Kindly make MD Anaesthesiology exam notes on approach towards an uncouncious patient
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
MD Anaesthesiology Exam Notes
Approach Towards an Unconscious Patient
1. DEFINITIONS & SPECTRUM OF CONSCIOUSNESS
| Term | Description |
|---|---|
| Consciousness | State of awareness of self and environment requiring intact arousal (ARAS) + cognition (cortex) |
| Lethargy | Reduced wakefulness; arousable with stimulation, responds appropriately |
| Obtundation | Reduced alertness; less responsive to environment; reduced interest in surroundings |
| Stupor | Responds only to vigorous/painful stimuli; returns to unresponsive state when stimulation ceases |
| Coma | No purposeful response to external stimuli or inner needs; GCS ≤ 8 |
| Vegetative State | Wakefulness without awareness (eyes open); brainstem intact; cortex nonfunctional |
| Locked-In State | Full awareness but complete paralysis; only vertical eye movements and blinking preserved — pseudocoma (basilar artery thrombosis, pontine infarction, severe Guillain-Barré) |
| Brain Death | Irreversible cessation of all cerebral and brainstem function |
Almost all coma traces to (1) widespread bihemispherical dysfunction or (2) suppression of the reticular activating system (RAS) in the upper brainstem/thalamus. — Harrison's Principles of Internal Medicine 22E
2. IMMEDIATE PRIORITIES (BEFORE ANYTHING ELSE)
A–B–C–D–E: The Anaesthetist's Primary Survey
"It is never justified to delay attending to the basics of airway, breathing, and circulation while performing a more elaborate scoring evaluation." — Plum & Posner's Diagnosis and Treatment of Stupor and Coma
| Priority | Action |
|---|---|
| A — Airway | Open/clear airway; jaw thrust / chin lift; suction; early intubation if GCS ≤ 8 or loss of protective reflexes |
| B — Breathing | Assess rate, depth, pattern; SpO₂; supplemental O₂ / assisted ventilation as needed |
| C — Circulation | HR, BP, IV access × 2; cardiac monitor; treat shock, arrhythmia |
| D — Disability | GCS, pupil size & reactivity, posturing, blood glucose (BGL) |
| E — Exposure | Full exposure; temperature; signs of trauma/injection marks/rash |
Empiric IV "coma cocktail" (when cause unknown and IV access secured):
- Dextrose 50% 50 mL IV (after checking glucose; treat hypoglycaemia empirically in resource-limited settings)
- Thiamine 100 mg IV (before or with dextrose to prevent Wernicke's encephalopathy)
- Naloxone 0.4–2 mg IV (if opioid overdose suspected)
- Flumazenil (if benzodiazepine overdose — use cautiously in polypharmacy/epilepsy)
3. AIRWAY MANAGEMENT IN THE UNCONSCIOUS PATIENT
| Situation | Action |
|---|---|
| GCS ≤ 8 / absent gag reflex | Definitive airway — Rapid Sequence Intubation (RSI) |
| Cervical spine not cleared (trauma) | Maintain manual in-line stabilisation (MILS) during laryngoscopy; assume spinal injury |
| Full stomach / aspiration risk | RSI with cricoid pressure (Sellick's), suction ready |
| Difficult airway anticipated | Video laryngoscopy, surgical airway backup plan |
RSI Drug Sequence
- Pre-oxygenate 3–5 min 100% O₂
- Pre-treatment (optional): Fentanyl 1–3 µg/kg, Atropine in children/bradycardia
- Induction: Ketamine 1–2 mg/kg (haemodynamically unstable) OR Thiopentone 3–5 mg/kg (raised ICP) OR Propofol 1–2 mg/kg (haemostable)
- Cricoid pressure applied
- Paralysis: Succinylcholine 1.5 mg/kg IV (preferred, fastest onset) OR Rocuronium 1.2 mg/kg (if succinylcholine contraindicated)
- Laryngoscopy & intubation; confirm with waveform capnography
- Release cricoid pressure after cuff inflation confirmed
Succinylcholine contraindications in unconscious patients: crush injuries >72 h, burns >72 h, denervation injuries, hyperkalemia, known malignant hyperthermia susceptibility.
