Contents:** Sigmoid arteries and veins (branches of inferior mesenteric artery/vein), lymph nodes, autonomic nerves.
- The left ureter passes behind the apex of the sigmoid mesocolon.
> **Clinical Note:**
> - **Sigmoid volvulus:** The sigmoid colon, being mobile on its mesentery, is the most common site of colonic volvulus. Occurs when the sigmoid twists on its mesentery → obstruction and ischemia. Common in elderly, institutionalized patients, and those with chronic constipation and a redundant sigmoid colon. Also very common in Africa and South America ("sigmoid volvulus belt"). Diagnosed by the characteristic **"coffee bean sign"** or **"omega loop sign"** on abdominal X-ray. Initially managed with **flexible sigmoidoscopic decompression** (with a rectal tube), but recurrence is common, often requiring **sigmoid colectomy**.
> - **Ureter at risk during surgery:** The left ureter's relationship to the apex of the sigmoid mesocolon makes it vulnerable during sigmoid colon surgery.
##### 4. Mesoappendix
- Suspends the appendix from the lower surface of the mesentery of the ileum (near the ileocecal junction).
- **Shape:** Triangular fold.
- **Contents:** Appendicular artery (a branch of the ileocolic artery — specifically from the posterior cecal artery; it is an **end artery**), appendicular vein, lymphatics.
> **Clinical Note:**
> - **Appendicular artery as end artery:** Because the appendicular artery is a true end artery (no collateral supply), its thrombosis in appendicitis leads to **gangrenous appendicitis** and subsequent **perforation**. This is why appendicitis must be treated surgically (or with antibiotics in early, uncomplicated cases) before gangrene develops.
> - During **appendectomy**, the mesoappendix is ligated and divided first, and then the base of the appendix is ligated and divided.
#### B. Omenta
An **omentum** is a double-layered fold of peritoneum extending from the stomach and proximal duodenum to adjacent organs.
##### 1. Greater Omentum
- The largest peritoneal fold; hangs like an **"apron"** from the greater curvature of the stomach and the first part of the duodenum.
- **Layers:** Actually consists of **four layers** of peritoneum (two layers descend from the greater curvature, turn back on themselves, and two layers ascend to fuse with the transverse mesocolon). In adults, these four layers are usually fused.
- **Extent:** Hangs down from the greater curvature of the stomach over the transverse colon and coils of small intestine, reaches to varying levels (sometimes as far as the pelvis), then folds back up to attach to the transverse colon.
- **Attachments:**
- **Superior:** Greater curvature of the stomach and first part of the duodenum.
- **Inferior:** Free edge (variable length).
- **Posterior:** Fuses with the anterior surface of the transverse colon and transverse mesocolon.
- **Contents:** Variable amounts of fat (can be very large in obese individuals), right and left gastroepiploic (gastro-omental) vessels along the greater curvature, lymph nodes (**omental lymph nodes**), macrophages, and lymphoid aggregates ("milky spots").
- **The Greater Omentum as the "Abdominal Policeman" (or "Guardian of the Peritoneal Cavity"):** The omentum has remarkable ability to migrate toward sites of inflammation. It contains abundant macrophages in specialized structures called **"milky spots"** (aggregates of macrophages, lymphocytes, and mesothelial cells). When there is intra-abdominal inflammation, the omentum adheres to the inflamed area, walls off infection, promotes angiogenesis, and delivers immune cells.
> **Clinical Note – Greater Omentum:**
> - **Walling off infections:** In appendicitis, the omentum frequently wraps around the inflamed appendix, limiting peritoneal contamination and forming a **peri-appendiceal abscess** or "appendicular mass." This is why generalized peritonitis from a perforated appendix is less common than might be expected.
> - **Omental infarction:** Torsion of the omentum or thrombosis of omental vessels can cause omental infarction, presenting as acute abdominal pain (often mimicking appendicitis or cholecystitis).
> - **Omental herniation:** The omentum can herniate through inguinal, femoral, or umbilical hernial defects ("omentocele").
> - **Omental patch (Graham patch):** In the repair of a perforated peptic ulcer, a pedicle of omentum may be used to plug the perforation (omentopexy).
> - **Omental cake:** In advanced ovarian cancer (and other peritoneal carcinomatoses), the omentum becomes infiltrated with tumor and becomes thickened and hardened — described as "omental cake" on imaging.
> - **Omental flaps:** In reconstructive surgery, omental flaps (pedicled on the gastroepiploic vessels) are used for reconstruction of chest wall defects, coverage of vascular grafts, and treatment of mediastinitis after cardiac surgery.
##### 2. Lesser Omentum
- Connects the lesser curvature of the stomach and the first part of the duodenum to the liver (porta hepatis and fissure for ligamentum venosum).
- **Two parts:**
1. **Hepatogastric ligament:** From the lesser curvature of the stomach to the fissure for ligamentum venosum on the visceral surface of the liver. This is thin and translucent (can be perforated to access the lesser sac).
2. **Hepatoduodenal ligament:** From the first part of the duodenum to the porta hepatis. This is thick and contains important structures forming the **portal triad** (hepatic triad).
- **Contents of the Hepatoduodenal Ligament (Portal Triad):**
- **Bile duct (common bile duct/CBD):** Anteriorly and to the right.
- **Hepatic artery proper:** Anteriorly and to the left.
- **Portal vein:** Posteriorly and between the other two.
- Also contains: hepatic plexus of nerves, hepatic lymph nodes, hepatic lymphatic vessels.
- **Mnemonic for arrangement:** (from right to left anteriorly) **D**uct, **A**rtery, **V**ein = **DAV** (or from anterior to posterior at the free edge: **"VAN" going posteriorly** — but more commonly remembered as the bile duct is most anterior and right, artery is anterior and left, vein is posterior).
> **Clinical Note – Pringle Maneuver:**
> - The hepatoduodenal ligament forms the **anterior border of the epiploic foramen (foramen of Winslow)**. The free right edge of the lesser omentum can be compressed between the thumb and index finger (**Pringle maneuver**) to temporarily occlude the hepatic artery and portal vein, thereby controlling hemorrhage from the liver. If bleeding stops with Pringle maneuver, the source is hepatic artery or portal vein. If bleeding continues, the source is hepatic veins or IVC (retrohepatic).
> - **Maximum safe occlusion time:** Intermittent clamping (15-20 minutes of clamping alternating with 5 minutes of unclamping) is used to minimize ischemic injury to the liver. Continuous clamping for up to 60 minutes has been tolerated in normothermic conditions.
- **Contents of the Hepatogastric Ligament:**
- Left and right gastric arteries (along the lesser curvature of the stomach)
- Left and right gastric veins
- Gastric lymph nodes
- **Aberrant/accessory left hepatic artery** (replaced left hepatic artery from the left gastric artery — present in ~25% of the population). This is a crucial variant.
> **Clinical Note:**
> - **Replaced left hepatic artery:** In approximately 25% of individuals, the left hepatic artery arises from the left gastric artery and courses through the hepatogastric ligament to reach the liver. Division of the hepatogastric ligament (e.g., during gastrectomy or fundoplication) without recognizing this variant can lead to devascularization of the left lobe of the liver and hepatic ischemia/necrosis.
> - During **upper GI endoscopy**, the lesser omentum is visible endoscopically, and its appearance may be relevant in staging gastric cancer (involvement suggests advanced disease).
##### 3. Gastrosplenic Ligament (Gastrolienal Ligament)
- Connects the greater curvature of the stomach (fundus and upper body) to the hilum of the spleen.
- **Contents:** Short gastric arteries and veins (branches of the splenic artery/vein), left gastroepiploic (gastro-omental) vessels (proximal portion).
- Embryologically, it is part of the greater omentum (dorsal mesogastrium).
##### 4. Splenorenal Ligament (Lienorenal Ligament)
- Connects the hilum of the spleen to the left kidney.
- **Contents:** Splenic artery (distal portion/tail), splenic vein, tail of the pancreas, left gastroepiploic vessels (origin).
- Embryologically derived from the dorsal mesogastrium.
> **Clinical Note:**
> - During **splenectomy**, the splenorenal and gastrosplenic ligaments must be carefully divided. The tail of the pancreas, which extends into the splenorenal ligament to the splenic hilum, is at risk of injury during splenectomy, potentially leading to **pancreatitis or pancreatic fistula**.
> - **Short gastric vessel ligation:** During splenectomy, the short gastric vessels in the gastrosplenic ligament must be carefully ligated. Failure can cause gastric ischemia of the fundus (though collateral supply usually prevents this) or hemorrhage.
#### C. Peritoneal Ligaments
Peritoneal ligaments are double layers of peritoneum connecting organs to each other or to the abdominal wall. Unlike mesenteries, they are not always associated with the gastrointestinal tract.
##### 1. Falciform Ligament
- Connects the liver to the anterior abdominal wall and the diaphragm.
- Contains the **ligamentum teres hepatis (round ligament of the liver)** in its free inferior edge — the obliterated remnant of the left umbilical vein.
- Contains small **paraumbilical veins** (veins of Sappey) that connect the portal venous system (left branch of the portal vein) to the systemic venous system (superficial epigastric veins in the abdominal wall).
- The falciform ligament divides the liver surface into anatomical right and left lobes (not the true surgical/functional right and left lobes, which are divided by Cantlie's line — a line from the gallbladder fossa to the IVC).
> **Clinical Note – Portal Hypertension and Caput Medusae:**
> - In portal hypertension (e.g., cirrhosis), blood cannot flow normally through the liver. The paraumbilical veins in the falciform ligament become dilated (**recanalization of the umbilical vein**) and serve as a portosystemic anastomosis (portal → paraumbilical veins → superficial epigastric veins). This produces dilated, tortuous veins radiating from the umbilicus — **caput medusae** (named after the snake-haired Gorgon of Greek mythology). The flow pattern can be determined by the Trendelenburg test: in portal hypertension, flow is away from the umbilicus in all directions.
> - A **Cruveilhier-Baumgarten syndrome** refers to portal hypertension with patent paraumbilical veins and a venous hum/thrill at the umbilicus.
##### 2. Coronary Ligament
- Reflections of peritoneum from the diaphragm to the liver.
