Lbbb ecg
Reading File
Finding Sources
Searching Images
LBBB left bundle branch block ECG
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Now I have comprehensive information. Let me compile a thorough response.
Left Bundle Branch Block (LBBB) on ECG
Pathophysiology
In LBBB, the left bundle branch fails to conduct, so the right ventricle depolarizes first via the normal His-Purkinje pathway, then ventricular activation spreads slowly cell-to-cell leftward through the myocardium rather than the fast conduction system. This produces a wide, abnormal QRS and abnormal repolarization (ST-T discordance).
ECG Diagnostic Criteria
| Feature | Finding |
|---|---|
| QRS duration | ≥ 120 ms (≥ 0.12 sec) — mandatory |
| V1 morphology | rS or QS pattern — deep, broad S-waves (or entirely negative) |
| Lateral leads (I, aVL, V5–V6) | Broad, monophasic, notched R-wave — no septal Q wave |
| ST segments & T waves | Discordant in V1–V6 (opposite direction to QRS vector) |
| Axis | Variable |
Key mnemonic: "WiLLiaM" — in LBBB, W-shape in V1, M-shape in V5/V6.
The absence of a septal Q wave in leads I, aVL, and V6 is a defining criterion that distinguishes true LBBB from nonspecific intraventricular conduction delay (IVCD). — Fuster and Hurst's The Heart, 15th Ed.
ECG Examples
Classic LBBB — 12-lead ECG from a cardiac stress test:
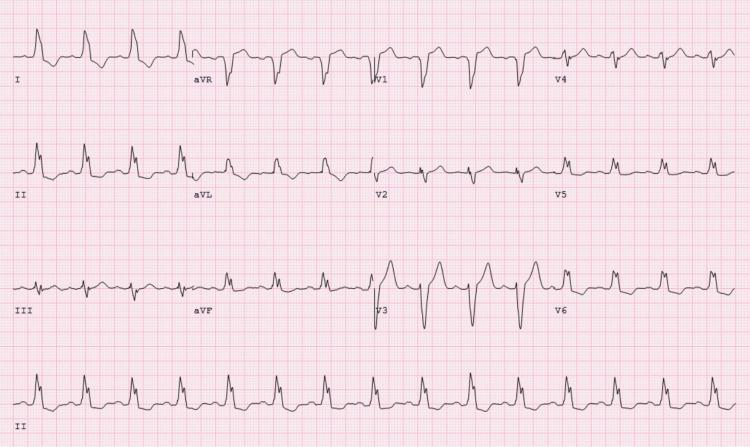
Features: Sinus tachycardia, QRS >120 ms, deep S-waves V1–V3, broad monophasic R-waves in leads I/aVL/V5/V6, discordant ST-T changes in lateral leads.
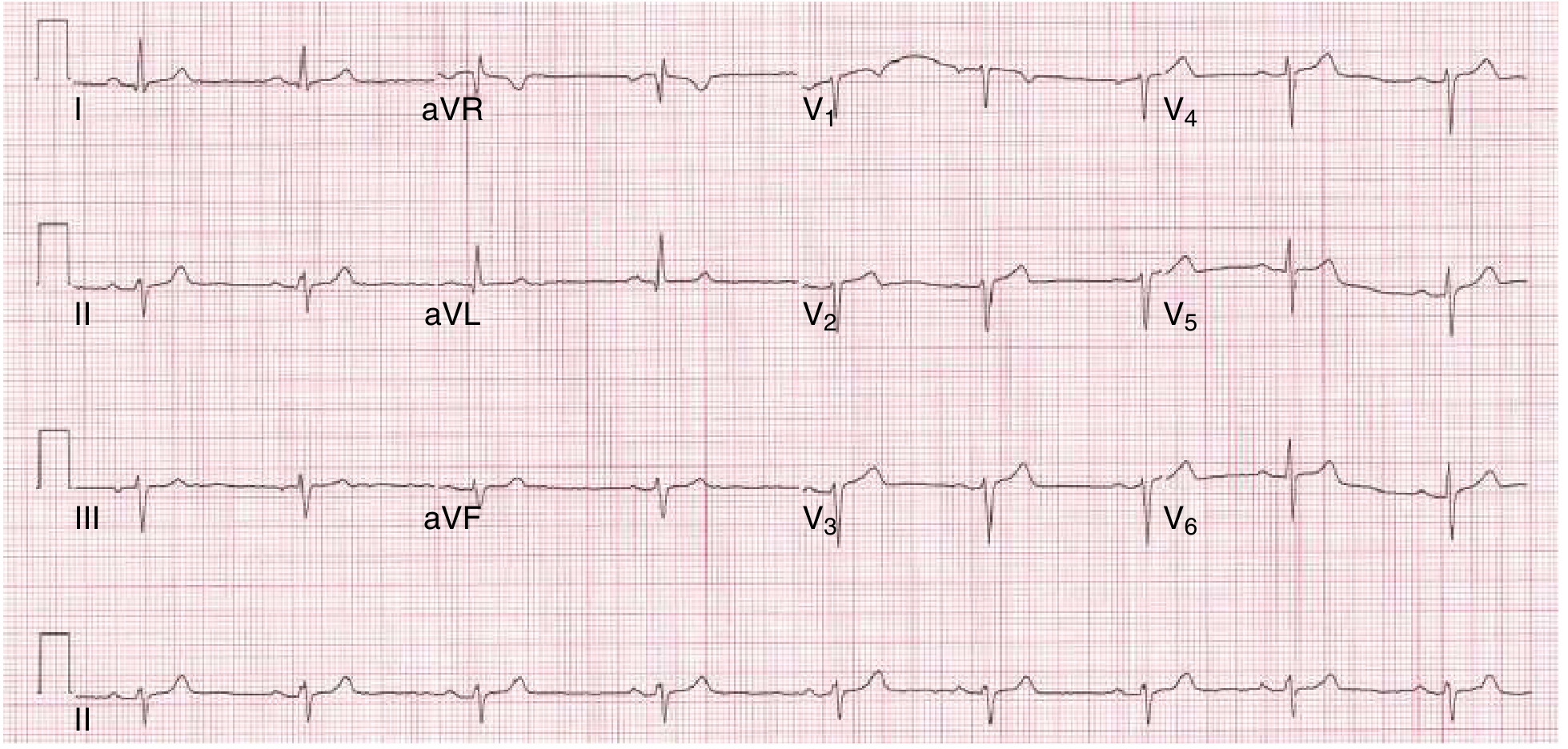
LBBB from Goldman-Cecil Medicine textbook:
Etiology & Clinical Significance
Common causes:
- Ischemia or myocardial infarction
- Left ventricular hypertrophy / LV dilation
- Fibrosis of the conduction system (e.g., Lenegre's/Lev's disease)
- Severe cardiac trauma
- Cardiomyopathy
Prognostic significance:
- In young, asymptomatic patients — weak predictive value (Bayes' theorem)