4. CLINICAL ASSESSMENT
4a. History (from relatives/witnesses/EMS)
- Onset: sudden (vascular/trauma) vs subacute (metabolic/infection)
- Preceding symptoms: headache, seizure, fever, focal deficit, vomiting
- Medical history: diabetes, epilepsy, liver/renal disease, hypertension, psychiatric illness
- Drug history: prescribed medications, recreational drugs, alcohol
- Circumstances: found alone, near medications, trauma scene, hospital setting
4b. Level of Consciousness Scales
AVPU Scale (Rapid Bedside Tool)
- A — Alert and oriented
- V — Responds to Voice
- P — Responds to Pain
- U — Unresponsive
Glasgow Coma Scale (GCS)
| Domain | Response | Score |
|---|---|---|
| Eye Opening | Spontaneous | 4 |
| To voice | 3 | |
| To pressure/pain | 2 | |
| None | 1 | |
| Verbal | Oriented | 5 |
| Confused | 4 | |
| Words only | 3 | |
| Sounds | 2 | |
| None | 1 | |
| Motor | Obeys commands | 6 |
| Localises pain | 5 | |
| Normal flexion (withdrawal) | 4 | |
| Abnormal flexion (decorticate) | 3 | |
| Extension (decerebrate) | 2 | |
| None | 1 |
- GCS ≤ 8 = severe brain injury → secure airway
- 9–12 = moderate; 13–15 = mild — Miller's Anesthesia 10e; Plum & Posner
FOUR Score (Full Outline of Unresponsiveness)
Preferred in intubated patients where verbal score cannot be assessed.
| Domain | Score (0–4) |
|---|---|
| Eye response | 4 = tracking/blinking to command → 0 = no response to pain |
| Motor response | 4 = thumbs-up/fist/peace sign → 0 = no response |
| Brainstem reflexes | 4 = pupil + corneal present → 0 = all absent (inc. cough) |
| Respiration | 4 = not intubated, regular → 0 = breathes at vent rate / apnoea |
— Plum & Posner's Diagnosis and Treatment of Stupor and Coma
4c. General Physical Examination
| Finding | Significance |
|---|---|
| Fever | Infection (meningitis, encephalitis, sepsis), heat stroke, neuroleptic malignant syndrome, malignant hyperthermia |
| Hypothermia | Exposure, alcohol/barbiturate/sedative/phenothiazine OD, hypoglycaemia, severe hypothyroidism; coma occurs at <31°C |
| Hypertension | Hypertensive encephalopathy, PRES, Cushing's response (raised ICP), eclampsia |
| Hypotension | Alcohol/barbiturate OD, internal haemorrhage, MI/cardiac failure, sepsis, Addisonian crisis |
| Tachypnoea | Metabolic acidosis, pneumonia, aspiration |