- Consists of anterior (upper) and posterior (lower) layers that enclose the **bare area of the liver** (area not covered by peritoneum).
- The two layers converge laterally to form the right and left **triangular ligaments**.
##### 3. Triangular Ligaments
- **Right triangular ligament:** Formed by convergence of the right ends of the coronary ligament layers. Short.
- **Left triangular ligament:** Formed by convergence of the left ends of the coronary ligament layers. Long. Contains the **left hepatic vein** near its attachment to the liver. Also contains the obliterated **ligamentum venosum** (remnant of ductus venosus) nearby.
> **Clinical Note:**
> - The bare area of the liver (between the layers of the coronary ligament) is in direct contact with the diaphragm and right adrenal gland. This means:
> - **Amoebic liver abscess** in the right lobe can rupture through the diaphragm into the right pleural cavity (right-sided pleural effusion or empyema) or even into the right lung (forming a hepatobronchial fistula — patient coughs "anchovy sauce" sputum).
> - **Hepatic bleeding** from the bare area can track into the retroperitoneum.
> - During **liver surgery (hepatectomy)**, the triangular and coronary ligaments must be divided to mobilize the liver. Division of the left triangular ligament must be done carefully to avoid injury to the left hepatic vein and left inferior phrenic vein.
##### 4. Hepatorenal Ligament
- A portion of the coronary ligament that extends from the posterior layer to the right kidney, forming the boundary of the hepatorenal recess (pouch of Morison).
##### 5. Gastrophrenic Ligament
- Connects the fundus of the stomach to the diaphragm. Contains the left inferior phrenic artery branches.
##### 6. Phrenicocolic Ligament
- Connects the left colic (splenic) flexure to the diaphragm at the level of the 11th rib.
- Forms a "shelf" that supports the spleen ("sustentaculum lienis").
- Limits communication between the left paracolic gutter and the left subphrenic space.
> **Clinical Note:**
> - The phrenicocolic ligament partially limits the spread of infected fluid from the left paracolic gutter to the left subphrenic space. However, fluid can still reach the left subphrenic space from the right side via the supracolic route.
##### 7. Broad Ligament of the Uterus
- A double layer of peritoneum extending from the sides of the uterus to the lateral pelvic wall and floor.
- **Subdivisions:**
- **Mesometrium:** The largest part; below the uterine tube and around the uterus. Contains the uterine artery and veins.
- **Mesosalpinx:** Between the uterine tube and the ovary/mesovarium. Contains the uterine tube, ovarian vessels (tubal branches), epoophoron, and paroophoron remnants.
- **Mesovarium:** Posterior extension connecting the ovary to the broad ligament. The ovary is attached by the mesovarium but projects posteriorly and is NOT covered by peritoneum on its surface (covered by germinal epithelium instead).
- **Contents:** Uterine tubes, round ligament of the uterus, ovarian ligament, uterine artery and veins, ovarian vessels, ureters (pass through the base), parametrial tissue.
> **Clinical Note:**
> - **Ureter during hysterectomy:** The ureter passes through the base of the broad ligament, approximately 2 cm lateral to the cervix. It is crossed superiorly by the uterine artery ("water under the bridge" — ureter = water, uterine artery = bridge). This relationship makes the ureter vulnerable to injury during hysterectomy. Ureteral injury is one of the most dreaded complications of pelvic surgery.
> - **Broad ligament hematoma:** Trauma to the uterine or ovarian vessels can cause a hematoma that dissects within the layers of the broad ligament (broad ligament hematoma), which can be massive.
#### D. Peritoneal Folds and Fossae
##### 1. On the Internal Surface of the Anterior Abdominal Wall (Below the Umbilicus)
Five peritoneal folds (ridges) radiate from the umbilicus toward the pelvis:
| Fold | Contents | Position |
|---|---|---|
| **Median umbilical fold** (1, unpaired) | Median umbilical ligament (obliterated urachus — remnant of the allantois) | Midline |
| **Medial umbilical folds** (2, paired) | Medial umbilical ligaments (obliterated umbilical arteries) | Medial to lateral |
| **Lateral umbilical folds** (2, paired) | Inferior epigastric vessels | Lateral |
Between these folds, there are peritoneal fossae (depressions):
| Fossa | Location | Clinical Significance |
|---|---|---|
| **Supravesical fossa** | Between median and medial umbilical folds | Rare site of supravesical hernia |
| **Medial inguinal fossa** | Between medial and lateral umbilical folds | Corresponds to the **superficial inguinal ring** / **Hesselbach's triangle** — site of **direct inguinal hernia** |
| **Lateral inguinal fossa** | Lateral to the lateral umbilical fold | Corresponds to the **deep inguinal ring** — site of **indirect inguinal hernia** |
> **Clinical Note – Inguinal Hernias:**
> - **Direct inguinal hernia:** Passes through the medial inguinal fossa (Hesselbach's triangle), through the posterior wall of the inguinal canal. Does NOT pass through the deep ring. Lies **medial** to the inferior epigastric vessels. Usually acquired, in older men, due to weakness of the transversalis fascia. Covered by peritoneum and transversalis fascia. Rarely strangulates.
> - **Indirect inguinal hernia:** Passes through the lateral inguinal fossa and the deep inguinal ring, traversing the entire inguinal canal, and may emerge through the superficial inguinal ring into the scrotum. Lies **lateral** to the inferior epigastric vessels. The hernia sac is a persistent processus vaginalis. More common overall, especially in young males. Higher risk of strangulation.
> - **Laparoscopic view:** During laparoscopic hernia repair (TEP or TAPP), the surgeon views the internal surface of the anterior abdominal wall from within the peritoneal cavity and can clearly see the five folds, the fossae, and the hernia defects. This is the most relevant clinical anatomy of these folds.
##### 2. Ileocecal Folds and Fossae
- **Superior ileocecal fold (vascular fold):** Contains the anterior cecal artery (branch of the ileocolic artery). Extends from the ileum to the cecum.
- **Inferior ileocecal fold (bloodless fold of Treves):** An avascular fold from the ileum to the mesoappendix/cecum.
- **Ileocecal recess (superior ileocecal recess):** Between the superior ileocecal fold and the mesentery.
- **Retrocecal recess:** Behind the cecum (site where the retrocecal appendix lies — most common position of the appendix, ~65%).
> **Clinical Note:**
> - The **retrocecal position** of the appendix means that in retrocecal appendicitis, the anterior abdominal wall signs (guarding, rigidity, rebound tenderness) may be **diminished or absent** because the inflamed appendix is shielded from the parietal peritoneum by the cecum. Instead, the patient may have:
> - Flank pain (posterior parietal peritoneum irritation)
> - Positive **psoas sign** (pain on extension of the right hip — appendix irritating the psoas muscle)
> - Right loin tenderness
> - A **pelvic appendix** may cause:
> - Suprapubic pain
> - Diarrhea or urinary frequency (irritation of rectum or bladder)
> - Positive **obturator sign** (pain on internal rotation of the flexed right hip — appendix irritating the obturator internus muscle)
> - Tenderness on digital rectal examination
##### 3. Paraduodenal Fossae
- Located near the duodenojejunal flexure (ligament of Treitz).
- **Superior duodenal fossa** (fossa of Landzert): Above the superior duodenal fold. Contains the inferior mesenteric vein.
- **Inferior duodenal fossa** (fossa of Jonnesco): Below the inferior duodenal fold.
- **Paraduodenal fossa** (fossa of Landzert, larger): Contains the inferior mesenteric vein and ascending branch of the left colic artery.
- These are potential sites of **internal hernias (paraduodenal hernias)**, which are the most common type of internal hernia (~53% of all internal hernias). They can cause intestinal obstruction.
##### 4. Intersigmoid Recess
- Located behind the apex of the sigmoid mesocolon, at the point where it reflects from the posterior pelvic wall.
- The left ureter passes behind this recess.
- A potential site for internal herniation (intersigmoid hernia).
### 2.9 Peritoneal Spaces and Recesses (Detailed)
The peritoneal cavity has several important spaces and recesses that are clinically significant as sites of fluid collection, abscess formation, and tumor spread.
#### A. Supracolic Spaces
##### 1. Subphrenic Spaces (Subdiaphragmatic Spaces)
**(a) Right Subphrenic Space (Right Anterior Superior Space):**
- Between the diaphragm (above) and the right lobe of the liver (below).
- Divided by the falciform ligament into right and left subphrenic spaces.
- Bounded posteriorly by the anterior layer of the coronary ligament.
- Communicates with the right subhepatic space (including the hepatorenal recess) laterally, and with the right paracolic gutter.
**(b) Left Subphrenic Space (Left Anterior Superior Space):**
- Between the diaphragm (above) and the left lobe of the liver and the anterior surface of the stomach (below).
- Divided from the left posterior subphrenic space (perisplenic/perihepatic space) by the left triangular ligament.
- Communicates with the left paracolic gutter.
**(c) Left Posterior Subphrenic Space (Perisplenic Space):**
- Between the spleen, left kidney, and left colic flexure, bounded by the phrenicocolic ligament inferiorly.
- This is essentially the space around the spleen.
> **Clinical Note – Subphrenic Abscess:**
> - Subphrenic abscesses occur most commonly after:
> - Perforated peptic ulcer
> - Ruptured appendix with generalized peritonitis
> - Post-operative complications (especially after gastric, biliary, or splenic surgery)
> - Liver abscess rupture
> - **Right subphrenic abscess** is the most common (accounts for ~60% of subphrenic abscesses), often secondary to perforated duodenal ulcer, cholecystitis, or appendicitis.
> - **Symptoms:** Fever (swinging/spiking), malaise, hiccups (diaphragmatic irritation of phrenic nerve), shoulder tip pain (referred via C3-C5), pleuritic chest pain.
> - **Diagnosis:** CT scan with contrast (most accurate). Chest X-ray may show elevated hemidiaphragm, pleural effusion, and gas under the diaphragm.
> - **Treatment:** Percutaneous CT/US-guided drainage + antibiotics. Surgical drainage if percutaneous approach fails.
##### 2. Subhepatic Spaces
**(a) Right Anterior Subhepatic Space:**
- Between the visceral surface of the right lobe of the liver and the transverse colon/duodenum/gallbladder.
