Management of hyperkalemia
Reading File
Finding Sources
Searching PubMed
"hyperkalemia" AND "management"
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from Harrison's 22E (2025) covering all three stages of hyperkalemia treatment. I have everything needed to write a thorough, well-organized answer.
Management of Hyperkalemia
Definition: Serum K+ ≥5.5 mEq/L (mmol/L). Levels ≥6.0 mEq/L or any level with ECG changes constitute a medical emergency.
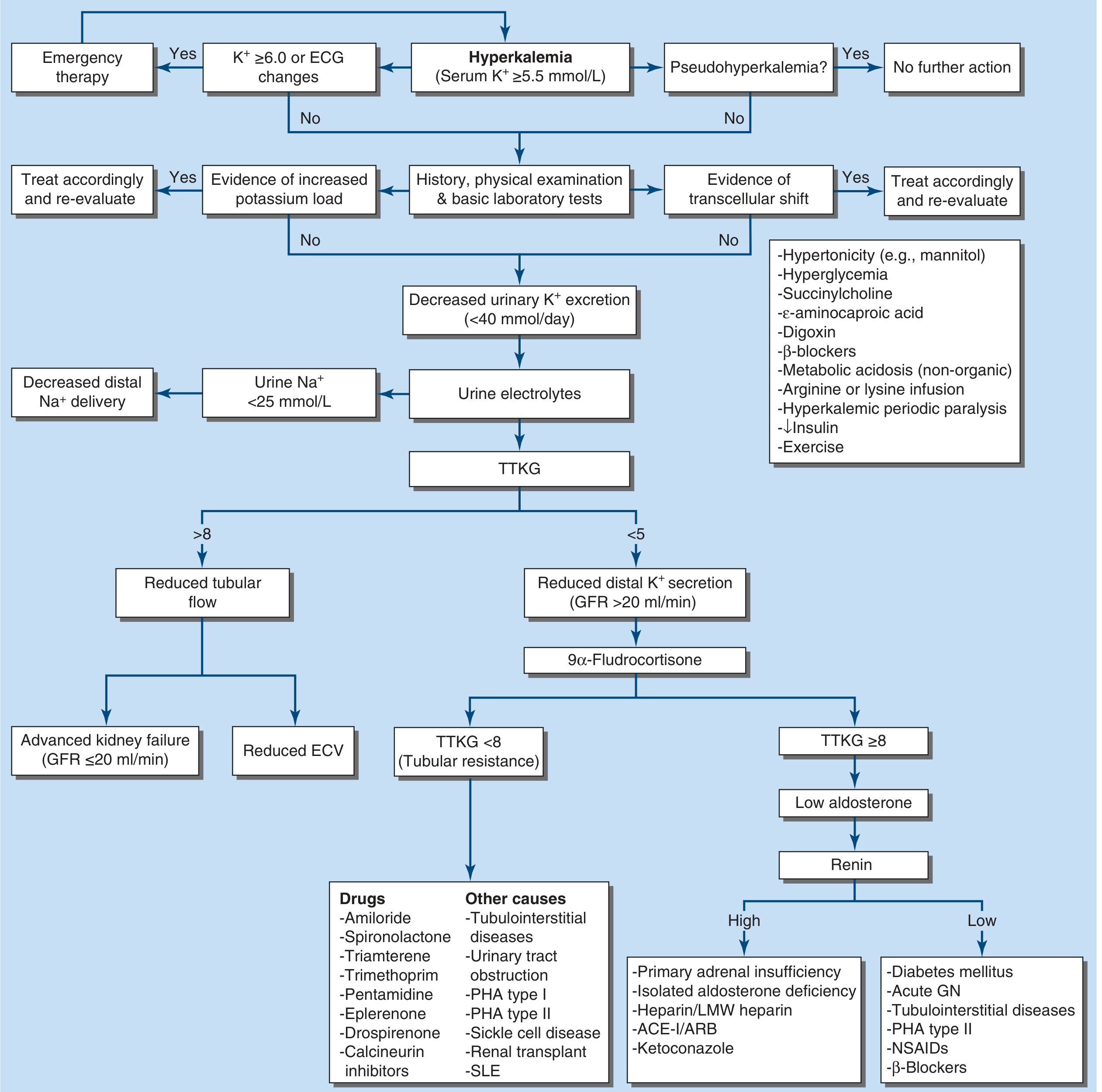
Step 0 - First Rule Out Pseudohyperkalemia
Before treating, confirm the result is real. Pseudohyperkalemia occurs with hemolysis, extreme leukocytosis, thrombocytosis, or prolonged tourniquet time. Repeat with a fresh, atraumatic sample if suspected.