| Skin | Cyanosis (hypoxia), cherry-red (CO poisoning), jaundice (hepatic coma), petechiae (TTP/meningococcaemia/DIC), needle tracks (IV drug use), tongue bites (seizures) |
| Odour | Alcohol, ketones (DKA), fetor hepaticus (hepatic failure), uraemic fetor |
| Head signs | Battle's sign (mastoid ecchymosis), raccoon eyes, CSF rhinorrhoea/otorrhoea, haemotympanum → base of skull fracture |
| Fundoscopy | Papilloedema (raised ICP), subhyaloid haemorrhage (SAH), hypertensive changes |
| Neck stiffness | Meningitis, SAH (note: absent in deep coma even with meningitis!) |
4d. Neurological Examination
Pupils
The most important sign in coma localisation:
| Pupil Finding | Localisation/Cause |
|---|---|
| Bilaterally small (miotic), reactive | Metabolic, opioid OD, pontine (bilateral pontine haemorrhage — "pinpoint") |
| Bilaterally mid-dilated (4–5 mm), fixed | Midbrain damage |
| Unilaterally dilated, fixed ("blown pupil") | Uncal herniation compressing CN III ipsilateral to mass |
| Bilaterally large, fixed | Severe anoxia, atropine/anticholinergic OD |
| Small, reactive | Metabolic/toxic (intact brainstem) |
| Anisocoria (new) | Structural intracranial pathology until proven otherwise |
CNS-depressant drugs lose corneal responses before pupils become unreactive to light. Preserved pupillary responses strongly suggest a metabolic cause. — Harrison's Principles of Internal Medicine 22E
Ocular Movements
| Test | Technique | Interpretation |
|---|---|---|
| Doll's Eye Reflex (Oculocephalic) | Brisk horizontal head rotation; eyes should deviate opposite direction | Absent in brainstem damage (eyes move with head); Present = intact brainstem |
| Cold Caloric Testing (Oculovestibular) | Cold water 30–50 mL in external auditory canal | Normal awake: nystagmus away from side. Coma with intact brainstem: tonic conjugate deviation toward cold. Absent: brainstem dysfunction |
| Spontaneous movements | Roving eye movements | Intact brainstem, metabolic cause likely |
| Ocular bobbing | Brisk downward then slow return | Pontine haemorrhage |
| Sustained deviation | Eyes deviate toward side of lesion | Frontal/hemisphere lesion (away from hemiplegia) |
Respiratory Patterns in Coma
| Pattern | Cause |
|---|---|
| Cheyne-Stokes (crescendo-decrescendo with apnoea) | Bihemispherical damage, metabolic suppression, CHF |
| Central Neurogenic Hyperventilation (deep, rapid — Kussmaul) | Pontomesencephalic lesions OR metabolic acidosis (DKA, uraemia) |