**(b) Hepatorenal Recess (Pouch of Morison / Right Posterior Subhepatic Space):**
- The **deepest part of the supracolic peritoneal cavity** in the **supine position**.
- Located between the posterior surface of the right lobe of the liver (anteriorly) and the right kidney and right adrenal gland (posteriorly).
- **Boundaries:**
- Superior: Posterior layer of the coronary ligament
- Inferior: Transverse mesocolon and hepatic flexure of colon
- Medial: Duodenum (D2) and epiploic foramen (of Winslow)
- Lateral: Right paracolic gutter
- **Significance:** Being the most dependent part of the supracolic compartment in a supine patient, **free intraperitoneal fluid** (blood, bile, pus, ascites) gravitates here first.
> **Clinical Note – Hepatorenal Recess (Morison's Pouch):**
> - **FAST exam (Focused Assessment with Sonography for Trauma):** The hepatorenal recess is one of the four areas examined during a FAST ultrasound in trauma. The presence of anechoic (dark) fluid in Morison's pouch indicates **hemoperitoneum** and may necessitate emergent laparotomy. As little as **200 mL** of free fluid can be detected in Morison's pouch by ultrasound.
> - FAST also examines: splenorenal recess, suprapubic (pouch of Douglas/rectovesical pouch), and pericardium.
> - **Diagnostic peritoneal lavage (DPL):** Now largely replaced by FAST and CT scan, but may still be used. A catheter is placed into the peritoneal cavity (infraumbilical, supraumbilical if pelvic fracture) and lavage fluid is instilled and aspirated. Positive if: >100,000 RBCs/mm³, >500 WBCs/mm³, presence of bile/bacteria/food particles.
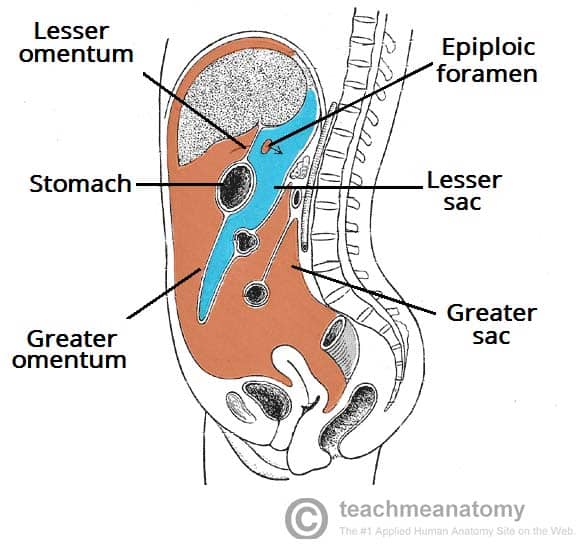
##### 3. Lesser Sac (Omental Bursa)
This is a large, complex peritoneal recess located **behind the stomach and lesser omentum** and **in front of the pancreas**. It is the largest peritoneal recess.
**Boundaries:**
- **Anterior:** Lesser omentum (hepatogastric and hepatoduodenal ligaments), posterior wall of the stomach, anterior two layers of the greater omentum.
- **Posterior:** Peritoneum over the pancreas, left kidney, left adrenal gland, splenic artery, diaphragm (left crus), aorta.
- **Superior:** Caudate lobe of the liver, diaphragm.
- **Inferior:** Posterior two layers of the greater omentum fused with the transverse mesocolon.
- **Left:** Gastrosplenic ligament, splenorenal ligament, hilum of the spleen.
- **Right:** Epiploic foramen (the only communication with the greater sac).
**Subdivisions:**
1. **Superior recess:** Behind the caudate lobe of the liver, extending to the diaphragm.
2. **Inferior recess:** Between the layers of the greater omentum (usually obliterated in adults by fusion of the layers).
3. **Splenic recess:** Extends to the left toward the hilum of the spleen.
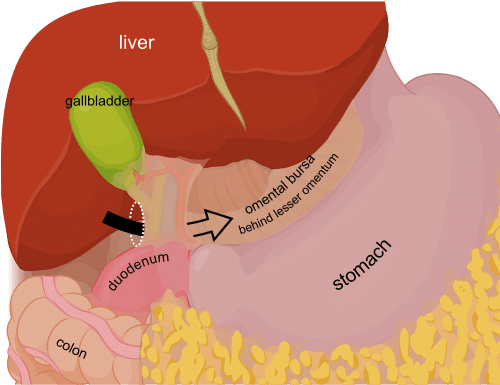
**Epiploic Foramen (Foramen of Winslow / Aditus to the Lesser Sac):**
This is the only natural communication between the **greater sac (main peritoneal cavity)** and the **lesser sac (omental bursa)**.
**Boundaries:**
- **Anterior:** Free edge of the lesser omentum (hepatoduodenal ligament containing the portal triad — CBD, hepatic artery proper, portal vein).
- **Posterior:** IVC (covered by peritoneum) and right crus of the diaphragm.
- **Superior:** Caudate lobe of the liver (caudate process).
- **Inferior:** First part of the duodenum (superior part, D1).
> **Clinical Note – Lesser Sac:**
> - **Pancreatic pseudocyst:** The most common collection in the lesser sac is a pancreatic pseudocyst, resulting from acute or chronic pancreatitis. The pseudocyst is walled off by the boundaries of the lesser sac (stomach anteriorly, pancreas posteriorly). It can cause gastric compression (early satiety, vomiting), biliary obstruction, or vascular complications (splenic artery pseudoaneurysm). Treatment: internal drainage (cystogastrostomy — endoscopic or surgical), or external drainage.
> - **Perforated posterior gastric ulcer:** A posterior gastric ulcer can perforate into the lesser sac. The inflammatory fluid is initially contained within the lesser sac (hence the initial pain may be less severe than an anterior perforation, which spills into the greater sac). However, the fluid can erode into the splenic artery causing massive hemorrhage, or can escape through the epiploic foramen into the greater sac.
> - **Lesser sac abscess:** Can form as a complication of pancreatitis, perforated posterior gastric ulcer, or after gastrectomy. Drainage is required.
> - **Foramen of Winslow hernia:** Extremely rare internal hernia where bowel loops enter the lesser sac through the epiploic foramen. Can cause bowel obstruction.
> - **Pringle maneuver (reiterated):** The anterior boundary of the epiploic foramen is the hepatoduodenal ligament. The Pringle maneuver compresses this structure.
> - **Surgical access to the lesser sac:**
> - Through the **gastrocolic ligament** (between greater curvature of stomach and transverse colon — the most common surgical approach, dividing the greater omentum between the gastroepiploic vessels and the transverse colon).
> - Through the **hepatogastric ligament** (thin, avascular part of the lesser omentum — watch for aberrant left hepatic artery!).
> - Through the **transverse mesocolon** (from below).
#### B. Infracolic Spaces
##### 1. Right Infracolic Space
- Between the mesentery of the small intestine (to the left) and the ascending colon/cecum (to the right), below the transverse mesocolon.
- Larger than the left infracolic space.
- Communicates with the pelvis inferiorly (fluid tracks freely into the right paracolic gutter → pelvic cavity).
##### 2. Left Infracolic Space
- Between the mesentery of the small intestine (to the right) and the descending colon (to the left), below the transverse mesocolon.
- Partially closed off inferiorly by the sigmoid mesocolon.
- Less commonly a site of abscess formation because communication with the pelvis is partially blocked by the sigmoid mesocolon.
#### C. Paracolic Gutters
The paracolic gutters (sulci) are channels on either side of the ascending and descending colon, between the colon and the lateral abdominal wall.
##### 1. Right Paracolic Gutter
- Between the ascending colon and the right lateral abdominal wall.
- **Wider and deeper** than the left.
- **Communicates freely** superiorly with the **right subhepatic space (Morison's pouch)** and the **right subphrenic space**.
- Communicates inferiorly with the **pelvis** (right iliac fossa → rectovesical pouch or rectouterine pouch).
- This gutter is the **main pathway** for the spread of fluid/infection from the right iliac fossa (e.g., ruptured appendix) to the right subphrenic space.
##### 2. Left Paracolic Gutter
- Between the descending colon and the left lateral abdominal wall.
- **Narrower** than the right.
- Superior communication with the left subphrenic space is **partially blocked by the phrenicocolic ligament** (which acts as a barrier at the splenic flexure).
- Communicates inferiorly with the pelvis (though partially blocked by the sigmoid mesocolon).
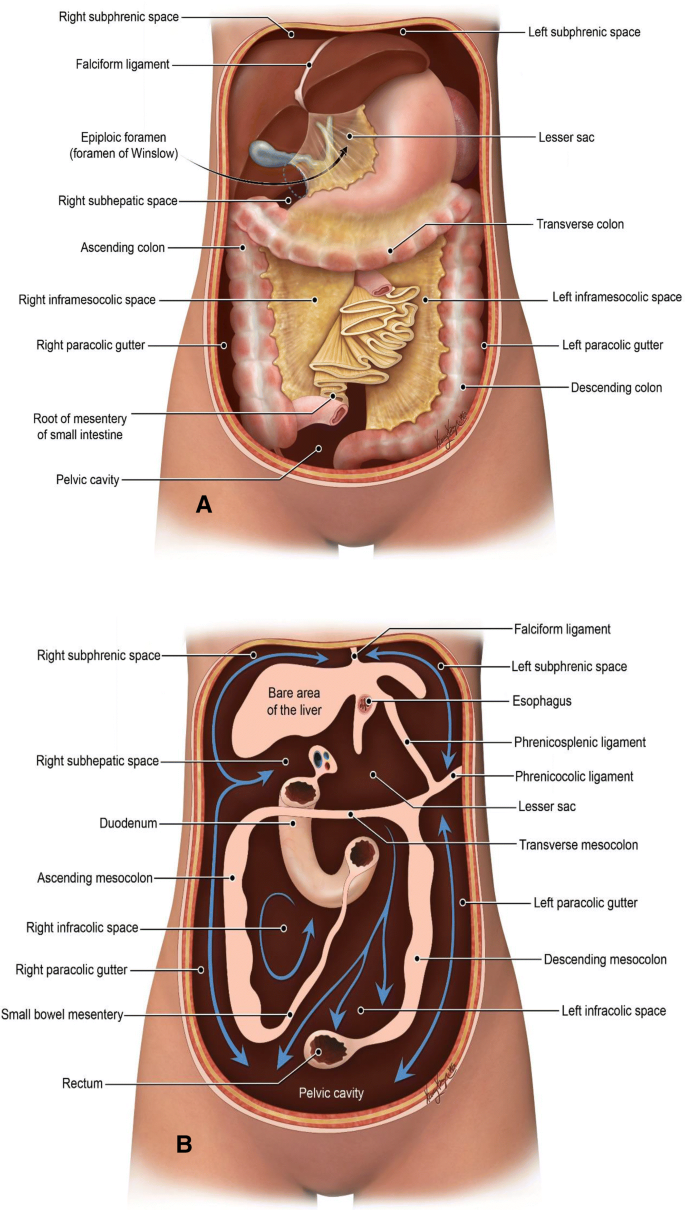
> **Clinical Note – Fluid Flow Pathways:**
> - In a supine patient, intraperitoneal fluid (from a ruptured appendix, perforated ulcer, splenic laceration, etc.) follows gravity and flows along predictable pathways:
> 1. From the **right iliac fossa** → right paracolic gutter → right subhepatic space (Morison's pouch) → right subphrenic space.