Step 1 - Assess Severity and Obtain an ECG Immediately
ECG changes follow a characteristic progression as K+ rises:
| K+ Level | ECG Changes |
|---|---|
| 5.5-6.0 mEq/L | Tall, peaked (tented) T waves, shortened QT |
| 6.0-6.5 mEq/L | Prolonged PR, widened QRS |
| 6.5-7.0 mEq/L | Loss of P waves, further QRS widening |
| >7.0 mEq/L | Sine wave pattern → ventricular fibrillation/asystole |
An ECG should be obtained whenever hyperkalemia is suspected. A normal ECG does not rule out dangerous hyperkalemia - ECG changes can be absent even at severely elevated levels. K+ ≥6.0 mEq/L with OR without ECG changes warrants urgent treatment.
- Harrison's Principles of Internal Medicine 22E (2025), p. 404
- Rosen's Emergency Medicine, p. 1367
Treatment: Three Stages
Treatment is organized into three sequential but often simultaneous stages:
Stage 1 - Cardiac Membrane Stabilization (Immediate)
Goal: Protect the heart while other measures take effect. Does NOT lower serum K+.
IV Calcium
-
Calcium raises the action potential threshold, restoring the difference between resting and threshold potentials - it reverses depolarization blockade without changing the resting membrane potential.
-
Dose: 10 mL of 10% calcium gluconate IV over 2-3 minutes with continuous cardiac monitoring (alternatively: 3-4 mL of 10% calcium chloride - note CaCl has ~3x more elemental calcium but is more irritating to veins)
-
Onset: 1-3 minutes; Duration: 30-60 minutes
-
Repeat if no ECG improvement, or if ECG changes recur after initial improvement
-
Caution in digoxin toxicity: Hypercalcemia potentiates digoxin cardiac toxicity. If calcium is judged necessary, dilute 10 mL of 10% calcium gluconate in 100 mL D5W and infuse over 20-30 min. The best treatment of hyperkalemia in acute digoxin toxicity is digoxin-specific Fab fragments.
-
Harrison's, p. 404; Morgan & Mikhail's Clinical Anesthesiology 7e, p. 2179
Stage 2 - Redistribution of K+ into Cells (Rapid, Temporary)
Goal: Buy time. These measures temporarily drive K+ intracellularly. They do NOT remove K+ from the body.
A. Insulin + Glucose (First-line)
- Mechanism: Insulin activates the Na+/K+-ATPase pump, shifting K+ into cells
- Dose: 10 units regular insulin IV + 50 mL of 50% dextrose (D50W = 25 g glucose) immediately after
- Onset: 10-20 min; Peak: 30-60 min; Duration: 4-6 hours
- Important: Do NOT give bolus D50W without insulin - hypertonic glucose alone acutely worsens hyperkalemia via osmotic effects
- If glucose ≥200-250 mg/dL, give insulin without glucose, with close monitoring
- Follow with 10% dextrose infusion at 50-75 mL/h to prevent hypoglycemia
B. Beta-2 Agonists (Additive to insulin)
- Nebulized albuterol: 10-20 mg in 4 mL normal saline inhaled over 10 minutes
- Onset: ~30 min; Peak: ~90 min; Duration: 2-6 hours
- Effect is additive with insulin + glucose
- Caveat: ~20% of ESRD patients are resistant to beta-2 agonists - never rely on albuterol alone without insulin
- Side effects: tachycardia, hyperglycemia
- Use with caution in patients with known cardiac disease
C. Sodium Bicarbonate
-
Older teaching: IV sodium bicarbonate drives K+ into cells via exchange for H+
-
Current evidence: IV bicarbonate has no role in acute treatment of hyperkalemia as a rapid agent
-
A delayed drop in plasma K+ (4-6 h) can be seen after sustained isotonic bicarbonate infusion in patients with metabolic acidosis
-
Correct method if used: Infuse 150 mEq NaHCO3 in 1 L D5W (isotonic preparation) - do NOT give repeated hypertonic bolus ampules due to risk of hypernatremia and hypertonicity
-
Harrison's 22E, p. 404
Stage 3 - Removal of Potassium from the Body (Definitive)
Goal: Reduce total body K+. Essential to prevent recurrence.