| Apneusis (prolonged inspiratory cramps) | Pontine infarction |
| Cluster breathing | Lower pontine/upper medullary lesion |
| Ataxic/Agonal gasping | Lower medullary damage; terminal |
| Slow, shallow, regular | Metabolic or drug-induced depression of medullary centres |
| Posthyperventilation apnoea | Diffuse bihemispherical or frontal lobe damage |
— Plum & Posner's Diagnosis and Treatment of Stupor and Coma
Motor Examination
| Finding | Significance |
|---|---|
| Decorticate posturing (flexion elbows/wrists, supination) | Bilateral damage rostral to midbrain |
| Decerebrate posturing (extension elbows/wrists, pronation) | Damage to motor tracts caudal to midbrain |
| Flaccidity + absent reflexes | Deep coma, medullary failure, spinal shock |
| Hemiplegia | Contralateral hemisphere lesion |
| Multifocal myoclonus | Metabolic encephalopathy (uremia, hypoxia, drug OD) |
| Asterixis (bilateral) | Metabolic encephalopathy, drug intoxication |
5. DIFFERENTIAL DIAGNOSIS OF COMA
Mnemonic: "AEIOU TIPS"
| Letter | Causes |
|---|---|
| A — Alcohol / Acidosis | Alcohol intoxication, DKA, lactic acidosis |
| E — Epilepsy | Post-ictal state, non-convulsive status epilepticus (NCSE) |
| I — Insulin / Ions | Hypoglycaemia, hyperglycaemia (HHS/DKA), Na⁺, Ca²⁺, Mg²⁺ disorders |
| O — Overdose / O₂ | Drug OD (opioids, benzodiazepines, TCAs), CO poisoning, hypoxia |
| U — Uraemia | Renal failure, hepatic failure (hepatic encephalopathy) |
| T — Trauma | TBI, subdural/epidural haematoma, diffuse axonal injury |
| I — Infection | Meningitis, encephalitis, septic encephalopathy, cerebral abscess |
| P — Psychiatric / Poisoning | Functional unresponsiveness, serotonin syndrome, NMS |
| S — Stroke / Structural | ICH, ischaemic stroke, SAH, posterior fossa lesions, hydrocephalus |
Formal Classification (Harrison's Principles of Internal Medicine 22E)
Category 1 — No focal neurological signs (CT often normal):
- Intoxications: alcohol, sedatives, opioids
- Metabolic: anoxia, hypoglycaemia, hyperglycaemia, hypo/hypernatraemia, hypercalcaemia, uraemia, hepatic failure, Addisonian crisis, thyroid disorders
- Severe systemic infection: septicaemia, pneumonia, typhoid, malaria
- Shock (any cause)
- Status epilepticus / post-ictal
- Hypertensive encephalopathy / PRES / eclampsia
- Hyperthermia / hypothermia