> 2. From the **pelvis** → paracolic gutters → subphrenic spaces.
> 3. From the **left upper quadrant** → left paracolic gutter → pelvis (the phrenicocolic ligament limits upward spread on the left).
> - These pathways explain the distribution of **subphrenic abscesses** and **pelvic abscesses** after appendicitis and other conditions.
> - **Practical point for surgeons:** When irrigating the abdomen during surgery, attention must be paid to all these spaces, especially Morison's pouch, both subphrenic spaces, both paracolic gutters, and the pelvis. Failure to irrigate these recesses can lead to residual abscesses.
#### D. Pelvic Peritoneal Spaces
##### In Males:
- The peritoneum descends from the anterior abdominal wall → covers the superior surface of the bladder → reflects onto the anterior surface of the rectum, forming the **rectovesical pouch (pouch of Douglas in males)**.
- The rectovesical pouch is the **most dependent part** of the peritoneal cavity in a **supine male** (and in the erect position).
##### In Females:
The peritoneum creates two pouches:
**(a) Vesicouterine Pouch (Uterovesical Pouch):**
- Between the bladder (anterior) and the uterus (posterior).
- Relatively shallow.
- Usually empty.
**(b) Rectouterine Pouch (Pouch of Douglas / Cul-de-sac of Douglas):**
- Between the uterus/posterior fornix of the vagina (anterior) and the rectum (posterior).
- The **most dependent part of the peritoneal cavity** in the female (both supine and erect).
- Bounded laterally by the **rectouterine folds** (uterosacral ligaments, which contain smooth muscle and the uterosacral nerve plexus).
> **Clinical Note – Pouch of Douglas:**
> - **Fluid collection:** Blood (ruptured ectopic pregnancy), pus (pelvic abscess), ascites, and tumor deposits commonly collect in the pouch of Douglas.
> - **Digital rectal examination (DRE):** The pouch of Douglas can be palpated through the anterior rectal wall. A "boggy" or tender mass suggests a pelvic abscess or blood collection.
> - **Posterior colpotomy (culdocentesis):** In females, fluid in the pouch of Douglas can be aspirated through the posterior fornix of the vagina (the peritoneum of the pouch of Douglas is separated from the posterior vaginal fornix by only a thin layer of tissue). Finding non-clotting blood (hemoperitoneum) supports the diagnosis of ruptured ectopic pregnancy. Though largely replaced by ultrasound and laparoscopy, it remains a useful emergency procedure.
> - **Douglas abscess drainage:** A pelvic abscess in the pouch of Douglas can be drained transrectally (guided by ultrasound or CT) or transvaginally (posterior colpotomy).
> - **Ovarian cancer staging:** The pouch of Douglas is examined for tumor deposits (peritoneal seeding) during surgical staging of ovarian cancer.
> - **Endometriosis:** The pouch of Douglas is one of the most common sites for endometrial implants (ectopic endometrial tissue). This can cause **dyspareunia** (pain during intercourse), **dysmenorrhea**, and chronic pelvic pain. On laparoscopy, "powder burn" or "chocolate cyst" (endometrioma) lesions are seen.
### 2.10 The Greater Sac vs. Lesser Sac Summary
| Feature | Greater Sac | Lesser Sac (Omental Bursa) |
|---|---|---|
| Size | Larger; main peritoneal cavity | Smaller; a diverticulum |
| Location | Everywhere except behind stomach/lesser omentum | Behind stomach, lesser omentum; in front of pancreas |
| Communication | Through epiploic foramen to lesser sac | Through epiploic foramen to greater sac |
| Clinical significance | Main site of ascites, peritonitis, tumor spread | Pancreatic pseudocysts, posterior gastric ulcer perforations |
---
## PART 3: PERITONEAL FLUID AND ITS CLINICAL SIGNIFICANCE
### 3.1 Normal Peritoneal Fluid
- **Volume:** 50-100 mL
- **Composition:** Ultrafiltrate of plasma — contains water, electrolytes, proteins (mostly albumin, at lower concentration than plasma), small number of cells (mesothelial cells, macrophages, lymphocytes, mast cells)
- **Function:** Lubrication, immune surveillance, nutrient transport
- **Turnover:** Approximately 1 liter per day is produced and reabsorbed
### 3.2 Ascites
**Ascites** is the pathological accumulation of fluid in the peritoneal cavity (>25 mL, though clinically detectable when >500 mL-1L).
**Causes:**
- **Transudative (protein <2.5 g/dL; SAAG ≥1.1 g/dL):**
- Cirrhosis (most common cause overall — ~85%)
- Congestive heart failure (cardiac ascites)
- Nephrotic syndrome
- Hypoalbuminemia (malnutrition, hepatic failure)
- Budd-Chiari syndrome
- Constrictive pericarditis
- **Exudative (protein >2.5 g/dL; SAAG <1.1 g/dL):**
- Peritoneal carcinomatosis (ovarian, gastric, colon cancer)
- Tuberculous peritonitis
- Peritoneal mesothelioma
- Pancreatitis
- Connective tissue diseases (SLE)
- Meigs syndrome (ovarian fibroma + ascites + pleural effusion)
**SAAG (Serum-Ascites Albumin Gradient):**
- SAAG = Serum albumin - Ascites albumin
- ≥1.1 g/dL → Portal hypertension (97% accuracy)
- <1.1 g/dL → Non-portal hypertension causes
> **Clinical Note:**
> - **Detection of ascites:**
> - **Shifting dullness:** Percussion of the flanks in supine position (dull flanks, resonant center), then turning the patient on one side and re-percussing (the area of dullness shifts to the dependent side). Requires >500 mL of fluid.
> - **Fluid thrill:** Place one hand on each flank; tap one side while an assistant places the edge of their hand firmly in the midline to block transmission through subcutaneous fat. A transmitted impulse (thrill) felt on the other side indicates large-volume ascites (>1-2L).
> - **Puddle sign:** Patient prone for 5 minutes then rises on elbows and knees; stethoscope placed on the most dependent part of the abdomen; flicking finger against the flank; increased intensity of sound indicates small-volume ascites (detects as little as 120 mL). Rarely used now.
> - **Ultrasound:** Most sensitive clinical method. Can detect as little as 100 mL.
> - **CT scan:** Also very sensitive; identifies loculated collections and associated pathology.
> - **Paracentesis (abdominal tap / ascitic tap):** Performed at a point two-thirds of the way from the umbilicus to the ASIS (in the left iliac fossa, to avoid the cecum on the right), or in the midline below the umbilicus. Avoid the inferior epigastric artery (use the Z-track technique to prevent persistent leakage). Diagnostic paracentesis (small volume) or therapeutic paracentesis (large volume — 4-6 liters or more, with albumin replacement to prevent post-paracentesis circulatory dysfunction).
> - **Spontaneous bacterial peritonitis (SBP):** In cirrhotic patients with ascites, bacteria (usually gram-negative enterics — *E. coli*, *Klebsiella*) can translocate from the gut into the ascitic fluid without a surgical source. Diagnosed by ascitic fluid PMN count ≥250 cells/mm³. Treated with IV ceftriaxone or cefotaxime.
### 3.3 Pneumoperitoneum
**Pneumoperitoneum** is the presence of free air (gas) in the peritoneal cavity.
**Causes:**
- **Perforation of a hollow viscus:** Most common cause — perforated peptic ulcer (most common), perforated appendix, perforated diverticulitis, perforated bowel (trauma, malignancy, ischemia, inflammatory bowel disease).
- **Post-surgical:** After laparotomy or laparoscopy (air is deliberately introduced during laparoscopy — CO₂). This post-operative pneumoperitoneum can persist for up to 7 days.
- **Per vagina:** Air can enter through the female genital tract (after pelvic examination, intercourse, vaginal douching). Remember, the female peritoneal cavity communicates with the exterior.
- **Other rare causes:** Peritoneal dialysis, pneumatosis intestinalis, jejunal diverticulosis.
> **Clinical Note:**
> - **Erect chest X-ray** (or left lateral decubitus abdominal film): **Free air under the diaphragm** (subdiaphragmatic air) is the hallmark of pneumoperitoneum. The right hemidiaphragm is easier to evaluate (on the left, the gastric bubble may cause confusion). As little as 1-2 mL of free air can be detected on an erect film.
> - **Rigler's sign (double wall sign):** On supine abdominal X-ray, both the inner (mucosal) and outer (serosal) walls of the bowel are visible, indicating free air on both sides of the bowel wall.
> - **"Football sign":** In neonates with necrotizing enterocolitis (NEC), massive pneumoperitoneum creates a large oval lucency resembling a football.
> - **Management:** Pneumoperitoneum due to bowel perforation is a **surgical emergency** requiring resuscitation and laparotomy (or laparoscopy). Exception: if the clinical picture strongly suggests a benign cause (e.g., post-laparoscopy), conservative management may be appropriate.