A. Loop Diuretics (if renal function adequate)
- Furosemide promotes renal K+ excretion
- Useful in volume-replete or hypervolemic patients with sufficient renal function
- May combine with IV saline (for hypovolemic patients with oliguria and decreased distal Na+ delivery) or isotonic bicarbonate
B. Potassium Binders (for subacute/chronic management)
| Agent | Mechanism | Notes |
|---|---|---|
| Sodium zirconium cyclosilicate (SZC, Lokelma) | Inorganic crystalline compound; exchanges Na+ and H+ for K+ and NH4+ in intestine | Preferred newer agent; faster onset than patiromer |
| Patiromer (Veltassa) | Non-absorbed polymer; binds K+ in exchange for Ca2+ | Watch for hypomagnesemia; approved for chronic hyperkalemia |
| Sodium polystyrene sulfonate (SPS, Kayexalate) | Exchanges Na+ for K+ in GI tract | Full effect takes up to 24 h; FDA black box warning for intestinal necrosis (risk increased in reduced gut motility, post-op, opioid use, with sorbitol); use only when alternatives unavailable |
- SPS and patiromer are not for urgent/acute hyperkalemia management due to delayed onset
- SZC has a faster onset and is preferred in many settings
- The newer binders (SZC, patiromer) allow patients on RAAS inhibitors (ACE-I, ARBs, MRAs) to continue therapy despite CKD or heart failure - a major clinical advance
C. Hemodialysis (Definitive)
-
The most effective and reliable method to reduce plasma K+
-
Peritoneal dialysis is considerably less effective
-
Indicated for: severe or refractory hyperkalemia, AKI with impaired K+ excretion, patients unable to tolerate other therapies
-
Amount of K+ removed depends on dialyzer type, blood and dialysate flow rates, duration, and the plasma-to-dialysate K+ gradient
-
Harrison's 22E, p. 404; Morgan & Mikhail's, p. 2180
ECG Monitoring Summary
Continuous cardiac monitoring is mandatory during acute management. The ECG changes in hyperkalemia progress as shown in Morgan & Mikhail's:
Peaked T waves → widened QRS + prolonged PR → loss of P waves → sine wave pattern → ventricular fibrillation / asystole
- Morgan & Mikhail's Clinical Anesthesiology 7e, p. 2179
Special Situations
| Situation | Key Modification |
|---|---|
| Digoxin toxicity | Fab fragments are the treatment of choice; use calcium cautiously (dilute, slow infusion) |
| Metabolic acidosis | Bicarbonate infusion may help over hours; correct underlying cause |
| Hypoaldosteronism | Mineralocorticoid replacement (fludrocortisone 0.1 mg/day) if GFR >20 mL/min and TTKG <5 |
| ESRD / CKD | Hemodialysis is often the only reliable option; ~20% are albuterol-resistant; succinylcholine contraindicated |
| Surgical patient | Elective surgery contraindicated; avoid succinylcholine, potassium-containing IV fluids; prevent acidosis; control ventilation under GA |
| CKD on ACE-I/ARB/MRA | Novel binders (SZC, patiromer) allow continuation of RAAS inhibition |
Quick Reference Summary Table
| Intervention | Onset | Duration | Effect | Stage |
|---|---|---|---|---|
| IV Calcium gluconate | 1-3 min | 30-60 min | Membrane stabilization only | 1 |
| Insulin + D50W | 10-20 min | 4-6 h | Shift K+ into cells | 2 |
| Nebulized albuterol (10-20 mg) | 30 min | 2-6 h | Shift K+ into cells | 2 |
| Isotonic NaHCO3 infusion | 4-6 h | Variable | Shift K+ into cells (acidosis) | 2 |
| Loop diuretic | Variable | - | Remove K+ via urine | 3 |
| SZC (Lokelma) | Hours | - | Remove K+ via GI tract | 3 |
| Patiromer | Hours-days | - | Remove K+ via GI tract | 3 |
| SPS (Kayexalate) | Up to 24 h | - | Remove K+ via GI tract | 3 |
| Hemodialysis | Minutes | Duration of session | Most effective removal | 3 |
Recent Evidence Note
A 2025 network meta-analysis (PMID 40542996) confirmed that novel potassium binders (SZC and patiromer) are effective in reducing hyperkalemia AND enable optimization of RAAS inhibitor therapy in patients with CKD or heart failure - supporting their use over SPS in chronic management settings.