- Concussion, acute hydrocephalus
Category 2 — Focal brainstem or lateralising signs (CT typically abnormal):
- Basal ganglia/thalamic haemorrhage, large MCA infarction
- Basilar artery thrombosis
- Brainstem infarction
- Brain abscess, subdural empyema
- Epidural/subdural haemorrhage, cerebral contusion
- Brain tumour with oedema
- Cerebellar/pontine haemorrhage or infarction
- Diffuse traumatic brain injury
Category 3 — Meningeal irritation ± fever, CSF abnormality:
- Subarachnoid haemorrhage (sudden severe headache + collapse)
- Bacterial meningitis, encephalitis
- Paraneoplastic/autoimmune encephalitis
- Carcinomatous meningitis
6. INVESTIGATIONS
Immediate (Bedside/Point-of-Care)
- Blood glucose (fingerprick — treat hypoglycaemia immediately)
- SpO₂, ABG (acid-base, PaO₂, PaCO₂)
- ECG (arrhythmia, ischaemia)
- 12-lead ECG + continuous monitoring
Urgent Bloods
- Full blood count (infection, anaemia)
- Urea, creatinine, electrolytes (Na⁺, K⁺, Ca²⁺, Mg²⁺, phosphate)
- Liver function tests + ammonia
- Blood glucose, HbA1c
- Thyroid function (TFTs)
- Serum osmolality
- Coagulation (PT, APTT, INR)
- Blood cultures (if febrile)
- Toxicology screen (blood + urine)
- Cortisol (if Addisonian crisis suspected)
- Lactate
Neuroimaging
- CT head (non-contrast) — FIRST LINE: haemorrhage, mass lesion, herniation, hydrocephalus
- Normal CT does not exclude: early bilateral infarction, brainstem infarction, encephalitis, axonal shearing, hypoxic injury, isodense subdural
- MRI Brain (+ DWI) — superior for posterior fossa, early ischaemia, diffuse axonal injury
- CT Angiography — if posterior circulation stroke suspected
CSF Analysis (Lumbar Puncture)
- Indicated: meningism, fever + no focal signs, SAH with normal CT
- Contraindicated: mass lesion / raised ICP, coagulopathy, overlying skin infection
- Test: opening pressure, cells (WBC/RBC), protein, glucose (paired serum glucose), Gram stain, culture, xanthochromia
EEG
- Essential for non-convulsive status epilepticus (NCSE)
- Metabolic coma: generalised slow δ or triphasic waves (frontal in hepatic failure)
- Sedative OD: diffuse fast β activity
- Herpes encephalitis: periodic lateralised epileptiform discharges (PLEDs)
- "Alpha coma" (unresponsive α): post-cardiac arrest, brainstem infarction — poor prognosis
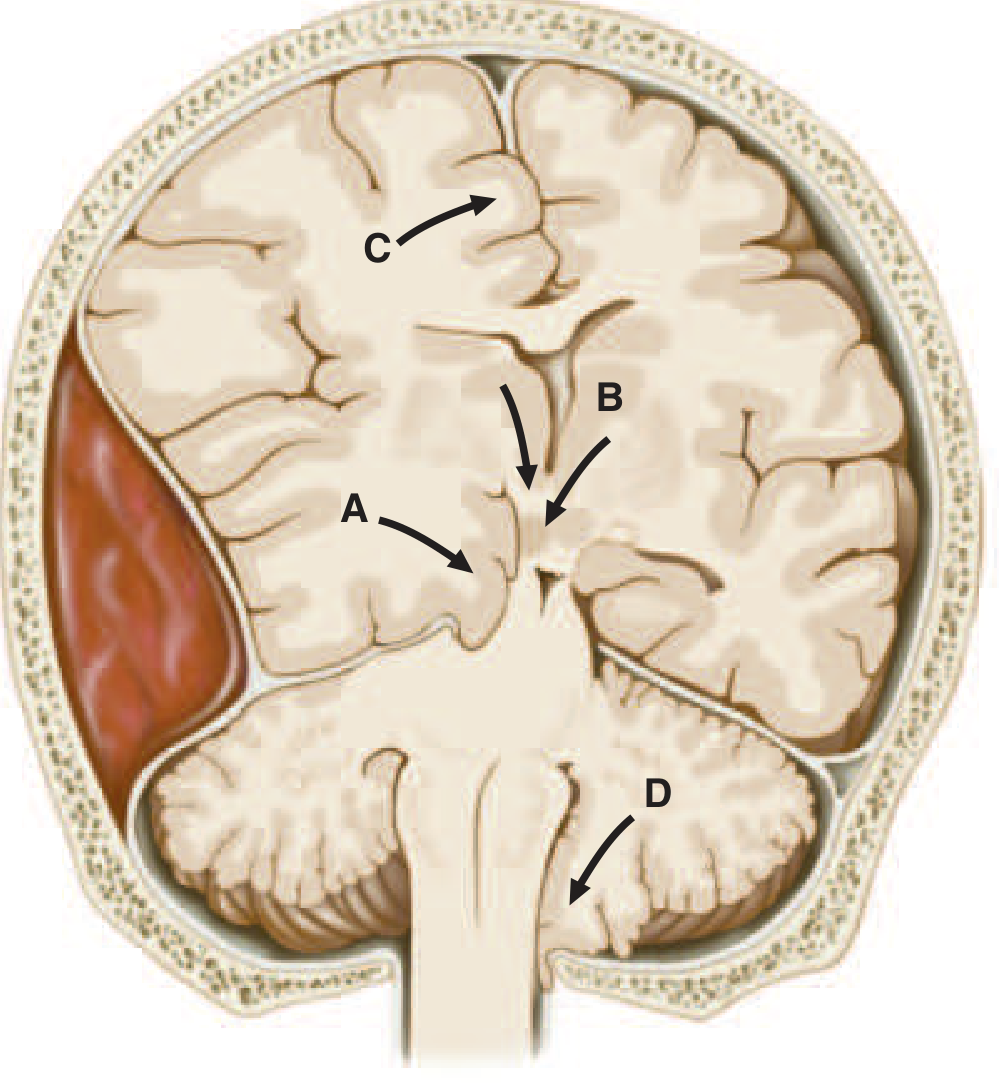
7. HERNIATION SYNDROMES