---
## PART 4: EMBRYOLOGY OF THE PERITONEUM (Relevant to Understanding Adult Anatomy)
### 4.1 Development
- The peritoneal cavity develops from the **intraembryonic coelom** (lateral plate mesoderm splits into somatic and splanchnic layers; the space between them is the coelom).
- The **splanchnic mesoderm** gives rise to the visceral peritoneum.
- The **somatic mesoderm** gives rise to the parietal peritoneum.
- Initially, the gut tube (from the foregut to the hindgut) is suspended in the midline by a **dorsal mesentery** (continuous) and a **ventral mesentery** (only in the foregut — future lesser omentum and falciform ligament).
### 4.2 Fate of the Ventral Mesentery
- The ventral mesentery persists only in the region of the foregut (from the esophagus to the proximal duodenum).
- It gives rise to:
- **Lesser omentum** (hepatogastric + hepatoduodenal ligaments)
- **Falciform ligament** (from the liver to the anterior abdominal wall)
- The liver develops within the ventral mesentery, dividing it into the lesser omentum (behind) and falciform ligament (in front).
### 4.3 Fate of the Dorsal Mesentery
- The dorsal mesentery is present along the entire length of the GI tract.
- It gives rise to:
- **Greater omentum** (dorsal mesogastrium — expands enormously)
- **Gastrosplenic ligament** (part of dorsal mesogastrium; the spleen develops within it)
- **Splenorenal ligament** (part of dorsal mesogastrium)
- **Mesentery proper** (of small intestine)
- **Transverse mesocolon**
- **Sigmoid mesocolon**
- **Mesoappendix**
### 4.4 Rotation of the Stomach and Formation of the Lesser Sac
- The stomach undergoes a **90° clockwise rotation** (viewed from above):
- The left side faces anteriorly → left vagus nerve (anterior vagal trunk) comes to lie on the anterior surface.
- The right side faces posteriorly → right vagus nerve (posterior vagal trunk) comes to lie on the posterior surface.
- The original posterior border (dorsal mesentery attachment) becomes the greater curvature.
- The original anterior border (ventral mesentery attachment) becomes the lesser curvature.
- The dorsal mesogastrium elongates enormously and grows to the left and downward, forming the greater omentum.
- The space behind the stomach (originally on the right side of the dorsal mesentery) expands to form the **lesser sac (omental bursa)**.
- The communication with the main peritoneal cavity (greater sac) narrows to become the **epiploic foramen**.
### 4.5 Fusion of Mesenteries and Formation of Retroperitoneal Structures
During development, certain segments of the gut rotate and their mesenteries fuse with the posterior body wall peritoneum, making these organs **secondarily retroperitoneal**:
- **Duodenum (D2-D4):** Originally had a mesentery; during rotation of the midgut and growth, the duodenal loop becomes pressed against the posterior body wall, and its mesentery fuses with the posterior parietal peritoneum.
- **Pancreas:** Similarly, the pancreas (which developed in the dorsal and ventral mesenteries) becomes pressed against the posterior body wall and fuses (except for the tail).
- **Ascending and descending colon:** After the midgut and hindgut rotation, the ascending colon (from the midgut) and descending colon (from the hindgut) press against the posterior body wall and their mesenteries fuse → the plane of fusion creates the "**fascia of Toldt**" (actually a fusion fascia, not a true fascia). This is the avascular plane used by surgeons during colonic mobilization.
> **Clinical Note – Malrotation and Volvulus:**
> - **Intestinal malrotation:** Failure of normal rotation of the midgut (270° counterclockwise rotation around the SMA axis). The cecum remains in the upper abdomen, and abnormal peritoneal bands (**Ladd's bands**) cross from the cecum to the right lateral abdominal wall, potentially obstructing the duodenum. The mesentery has a narrow pedicle, predisposing to **midgut volvulus** (twisting of the entire small intestine and part of the colon around the SMA → ischemia and necrosis of the entire midgut).
> - **Midgut volvulus** is a **life-threatening surgical emergency** in neonates. Presents with **bilious vomiting** (green vomitus) in a neonate. Upper GI contrast study shows the "**corkscrew sign**" or "**bird's beak sign**" with abnormal position of the duodenojejunal flexure (ligament of Treitz to the right of the midline).
> - **Ladd's procedure:** The surgery for malrotation involves:
> 1. Counterclockwise detorsion of the volvulus
> 2. Division of Ladd's bands
> 3. Widening of the mesenteric base
> 4. Appendectomy (because the appendix is in an abnormal position and future diagnosis of appendicitis would be confused)
> 5. Placement of the small bowel in the right abdomen and colon in the left
---
## PART 5: PERITONEAL REFLECTIONS AND SPECIFIC ORGAN RELATIONSHIPS
### 5.1 Peritoneal Reflections of the Liver
- Almost entirely covered by peritoneum except at the **bare area**.
- **Bare area:** The posterior surface of the right lobe of the liver between the two layers of the coronary ligament. Here, the liver is in direct contact with the diaphragm and the right adrenal gland. The IVC groove runs through this area.
- **Peritoneal attachments:**
- Coronary ligament (anterior and posterior layers)
- Right and left triangular ligaments
- Falciform ligament (to anterior abdominal wall)
- Lesser omentum (to lesser curvature of stomach and first part of duodenum)
- Hepatorenal ligament (to right kidney)
- **Fissure for ligamentum teres:** On the inferior surface; contains the round ligament of the liver (obliterated left umbilical vein).
- **Fissure for ligamentum venosum:** On the posterior surface; contains the ligamentum venosum (obliterated ductus venosus). The lesser omentum (hepatogastric ligament) is attached at this fissure.
### 5.2 Peritoneal Reflections of the Spleen
- Completely covered by peritoneum (the only fully intraperitoneal lymphoid organ, though not a lymph node — it is the largest lymphoid organ).
- **Peritoneal attachments:**
- Gastrosplenic ligament (to stomach)
- Splenorenal (lienorenal) ligament (to left kidney)
- Phrenicocolic ligament (supports the splenic flexure and inferior pole of the spleen)
- Splenocolic ligament (less constant; from inferior pole to splenic flexure)
> **Clinical Note – Spleen:**
> - The spleen is the **most commonly injured abdominal organ** in blunt abdominal trauma (e.g., motor vehicle accidents, falls, sports injuries). It is relatively fragile, highly vascular, and partially protected by the 9th-11th ribs on the left side.
> - **Left lower rib fractures** (ribs 9-12) should raise suspicion of splenic injury.
> - **Kehr's sign:** Left shoulder tip pain (referred via phrenic nerve irritation by blood under the left hemidiaphragm) in splenic rupture.
> - **Delayed splenic rupture:** Can occur days to weeks after the initial injury. A subcapsular hematoma expands and eventually ruptures. Therefore, patients with splenic injuries managed non-operatively require monitoring.
> - **Splenectomy complications:**
> - **OPSI (Overwhelming Post-Splenectomy Infection):** Life-threatening sepsis from encapsulated organisms (*Streptococcus pneumoniae*, *Haemophilus influenzae*, *Neisseria meningitidis*). Lifetime risk. Prevention: vaccination (pneumococcal, meningococcal, H. influenzae type B) ideally 2 weeks before elective splenectomy or ASAP after emergency splenectomy, plus daily prophylactic penicillin (especially in children).
> - **Thrombocytosis:** Platelet count can rise significantly after splenectomy, increasing thrombotic risk.
> - **Howell-Jolly bodies, target cells:** Seen on blood smear after splenectomy (normally the spleen removes nuclear remnants and abnormal red cells).
> - **Splenosis:** After splenic rupture or splenectomy, fragments of splenic tissue can implant on peritoneal surfaces and grow (autotransplantation). These splenic implants can occasionally provide some splenic function.
> - **Accessory spleen (splenunculus):** Present in ~10-30% of people, usually near the splenic hilum, in the gastrosplenic or splenorenal ligament, or in the greater omentum. Important to identify and remove during splenectomy for hematologic conditions (e.g., ITP), as a missed accessory spleen can cause recurrence.
### 5.3 Peritoneal Reflections of the Stomach
- Almost completely covered by peritoneum.
- **Greater curvature:** Gives attachment to the greater omentum (gastrocolic ligament — part of greater omentum connecting stomach to transverse colon) and the gastrosplenic ligament.
- **Lesser curvature:** Gives attachment to the lesser omentum.
- **Posterior surface:** Forms the anterior wall of the lesser sac. Related to the "stomach bed" (structures behind the stomach): pancreas, splenic artery, left kidney, left adrenal gland, spleen, transverse mesocolon, splenic flexure of colon.
- **Anterior surface:** Covered by peritoneum of the greater sac. Related to the left lobe of the liver, anterior abdominal wall, and diaphragm.
> **Clinical Note – Stomach Bed:**
> - A posterior gastric ulcer can erode into structures of the stomach bed, particularly the **splenic artery** (causing massive hemorrhage — the most important vessel in the stomach bed) or the **pancreas** (causing pancreatitis).
> - **Gastric ulcer perforation:**
> - Anterior perforation → peritonitis (gastric acid leaks into the greater sac → severe chemical peritonitis → board-like rigidity → free air under diaphragm on erect CXR).
> - Posterior perforation → lesser sac abscess (contained initially) or erosion into splenic artery (catastrophic hemorrhage).
### 5.4 Peritoneum of the Intestines
#### Small Intestine (Jejunum and Ileum):
- Completely covered by peritoneum (intraperitoneal).
- Suspended by the mesentery proper.