Primary sources: Harrison's Principles of Internal Medicine 22E (2025) - the most up-to-date reference used; Morgan & Mikhail's Clinical Anesthesiology 7e; Rosen's Emergency Medicine 10e
Peadiatric dose of levipil
Reading File
Finding Sources
Searching the Web
levetiracetam Levipil pediatric dose mg/kg children epilepsy
Excellent - I have comprehensive, age-stratified dosing from multiple authoritative sources. Here is the full answer:
Levipil (Levetiracetam) - Pediatric Dosing
Levipil is the Indian brand name for levetiracetam, an antiepileptic used as adjunctive therapy for partial-onset, myoclonic, and generalized tonic-clonic seizures.
Key pharmacokinetic point in children: Clearance is 30-40% higher and half-life shorter (~5-6 h vs. 7.2 h in adults), so children require higher doses on a mg/kg basis than adults.
Age-Stratified Dosing (Oral)
| Age Group | Starting Dose | Titration | Maximum Dose | Formulation |
|---|---|---|---|---|
| 1 month to <6 months | 7 mg/kg twice daily (14 mg/kg/day) | Increase by 7 mg/kg BD every 2 weeks | 21 mg/kg twice daily (42 mg/kg/day) | 100 mg/mL oral solution |
| 6 months to <4 years | 10 mg/kg twice daily (20 mg/kg/day) | Increase by 10 mg/kg BD every 2 weeks | 25 mg/kg twice daily (50 mg/kg/day) | 100 mg/mL oral solution |
| 4 years to <12 years (and adolescents <50 kg) | 10 mg/kg twice daily (20 mg/kg/day) | Increase by 10 mg/kg BD every 2 weeks | 30 mg/kg twice daily (60 mg/kg/day) | Oral solution or tablet |
| Adolescents ≥12 years, weight <50 kg | 10 mg/kg twice daily | Increase by 10 mg/kg BD every 2 weeks | 30 mg/kg twice daily (60 mg/kg/day) | Tablet or solution |
| Adolescents ≥12 years, weight ≥50 kg (adult dosing) | 500 mg twice daily | Increase by 500 mg BD every 2-4 weeks | 1500 mg twice daily (3000 mg/day) | Tablet (250/500/750 mg) |
The lowest effective dose should always be used. Dose changes should not exceed the stated increments.
IV / Infusion Dose (Levetiracetam Injection)
Used when oral route is not available (same total daily dose as oral):
- Children 4 years and older: Same mg/kg dose as oral, given as a 15-minute IV infusion, divided into 2 doses/day
- Acute seizures / status epilepticus (off-label loading): 20-60 mg/kg IV over 15 minutes (used in practice; max commonly 3000 mg)
- For head trauma prophylaxis (Tintinalli's): 20 mg/kg IV (max 500 mg/dose) for the first week
Levipil Formulations Available in India
| Formulation | Strength |
|---|---|
| Levipil 250 mg tablet | 250 mg |
| Levipil 500 mg tablet | 500 mg |
| Levipil 750 mg tablet | 750 mg |
| Levipil 1000 mg tablet | 1000 mg |
| Levipil oral solution | 100 mg/mL (bottle) |
| Levipil injection | 500 mg/5 mL |
Practical Titration Example (Child, 20 kg, age 6 years)
| Week | Dose |
|---|---|
| Week 1-2 | 200 mg (10 mg/kg) BD |
| Week 3-4 | 300 mg (15 mg/kg) BD |
| Week 5-6 | 400 mg (20 mg/kg) BD |
| Maintenance (target) | Up to 600 mg (30 mg/kg) BD |
Important Clinical Notes
- Twice-daily dosing is standard for all age groups
- Renal dose adjustment is required: levetiracetam is ~66% renally cleared. Reduce dose if eGFR <80 mL/min/1.73m²
- No hepatic adjustment needed (minimal hepatic metabolism)
- Enzyme-inducing AEDs (e.g., carbamazepine) increase levetiracetam clearance by ~22% - may need higher doses
- Behavioral side effects (irritability, aggression) are more common in children than adults; inform parents
- No significant drug-drug interactions with common AEDs (valproate, lamotrigine, topiramate, carbamazepine)
- Neonates (<1 month): not formally approved; used cautiously at 10-20 mg/kg/day in some NICUs
Sources: UCB Pharma/Keppra prescribing information (Mar 2024); Tintinalli's Emergency Medicine; FDA pediatric review; PMC levetiracetam in childhood epilepsy review
This is a shared conversation. Sign in to Orris to start your own chat.