| Type | Mechanism | Clinical Features |
|---|---|---|
| Uncal (transtentorial) | Medial temporal lobe pushed through tentorial notch | Ipsilateral CN III palsy (blown pupil) → contralateral hemiplegia; later bilateral signs |
| Central | Downward displacement of diencephalon through tentorium | Small reactive pupils → decorticate → decerebrate posturing; Cheyne-Stokes → central hyperventilation |
| Transfalcial (subfalcine) | Cingulate gyrus under falx | Leg weakness contralateral; ACA compression |
| Foraminal (tonsillar) | Cerebellar tonsils through foramen magnum | Sudden apnoea, bradycardia, death — most dangerous |
8. RAISED INTRACRANIAL PRESSURE (ICP) MANAGEMENT
Cushing's Triad: Hypertension + Bradycardia + Irregular respiration → sign of impending herniation
Principles
- Cerebral Perfusion Pressure (CPP) = MAP − ICP; target CPP 60–70 mmHg
- Normal ICP: ≤ 15 mmHg; treat if > 20–22 mmHg
Immediate Measures
- HOB 30°, head in neutral position
- Ensure adequate oxygenation/ventilation; target PaO₂ > 60 mmHg, PaCO₂ 35–40 mmHg (avoid hypercapnia)
- Avoid hypotension — maintain adequate MAP
- Treat hyperthermia, seizures, pain/agitation
- Mannitol 20% 0.25–1 g/kg IV bolus (osmotic agent)
- Hypertonic saline 3% NaCl (alternative to mannitol)
- Avoid glucose-containing fluids (worsen cerebral oedema)
- Dexamethasone (only for oedema around tumours/abscesses; NOT for TBI or stroke)
- Hyperventilation to PaCO₂ 30–35 mmHg — temporising only (causes vasoconstriction)
- CSF drainage via external ventricular drain (EVD) if available
- Decompressive craniectomy (surgical option)
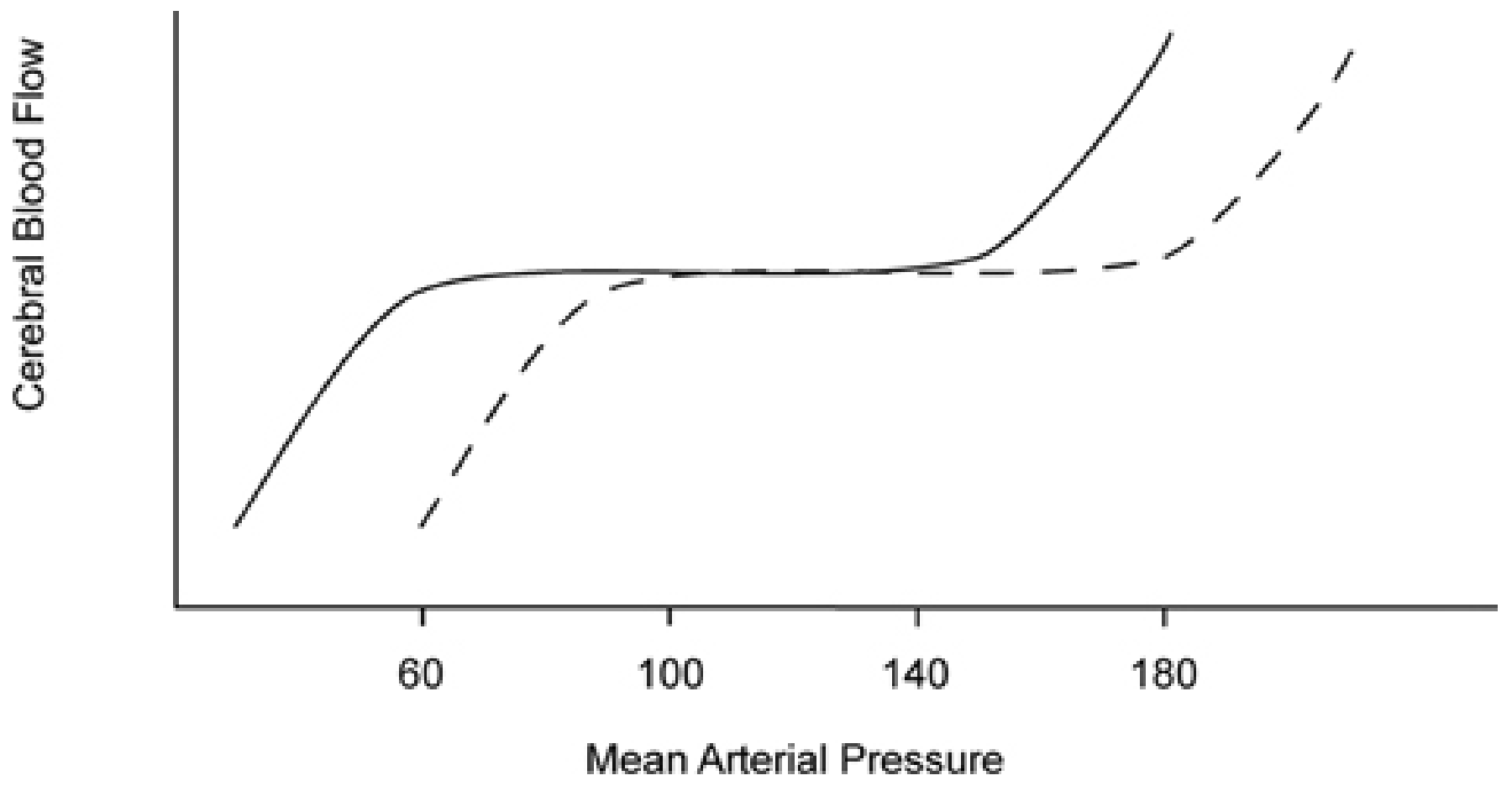
9. CEREBRAL AUTOREGULATION
- Normal range: MAP 50–150 mmHg — CBF remains constant
- Chronic hypertension: autoregulatory curve shifts right → risk of ischaemia at "normal" blood pressures
- Below lower limit → CBF ∝ MAP → ischaemia
- Above upper limit → hyperaemia → hypertensive encephalopathy, PRES
Anaesthetic relevance: in the unconscious/comatose patient, autoregulation is often impaired. Avoid hypotension or extreme hypertension.
10. SPECIFIC CAUSES — ANAESTHETIC MANAGEMENT PEARLS
Hypoglycaemia
- BGL < 3 mmol/L: 50% dextrose 50 mL IV → recheck
- Follow with 10% dextrose infusion; monitor regularly
Opioid Overdose
- Miosis, respiratory depression, bradycardia