- **Differences between jejunum and ileum:**
| Feature | Jejunum | Ileum |
|---|---|---|
| Location | Upper left abdomen | Lower right abdomen |
| Wall thickness | Thicker (more folds) | Thinner |
| Vascularity | More vascular (redder) | Less vascular (paler) |
| Vasa recta | Long, infrequent | Short, more frequent |
| Arterial arcades | 1-2 tiers | 4-5 tiers |
| Fat in mesentery | Less | More (windows less transparent) |
| Plicae circulares (valvulae conniventes) | Prominent, tall, closely spaced | Sparse, low, absent in terminal ileum |
| Peyer's patches | Few/absent | Abundant (antimesenteric border) |
| Lymphoid tissue | Sparse | Prominent |
| Diameter | Wider (2.5-3 cm) | Narrower (2 cm) |
> **Clinical Note:**
> - **Meckel's diverticulum:** A remnant of the vitellointestinal (omphalomesenteric) duct, present in ~2% of the population. Found on the antimesenteric border of the ileum, approximately 2 feet (60 cm) from the ileocecal valve. May contain ectopic gastric mucosa (in ~50%) or pancreatic tissue. The "Rule of 2s": 2% of population, 2 feet from ileocecal valve, 2 inches long, 2 types of ectopic tissue, presents before age 2 (though can present at any age), 2:1 male predominance. Complications: bleeding (ectopic gastric acid causes ulceration of adjacent ileal mucosa → painless rectal bleeding — may appear as melena or bright red blood), obstruction (via a band/fibrous remnant to the umbilicus), diverticulitis (clinically indistinguishable from appendicitis), perforation, intussusception. Diagnosed by **Meckel's (technetium-99m pertechnetate) scan** (detects ectopic gastric mucosa).
#### Large Intestine:
- **Cecum:** Usually intraperitoneal (but variable; may have short mesentery or be retroperitoneal).
- **Ascending colon:** Secondarily retroperitoneal.
- **Transverse colon:** Intraperitoneal (suspended by transverse mesocolon).
- **Descending colon:** Secondarily retroperitoneal.
- **Sigmoid colon:** Intraperitoneal (suspended by sigmoid mesocolon).
- **Rectum:**
- Upper third: peritoneum on front and sides (intraperitoneal)
- Middle third: peritoneum on front only
- Lower third: below the peritoneal reflection (subperitoneal/extraperitoneal)
> **Clinical Note:**
> - **Rectal cancer surgery:** The level of the tumor relative to the peritoneal reflection determines the type of surgery:
> - Tumors above the peritoneal reflection → anterior resection with primary anastomosis.
> - Tumors below the peritoneal reflection → abdominoperineal resection (APR) with permanent colostomy (Miles' procedure), or ultra-low anterior resection with coloanal anastomosis and temporary defunctioning ileostomy.
> - **Total mesorectal excision (TME):** Modern rectal cancer surgery involves excising the rectum with its entire mesorectal envelope (the perirectal fat and lymph nodes, enclosed by the mesorectal fascia — fascia propria of the rectum). This has dramatically reduced local recurrence rates.
---
## PART 6: SPECIFIC CLINICAL CONDITIONS RELATED TO THE PERITONEUM
### 6.1 Peritonitis
**Definition:** Inflammation of the peritoneum.
**Classification:**
#### A. Primary (Spontaneous) Peritonitis
- Infection of the peritoneal cavity without an identifiable intra-abdominal surgical source.
- **Spontaneous bacterial peritonitis (SBP):** In patients with cirrhosis and ascites. Organisms: *E. coli*, *Klebsiella*, *Streptococcus pneumoniae*. Diagnosed by ascitic fluid PMN count ≥250/mm³ and positive culture (monomicrobial). Treatment: IV cephalosporin (cefotaxime) + IV albumin.
- **Primary peritonitis in children:** Associated with nephrotic syndrome or post-streptococcal disease. Organism: *S. pneumoniae*.
- **Tuberculous peritonitis:** Due to *Mycobacterium tuberculosis*. Can be primary (hematogenous) or secondary (from intestinal or fallopian tube TB). "Doughy abdomen" on palpation. Ascites with high protein, high lymphocyte count, elevated adenosine deaminase (ADA) level. Peritoneal biopsy shows caseating granulomas ("millet seed" nodules on laparoscopy).
#### B. Secondary Peritonitis
- Due to contamination of the peritoneal cavity from a surgical/traumatic source.
- **Causes:**
- Perforated hollow viscus (peptic ulcer, appendicitis, diverticulitis, colorectal cancer, typhoid perforation)
- Gangrenous bowel (ischemia, strangulated hernia)
- Penetrating trauma
- Post-operative anastomotic leak
- Ruptured liver/splenic abscess
- **Bacteriology:** Polymicrobial — aerobic (E. coli, Enterococcus) and anaerobic (Bacteroides fragilis, Clostridium) organisms.
- **Clinical features:** Severe abdominal pain, guarding, rigidity, absent bowel sounds (paralytic ileus), fever, tachycardia, hypotension, dehydration.
- **Treatment:** Resuscitation (IV fluids, NGT decompression, urinary catheter, antibiotics — broad-spectrum covering gram-negatives and anaerobes) + **emergency surgery** to control the source (repair perforation, resect gangrenous bowel, drain abscess, peritoneal lavage).
#### C. Tertiary Peritonitis
- Persistent or recurrent infection after apparently successful treatment of secondary peritonitis.
- Often caused by nosocomial organisms (*Enterococcus*, *Candida*, *Staphylococcus epidermidis*) or multi-drug resistant bacteria.
- Seen in immunocompromised or critically ill patients.
- High mortality.
#### D. Chemical Peritonitis (Aseptic Peritonitis)
- Caused by irritation of the peritoneum by non-infected substances:
- **Gastric acid** (perforated peptic ulcer — most severe chemical peritonitis)
- **Bile** (ruptured gallbladder, bile duct injury — bile peritonitis)
- **Pancreatic enzymes** (acute pancreatitis)
- **Blood** (hemoperitoneum — relatively mild irritant)
- **Urine** (ruptured bladder — uroperitoneum)
- **Barium** (barium enema with perforation — barium peritonitis, very severe)
- **Meconium** (neonatal meconium peritonitis from bowel perforation in utero)
> **Clinical Note:**
> - **Perforated peptic ulcer timeline:**
> 1. **Phase 1 (0-2 hours): Chemical peritonitis.** Gastric acid (pH ~1-2) causes severe chemical irritation → intense epigastric pain, board-like rigidity, patient lies very still.
> 2. **Phase 2 (2-12 hours): "Period of deceptive improvement."** The body dilutes the acid with peritoneal fluid. Pain may decrease. The unwary clinician may think the patient is improving.
> 3. **Phase 3 (>12 hours): Bacterial peritonitis.** Contamination by oral and intestinal bacteria leads to secondary bacterial peritonitis → fever, sepsis, cardiovascular collapse.
> - **Gasless perforation:** Approximately 20-30% of perforated peptic ulcers do not show free air under the diaphragm on erect CXR (the perforation may be sealed by omentum, or too small for significant air leak). CT scan is more sensitive.
### 6.2 Peritoneal Adhesions
**Definition:** Abnormal fibrous bands connecting structures within the peritoneal cavity.
**Causes:**
- **Post-surgical (most common — ~90%):** Any abdominal or pelvic surgery can cause adhesions. The risk increases with the number of surgeries. Lower abdominal and pelvic surgeries (appendectomy, hysterectomy, colorectal surgery) are the most common causes.
- **Post-inflammatory:** Peritonitis (any cause), PID, endometriosis, Crohn's disease, radiation.
- **Congenital:** Ladd's bands (in malrotation), Jackson's membrane (peritoneal veil over the ascending colon).
**Pathophysiology:** Surgical trauma, ischemia, infection, or foreign body exposure (talc from gloves, suture material, gauze fibers) damages the mesothelial surface. Fibrin is deposited. Normally, fibrin is lysed by peritoneal fibrinolytic activity (tissue plasminogen activator, tPA). If fibrinolytic activity is suppressed (by inflammation, ischemia), the fibrin organizes into permanent fibrous adhesions with blood vessel ingrowth.
**Clinical Significance:**
1. **Intestinal obstruction:** Adhesions are the **most common cause of small bowel obstruction** (~60-70% in developed countries). The bowel can become kinked, compressed, or herniated through an adhesive band. Can lead to strangulation.
2. **Chronic abdominal pain:** Controversial association.
3. **Infertility:** Pelvic adhesions can occlude the fallopian tubes or fix the ovaries, preventing ovum pickup.
4. **Difficulty in subsequent surgery (hostile abdomen):** Dense adhesions make re-operation difficult and increase the risk of inadvertent bowel injury (enterotomy).
**Prevention strategies:**
- Good surgical technique (minimize tissue handling, avoid desiccation, meticulous hemostasis, minimal use of foreign materials)
- **Laparoscopic surgery** (less adhesion formation compared to open surgery — due to less tissue handling and desiccation)
- **Anti-adhesion barriers:** Hyaluronic acid/carboxymethylcellulose membrane (Seprafilm®), oxidized regenerated cellulose (Interceed®), 4% icodextrin solution (Adept®)
- Avoiding talc/starch on gloves
### 6.3 Peritoneal Dialysis
**Principle:** Uses the peritoneum as a semipermeable membrane for dialysis in patients with end-stage renal disease (ESRD).
**Method:** A dialysis catheter (**Tenckhoff catheter**) is placed into the peritoneal cavity (usually in the lower abdomen/pelvis, midline or paramedian). Dialysis solution (containing glucose as an osmotic agent, and electrolytes) is instilled into the peritoneal cavity → remains for a dwell time (4-6 hours for CAPD, or shorter for APD) → solutes (urea, creatinine, potassium) diffuse from peritoneal capillary blood into the dialysis solution → fluid is also drawn by osmosis → the used solution is drained.
**Types:**
- **CAPD (Continuous Ambulatory Peritoneal Dialysis):** 4 exchanges per day, done manually by the patient. Each exchange: 2-2.5 L of dialysate, dwell time 4-6 hours.
- **APD (Automated Peritoneal Dialysis):** A machine performs exchanges overnight while the patient sleeps.
**Complications:**
- **Peritonitis:** Most common serious complication. Usually caused by touch contamination (*S. aureus*, *S. epidermidis*, gram-negative rods). Cloudy effluent, abdominal pain, fever. Treatment: intraperitoneal antibiotics.
- **Exit site/tunnel infection**
- **Catheter malfunction** (displacement, omental wrapping, fibrin occlusion)
- **Hernias** (increased intra-abdominal pressure → inguinal, umbilical, or incisional hernias)
- **Hydrothorax** (fluid tracks from the peritoneal cavity through congenital diaphragmatic defects into the pleural cavity — usually right-sided)
- **Encapsulating peritoneal sclerosis (sclerosing peritonitis):** Long-term PD → thickening and fibrosis of the peritoneum → the bowel becomes encased in a cocoon of fibrous tissue ("cocoon abdomen") → small bowel obstruction. Rare but serious.