- In older patients — ominous marker for increased risk of death, stroke, and CHF
- Incomplete LBBB and hemiblocks are usually NOT associated with cardiac disease — Pfenninger & Fowler's Procedures for Primary Care
LBBB and Acute MI — The Critical Overlap
LBBB masks ST-segment analysis and complicates diagnosis of acute MI. Use the Sgarbossa Criteria (GUSTO trial):
| Criterion | Threshold | Score | Specificity |
|---|---|---|---|
| ST elevation concordant with QRS | ≥ 1 mm | 5 | Highest |
| ST depression in V1–V3 | ≥ 1 mm | 3 | High |
| ST elevation discordant with QRS | ≥ 5 mm | 2 | Lower alone |
A score ≥ 3 achieves ~90% specificity for AMI. — Rosen's Emergency Medicine
Modified Sgarbossa criteria (more sensitive): replaces the third criterion with an ST/S ratio > 0.25 (excessive discordance). This improves sensitivity without meaningful loss of specificity.
Clinical rule: New or presumed new LBBB in a patient with ischemic chest pain = treat as STEMI — immediate reperfusion (PCI preferred, or thrombolysis if PCI unavailable). However, new LBBB alone without Sgarbossa-positive features has <10% AMI rate. — Tintinalli's Emergency Medicine; Goldman-Cecil Medicine
Comparison: LBBB vs RBBB
| Feature | LBBB | RBBB |
|---|---|---|
| QRS duration | ≥ 120 ms | ≥ 120 ms |
| V1 morphology | rS or QS (deep negative) | rsr'/rsR' ("rabbit ears") |
| Lateral leads | Broad R, no Q wave | Wide S wave |
| ST/T discordance | V1–V6 | V1–V2 only |
| Septal Q in I/V6 | Absent | Present |
Management Considerations
- New LBBB + chest pain → STEMI workup immediately (PCI/thrombolysis)
- New LBBB + CHF or cardiomegaly → Echocardiogram
- Asymptomatic LBBB → Standard resting/exercise ECG unreliable; use stress echocardiogram or nuclear perfusion imaging
- LBBB + HF with reduced EF (EF ≤35%) → Consider cardiac resynchronization therapy (CRT)
This is a shared conversation. Sign in to Orris to start your own chat.