- Naloxone 0.4–2 mg IV (q2–3 min, titrate); short half-life → repeat doses/infusion needed
- Airway support/intubation if severe
Benzodiazepine Overdose
- Flumazenil 0.2 mg IV (q1 min up to 1 mg) — caution in epileptics, chronic BZD users (precipitates seizures)
Status Epilepticus / NCSE
- Lorazepam 0.1 mg/kg IV OR diazepam 0.1–0.2 mg/kg IV
- If refractory: phenytoin/fosphenytoin, levetiracetam, sodium valproate
- Refractory SE: ICU admission, propofol/midazolam/thiopentone infusion
- EEG monitoring mandatory in intubated patients
Hepatic Encephalopathy
- Avoid hepatotoxic drugs; reduce nitrogen load (lactulose, rifaximin)
- Correct precipitants (GI bleed, infection, electrolyte disturbance)
- Airway protection often required in Grade III–IV
Meningitis/Encephalitis
- Dexamethasone 0.15 mg/kg IV then empiric antibiotics (ceftriaxone ± ampicillin ± acyclovir)
- Do NOT delay antibiotics for CT/LP if high suspicion
Diabetic Ketoacidosis / HHS
- Fluid resuscitation first (0.9% NaCl)
- Insulin infusion, electrolyte replacement
- Avoid rapid correction of glucose/sodium (cerebral oedema risk)
Eclampsia
- MgSO₄ 4–6 g IV loading, 1–2 g/hr maintenance
- Control BP: labetalol, hydralazine, nifedipine
- Airway: RSI with thiopentone, suxamethonium
- Deliver fetus
11. BRAIN DEATH
Prerequisites (confounders must be excluded)
- Core temperature > 36°C
- No drug/sedative effect
- No metabolic derangement (Na⁺, glucose, acid-base)
- No neuromuscular blocking agents
- Circulatory stability
Clinical Criteria
- Deep coma: unresponsive to all stimuli
- Fixed dilated pupils (usually mid-sized; may be dilated)
- Absent corneal reflexes bilaterally
- Absent oculovestibular reflexes (caloric testing)
- Absent gag and cough reflexes
- Apnoea test: PaCO₂ rises to >60 mmHg (>8 kPa) with no respiratory effort
- Pre-oxygenate 100% O₂; disconnect ventilator; deliver O₂ at 6 L/min via catheter
- PaCO₂ rises ~2–3 mmHg/min; observe for 8–10 minutes
Ancillary Tests (where clinical testing incomplete)
- EEG (isoelectric/electrocerebral silence)
- Cerebral angiography (no intracranial flow)
- CT/MRI angiography
- Transcranial Doppler (absent flow/reverberant pattern)
- Nuclear scan (no cerebral perfusion)
"Brain death is the only type of brain damage recognised as morally, ethically, and legally equivalent to death." — Harrison's Principles of Internal Medicine 22E