- **Loss of ultrafiltration** (peritoneal membrane failure over time)
- **Metabolic:** Hyperglycemia (glucose-based dialysate), protein loss (through the peritoneum), weight gain, hyperlipidemia.
### 6.4 Peritoneal Carcinomatosis
**Definition:** Widespread metastatic tumor deposits on the peritoneal surfaces.
**Common primary tumors:**
- Ovarian cancer (most common cause of peritoneal carcinomatosis in women)
- Colorectal cancer
- Gastric cancer
- Appendiceal mucinous neoplasms (pseudomyxoma peritonei)
- Pancreatic cancer
- Mesothelioma (primary peritoneal malignancy)
**Mechanism of spread:**
1. **Transcoelomic (transperitoneal) spread:** Cancer cells exfoliate from the surface of an involved organ → float in peritoneal fluid → implant on peritoneal surfaces (especially in dependent areas: pouch of Douglas, right paracolic gutter, omentum, diaphragm).
2. **Direct invasion:** Primary tumor invades through the visceral peritoneum.
**Characteristic sites of deposit:**
- **Pouch of Douglas** (Blumer's shelf — palpable on DRE as a hard, shelf-like mass in the rectovesical/rectouterine pouch)
- **Greater omentum** (omental cake)
- **Ovaries** (Krukenberg tumor — secondary ovarian tumors, especially from gastric cancer; bilateral, with signet-ring cells)
- **Umbilicus** (Sister Mary Joseph nodule — metastatic deposit in the umbilicus, can occur from stomach, ovarian, colorectal, pancreatic cancer. Named after Sister Mary Joseph Dempsey, surgical assistant to Dr. William Mayo at Mayo Clinic)
- **Peritoneal surfaces** generally (studding of the peritoneum)
> **Clinical Note:**
> - **Virchow's node (signal node/sentinel node):** Left supraclavicular lymph node enlargement due to metastatic spread from abdominal cancers (especially gastric cancer) via the thoracic duct. Also known as **Troisier's sign**.
> - **Irish's node:** Left axillary lymph node enlargement from gastric cancer.
> - **Pseudomyxoma peritonei ("jelly belly"):** Large amounts of mucinous ascites filling the peritoneal cavity, usually from a ruptured appendiceal mucinous neoplasm. The peritoneum becomes coated with mucinous tumor. Treatment: **cytoreductive surgery (CRS) + HIPEC** (Hyperthermic Intraperitoneal Chemotherapy — heated chemotherapy solution bathed over the peritoneal surfaces intraoperatively at 42°C for 90 minutes). Sugarbaker technique.
### 6.5 Meigs Syndrome
- Triad of: **ovarian fibroma** (or other ovarian tumors) + **ascites** + **pleural effusion** (usually right-sided).
- All features resolve after removal of the tumor.
- The ascites is caused by transudation from the tumor surface, and the pleural effusion is caused by passage of ascitic fluid through lymphatic channels in the diaphragm.
### 6.6 Endometriosis of the Peritoneum
- Ectopic endometrial tissue implants on peritoneal surfaces.
- Most common sites: pouch of Douglas, uterosacral ligaments, ovaries, fallopian tubes, rectovaginal septum.
- Causes: cyclical bleeding from the implants → inflammation → adhesions → pain and infertility.
- **Sampson's theory of retrograde menstruation:** Menstrual blood flows backwards through the fallopian tubes into the peritoneal cavity, depositing viable endometrial cells.
- **Laparoscopy** is the gold standard for diagnosis: reveals "powder burn" (black/dark brown) lesions, "blueberry spots," red vesicular lesions, or white scarred lesions.
---
## PART 7: SPECIAL TOPICS
### 7.1 Ligament of Treitz (Suspensory Muscle of the Duodenum)
- A musculofibrous band (containing skeletal muscle superiorly and smooth muscle inferiorly) extending from the right crus of the diaphragm to the duodenojejunal flexure (DJF).
- **Function:** Suspends the DJF at its fixed position (left of L2 vertebra).
- **Clinical significance:**
- **Upper vs. Lower GI bleeding:** The ligament of Treitz is used as the landmark to divide the GI tract into upper and lower portions.
- **Upper GI bleed:** Proximal to the ligament of Treitz (esophagus, stomach, D1-D4).
- **Lower GI bleed:** Distal to the ligament of Treitz (jejunum, ileum, colon, rectum, anus).
- Upper GI bleeding typically presents with hematemesis (vomiting blood) and/or melena (black tarry stools).
- Lower GI bleeding typically presents with hematochezia (bright red blood per rectum).
- **Exceptions:** Massive upper GI bleeding can present with hematochezia (the blood passes through the GI tract too quickly to be degraded). Proximal lower GI bleeding (e.g., right colon) can present with melena.
- **Superior mesenteric artery syndrome (Wilkie's syndrome/Cast syndrome):** Compression of the third part of the duodenum (D3) between the SMA anteriorly and the aorta posteriorly. Can occur after significant weight loss (loss of retroperitoneal fat that normally cushions the mesenteric root), spinal surgery, prolonged bed rest, or body cast application. Presents with postprandial epigastric pain, nausea, bilious vomiting, weight loss. Treatment: nutritional support, left lateral decubitus or prone positioning after meals, and in refractory cases, duodenojejunostomy.
### 7.2 Peritoneal Innervation Summary
| Structure | Nerve Supply | Pain Character | Pain Location |
|---|---|---|---|
| Parietal peritoneum (anterior wall) | Somatic (T7-L1) | Sharp, well-localized | Directly over the inflamed area |
| Parietal peritoneum (diaphragm, central) | Phrenic nerve (C3-C5) | Referred | Shoulder tip (C3-C4 dermatome) |
| Parietal peritoneum (diaphragm, peripheral) | Lower intercostal nerves | Localized | Thoracoabdominal wall |
| Parietal peritoneum (pelvic) | Obturator nerve (L2-L4) | Referred | Medial thigh/knee |
| Visceral peritoneum (foregut) | Splanchnic nerves (T5-T9) | Dull, poorly localized | Epigastrium |
| Visceral peritoneum (midgut) | Splanchnic nerves (T10-T11) | Dull, poorly localized | Periumbilical |
| Visceral peritoneum (hindgut) | Splanchnic nerves (T11-L2) | Dull, poorly localized | Suprapubic |
### 7.3 Blood Supply of the Peritoneum
- **Parietal peritoneum:** Supplied by arteries of the body wall — intercostal, subcostal, lumbar, superior and inferior epigastric, deep circumflex iliac arteries.
- **Visceral peritoneum:** Supplied by the same arteries that supply the underlying organ — branches of the celiac trunk (foregut), SMA (midgut), IMA (hindgut).
### 7.4 Lymphatic Drainage of the Peritoneum
- **Parietal peritoneum:**
- Anterior and lateral walls → axillary, internal thoracic (parasternal), and external iliac lymph nodes.
- Diaphragmatic peritoneum → mediastinal lymph nodes (through diaphragmatic stomata).
- Pelvic peritoneum → internal and external iliac lymph nodes.
- **Visceral peritoneum:** Drains with the organ it covers → preaortic lymph nodes (celiac, SMA, IMA nodes).
> **Clinical Note:**
> - The lymphatic communication between the diaphragmatic peritoneum and the mediastinum explains:
> - Rapid development of **bacteremia in peritonitis** (bacteria absorbed through diaphragmatic stomata → thoracic duct → bloodstream).
> - **Right-sided pleural effusion** in subphrenic abscess and liver pathology.
> - Spread of **ovarian cancer** to mediastinal lymph nodes.
### 7.5 Nerve Supply to Abdominal Organs and Referred Pain Patterns
Understanding peritoneal innervation helps explain referred pain:
| Organ | Autonomic Innervation | Visceral Pain Referral | When Parietal Peritoneum Involved |
|---|---|---|---|
| Stomach/Duodenum (D1-D2) | Greater splanchnic → celiac plexus (T5-T9) | Epigastrium | Localized to site |
| Liver/Gallbladder | Greater splanchnic → celiac plexus (T5-T9) | Epigastrium/right hypochondrium | Right hypochondrium + right shoulder (if diaphragmatic peritoneum irritated) |
| Spleen | Greater splanchnic → celiac plexus | Left hypochondrium | Left shoulder (Kehr's sign) |
| Small intestine | Lesser splanchnic → SMA plexus (T10-T11) | Periumbilical | Localized |
| Appendix | Lesser splanchnic → SMA plexus (T10) | Periumbilical → RIF (when parietal peritoneum involved) | McBurney's point |
| Ascending/Transverse colon (proximal 2/3) | SMA plexus (T10-T11) | Periumbilical | Localized |
| Descending/Sigmoid colon | IMA plexus/hypogastric plexus (T11-L2) | Suprapubic | Localized (LIF) |
| Kidney/Ureter | Renal plexus (T10-L1) | Flank → loin to groin | Not applicable (retroperitoneal) |
| Bladder | Pelvic splanchnic (S2-S4) / hypogastric plexus | Suprapubic | Suprapubic |
| Uterus | Hypogastric plexus (T10-L2) | Low back, lower abdomen | Lower abdomen |
| Ovary/Testis | T10 | Periumbilical (testicular pain can be referred to the umbilical region and vice versa) | Lower abdomen/groin |
> **Clinical Note:**
> - **Testicular pain referred to the abdomen:** Because the testis is supplied by T10 (same as the umbilical region), testicular pathology (torsion, orchitis) can present as periumbilical abdominal pain, especially in children. Always examine the scrotum in any male with abdominal pain!
> - **Referred pain to the shoulder:** Any pathology irritating the diaphragmatic peritoneum (subphrenic abscess, splenic rupture, liver abscess, perforated ulcer with subdiaphragmatic air/fluid) can cause shoulder tip pain via the phrenic nerve (C3-C5).