12. MONITORING IN THE UNCONSCIOUS PATIENT (ANAESTHETIC/ICU)
| Parameter | Monitoring Tool |
|---|---|
| Neurological status | Serial GCS/FOUR score, pupillary checks |
| Intracranial pressure | ICP monitor (EVD, parenchymal probe) |
| Cerebral oxygenation | Jugular venous bulb oximetry (SjO₂), NIRS |
| EEG/seizure surveillance | Continuous EEG in ICU (especially post-cardiac arrest, NCSE risk) |
| Airway | Waveform capnography (ETCO₂), CXR post-intubation |
| Haemodynamics | Arterial line, CVP, cardiac output monitoring |
| Temperature | Core temperature (target normothermia or therapeutic hypothermia post-cardiac arrest) |
| Metabolic | Hourly BGL, daily electrolytes, ABG |
13. FLOWCHART SUMMARY
UNCONSCIOUS PATIENT
│
▼
CALL FOR HELP + START TIMER
│
▼
PRIMARY SURVEY (ABCDE)
├─ Airway: Open + protect (intubate if GCS ≤ 8)
├─ Breathing: O₂, ventilation
├─ Circulation: IV access, fluids, monitoring
├─ Disability: GCS, pupils, BGL
└─ Exposure: trauma signs, temp, rash
│
▼
EMPIRICAL TREATMENT
(Dextrose + Thiamine + Naloxone)
│
▼
HISTORY + EXAMINATION
(Focused neurological exam)
│
▼
INVESTIGATIONS
(Bloods + CT head ± LP ± EEG)
│
▼
DIAGNOSIS → SPECIFIC TREATMENT
(Structural / Metabolic / Toxic / Infectious)
│
▼
ICU ADMISSION + ONGOING MONITORING
KEY EXAM POINTS (High-Yield)
- GCS ≤ 8 = intubate; always document GCS before sedation/paralysis
- The most common cause of coma is metabolic/toxic — not structural
- Preserved pupillary reflexes strongly suggest metabolic coma (structural causes typically impair pupils)
- Never withhold glucose + thiamine in undifferentiated coma
- Always exclude and treat hypoglycaemia first — it is the most easily reversible cause
- Herniation: ipsilateral blown pupil → uncal herniation; treat as emergency
- Succinylcholine is the fastest-onset paralytic for RSI but check K⁺ and contraindications in trauma
- Hyperventilation is only a temporising measure for raised ICP (lasts <30 min)
- Brain death apnoea test: PaCO₂ must exceed 60 mmHg — not simply "high"
- Normal CT does not exclude encephalitis, axonal injury, posterior fossa infarction, isodense subdural
Sources: Harrison's Principles of Internal Medicine 22E | Plum & Posner's Diagnosis and Treatment of Stupor and Coma | Miller's Anesthesia 10e | Bailey & Love's Short Practice of Surgery 28e
This is a shared conversation. Sign in to Orris to start your own chat.