---
## PART 8: SUMMARY OF KEY PERITONEAL RELATIONSHIPS AND CLINICAL CORRELATIONS
### Quick Reference: Peritoneal Spaces and Their Clinical Significance
| Space/Recess | Location | Most Dependent? | Clinical Significance |
|---|---|---|---|
| **Hepatorenal recess (Morison's pouch)** | Between right liver and right kidney | Yes (supracolic, supine) | First place fluid collects; FAST exam target |
| **Right subphrenic space** | Between diaphragm and right liver | No | Subphrenic abscess |
| **Left subphrenic space** | Between diaphragm and left liver/stomach | No | Subphrenic abscess (less common) |
| **Lesser sac (omental bursa)** | Behind stomach | No | Pancreatic pseudocyst, posterior ulcer perforation |
| **Right paracolic gutter** | Right of ascending colon | No | Pathway for fluid spread to subphrenic space |
| **Left paracolic gutter** | Left of descending colon | No | Narrower; partially blocked by phrenicocolic ligament |
| **Pouch of Douglas / Rectovesical pouch** | Between rectum and uterus/bladder | Yes (most dependent overall) | Fluid/blood/pus collection; culdocentesis; Blumer's shelf |
| **Paraduodenal fossae** | Near DJF | No | Internal hernias |
| **Intersigmoid recess** | Behind sigmoid mesocolon apex | No | Internal hernia; ureter landmark |
### Quick Reference: Important Peritoneal Structures
| Structure | Connects | Contains |
|---|---|---|
| **Falciform ligament** | Liver ↔ Anterior body wall | Ligamentum teres (obliterated left umbilical vein), paraumbilical veins |
| **Lesser omentum** | Lesser curvature of stomach/D1 ↔ Liver | Hepatogastric lig: gastric vessels; Hepatoduodenal lig: portal triad (CBD, hepatic artery, portal vein) |
| **Greater omentum** | Greater curvature of stomach ↔ Transverse colon | Gastroepiploic vessels, fat, lymphoid tissue ("milky spots"), macrophages |
| **Gastrosplenic ligament** | Stomach ↔ Spleen | Short gastric vessels, left gastroepiploic vessels |
| **Splenorenal ligament** | Spleen ↔ Left kidney | Splenic vessels, tail of pancreas |
| **Transverse mesocolon** | Transverse colon ↔ Posterior body wall (pancreas) | Middle colic vessels |
| **Sigmoid mesocolon** | Sigmoid colon ↔ Pelvic wall | Sigmoid vessels; apex overlies left ureter |
| **Mesentery proper** | Small intestine ↔ Posterior body wall | SMA/SMV branches, 400+ lymph nodes, nerves, fat |
| **Mesoappendix** | Appendix ↔ Ileal mesentery | Appendicular artery (end artery) |
| **Coronary ligament** | Liver ↔ Diaphragm | Encloses bare area of liver |
| **Broad ligament** | Uterus ↔ Pelvic wall | Uterine tubes, round ligament, ovarian ligament, uterine artery, ureter |
---
## PART 9: APPLIED ANATOMY – SURGICAL APPROACHES
### 9.1 Laparoscopy
- **CO₂ pneumoperitoneum** is created (12-15 mmHg pressure) to distend the peritoneal cavity and create a working space. CO₂ is used because it is non-combustible, rapidly absorbed, and does not support combustion (safe with electrocautery).
- **Veress needle** is inserted (usually at the umbilicus — the thinnest part of the abdominal wall) to insufflate CO₂. Alternatively, **open (Hasson) technique** is used (mini-incision → direct entry under vision).
- **Palmer's point** (left hypochondrium, midclavicular line, below the costal margin) is an alternative site for initial access when umbilical adhesions are expected (previous surgery).
- **Complications of pneumoperitoneum:**
- Gas embolism (rare but potentially fatal)
- Subcutaneous emphysema (CO₂ in subcutaneous tissue)
- Shoulder tip pain (CO₂ irritating the diaphragmatic peritoneum → phrenic nerve referral)
- Cardiac arrhythmias (CO₂ absorption → hypercarbia)
- Decreased venous return (increased intra-abdominal pressure compresses the IVC)
- Bowel or vascular injury during trocar insertion
### 9.2 Peritoneal Lavage/Washout
- Used during surgery for peritonitis: copious irrigation of all peritoneal spaces (subphrenic, subhepatic, paracolic gutters, pelvis, lesser sac) with warm saline to remove contamination.
- Reduces bacterial load and helps prevent abscess formation.
### 9.3 Peritoneal Drains
- After contaminated or high-risk surgeries, drains may be left in specific peritoneal spaces to allow egress of fluid/blood/bile.
- Types: closed suction drains (Jackson-Pratt, Blake), Penrose drains (open), sump drains.
- Common drain locations: Morison's pouch, pelvis (Douglas), subphrenic spaces, lesser sac.
---
## PART 10: MISCELLANEOUS CLINICAL CORRELATIONS
### 10.1 Hernia Types Related to Peritoneum
| Hernia Type | Relationship to Peritoneum | Notes |
|---|---|---|
| **Inguinal (indirect)** | Hernia sac is peritoneum (persistent processus vaginalis) | Through deep ring, lateral to inferior epigastric vessels |
| **Inguinal (direct)** | Hernia sac is peritoneum through weakened posterior wall | Through Hesselbach's triangle, medial to inferior epigastric vessels |
| **Femoral** | Peritoneal sac enters femoral canal | Below inguinal ligament, medial to femoral vein. Highest risk of strangulation |
| **Umbilical** | Peritoneal sac protrudes through umbilical ring | Common in neonates (physiologic), adults (obesity, ascites, pregnancy) |
| **Incisional** | Peritoneal sac protrudes through previous surgical incision | Risk factors: obesity, wound infection, poor surgical technique |
| **Paraduodenal (internal)** | Bowel enters paraduodenal fossae | Most common internal hernia |
| **Foramen of Winslow (internal)** | Bowel enters lesser sac through epiploic foramen | Very rare internal hernia |
| **Obturator** | Peritoneal sac enters obturator canal | **Howship-Romberg sign** (pain along inner thigh due to compression of obturator nerve). Often in elderly, thin females |
| **Richter's hernia** | Only antimesenteric wall of bowel herniates | Can strangulate without complete obstruction |
| **Littre's hernia** | Meckel's diverticulum in the hernia sac | Any hernia can be a Littre's hernia |
### 10.2 Peritoneal Signs in Specific Conditions
| Sign | Description | Condition |
|---|---|---|
| **McBurney's sign** | Tenderness at McBurney's point (1/3 from ASIS to umbilicus) | Appendicitis |
| **Rovsing's sign** | LIF palpation → RIF pain | Appendicitis |
| **Psoas sign** | Pain on extension of right hip | Retrocecal appendicitis (or psoas abscess) |
| **Obturator sign** | Pain on internal rotation of flexed right hip | Pelvic appendicitis |
| **Murphy's sign** | Arrest of inspiration during RUQ palpation | Acute cholecystitis |
| **Kehr's sign** | Left shoulder tip pain | Splenic rupture (blood irritating left hemidiaphragm) |
| **Blumberg's sign** | Rebound tenderness | Peritoneal irritation (any cause) |
| **Cullen's sign** | Periumbilical ecchymosis | Hemoperitoneum, acute pancreatitis, ruptured ectopic pregnancy |
| **Grey Turner's sign** | Flank ecchymosis | Retroperitoneal hemorrhage (pancreatitis) |
| **Fox's sign** | Ecchymosis of the inguinal ligament | Retroperitoneal hemorrhage |
| **Dance's sign** | Empty RIF | Ileocecal intussusception (mass has moved) |
| **Carnett's sign** | Tenderness increases with tensing of abdominal muscles | Abdominal wall pathology (not intra-abdominal) |
| **Chandelier sign** | Extreme cervical motion tenderness (patient "hits the chandelier") | PID/peritonitis from pelvic source |
| **Sister Mary Joseph nodule** | Palpable umbilical nodule | Metastatic intra-abdominal cancer |
| **Blumer's shelf** | Hard mass palpable on DRE (anterior rectal wall) | Metastatic deposits in pouch of Douglas |
### 10.3 Peritoneal Fluid Analysis
When paracentesis is performed, the ascitic fluid is analyzed:
| Test | Transudative | Exudative |
|---|---|---|
| Protein | <2.5 g/dL | >2.5 g/dL |
| SAAG | ≥1.1 g/dL | <1.1 g/dL |
| Cell count | Low WBC (<250 PMNs/mm³) | High WBC (>500/mm³; PMNs >250 in SBP) |
| LDH | Low | High |
| Glucose | Normal | Low (TB, malignancy) |
| ADA | Normal | High (tuberculosis) |
| Amylase | Normal | High (pancreatic ascites) |
| Triglycerides | Normal | High (>200 mg/dL in chylous ascites) |
| Cytology | Negative | Positive in malignancy (~60-90% sensitivity for peritoneal carcinomatosis) |
| Culture | Negative | Positive in infection (monomicrobial in SBP, polymicrobial in secondary peritonitis) |
---
## CONCLUSION
The anatomy of the abdominal cavity and peritoneum is fundamental to understanding abdominal pathology, surgical approaches, and clinical reasoning. The key concepts include:
1. **The peritoneum is a continuous serous membrane** forming parietal and visceral layers.
2. **Peritoneal spaces** (subphrenic, subhepatic, paracolic gutters, pelvic pouches) are clinically important as sites of fluid collection and abscess formation.
3. **Nerve supply differs** between parietal (somatic, well-localized) and visceral (autonomic, poorly localized, referred) peritoneum, explaining the clinical patterns of abdominal pain.
4. **Mesenteries, omenta, and ligaments** are double layers of peritoneum that convey vessels and nerves and define the anatomical relationships of organs.
5. **The organ's relationship to the peritoneum** (intraperitoneal, retroperitoneal, subperitoneal) determines surgical approach, mobility, and clinical presentation.
6. **The lesser sac** communicates with the greater sac only through the **epiploic foramen** and is clinically relevant in pancreatic and gastric pathology.
7. **Fluid follows predictable pathways** through the peritoneal cavity, explaining the distribution of abscesses and metastatic deposits.
This comprehensive understanding of peritoneal anatomy underpins safe surgical practice, accurate clinical diagnosis, and effective management of abdominal diseases.
Rewrite the whole content as it is plus add maximum number of high yield images along the content from your side