Hashimoto thyroiditis
Reading File
Finding Sources
Searching PubMed
"Hashimoto thyroiditis"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Loading Image
Finding Sources
Reading File
Finding Sources
I have all the necessary information. Here is the comprehensive answer:
Hashimoto Thyroiditis
Hashimoto thyroiditis (chronic autoimmune thyroiditis / chronic lymphocytic thyroiditis) is the most common cause of hypothyroidism in iodine-sufficient regions, and the most prevalent autoimmune disease in the United States.
Epidemiology
- Most common cause of diffuse goiter and hypothyroidism in iodine-replete countries (responsible for ~85% of hypothyroid cases in those areas)
- Prevalence of hypothyroidism in iodine-replete populations: 1-2%
- Peak age: 45-65 years (also reported in 3rd-5th decades)
- Female predominance: female-to-male ratio of 10:1 to 20:1
- Clusters in families; co-occurs with Graves disease and other autoimmune diseases
Pathogenesis
The disease results from a breakdown of immune self-tolerance to thyroid antigens, with progressive autoimmune destruction of thyrocytes. Key mechanisms:
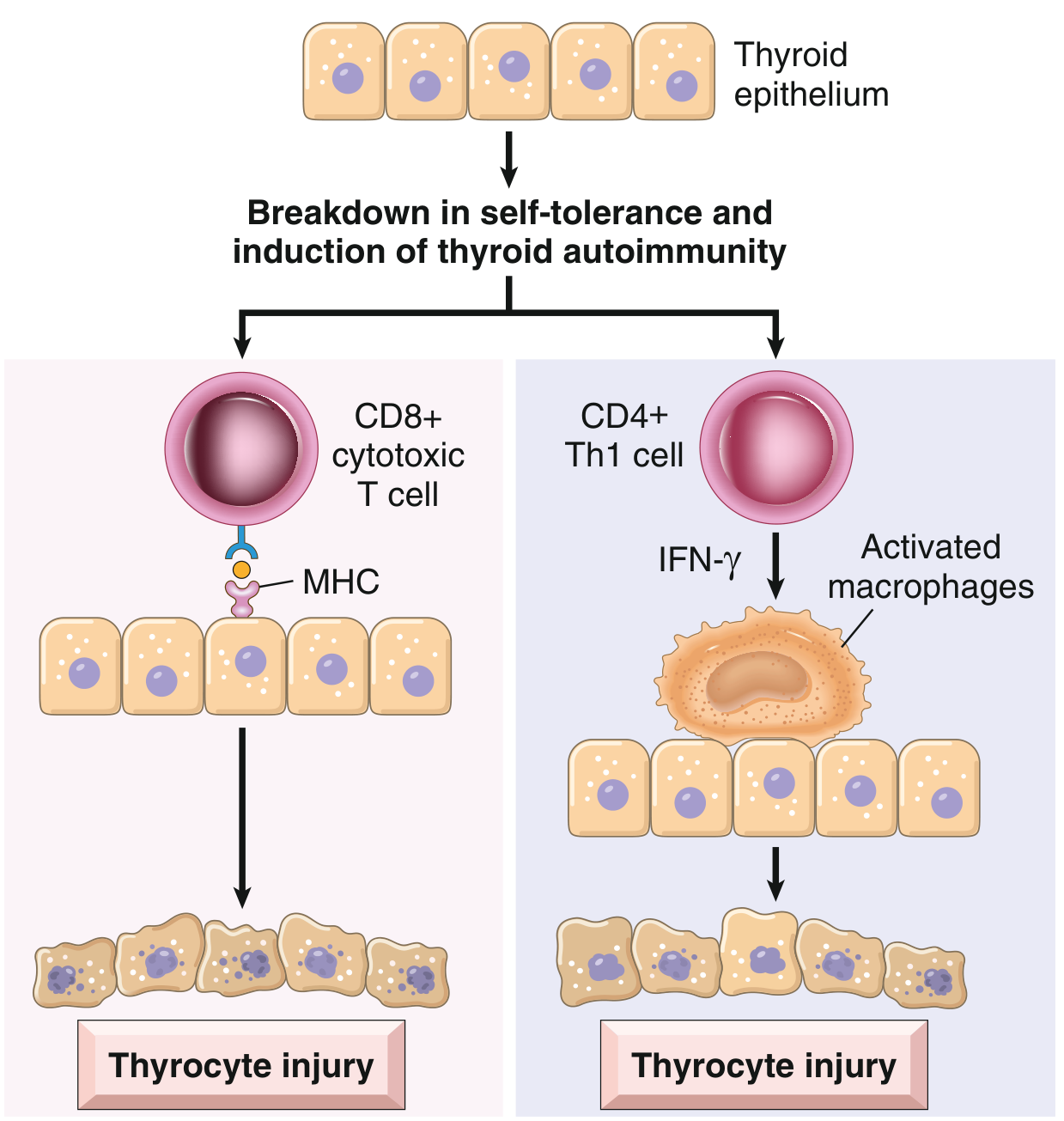
Fig. 18.4 - Pathogenesis of Hashimoto thyroiditis (Robbins & Kumar Basic Pathology)
- CD8+ cytotoxic T cells - kill thyroid epithelial cells directly via MHC-restricted mechanisms
- CD4+ Th1 cytokine-mediated damage - IFN-γ production recruits and activates macrophages, which destroy follicles
- Antithyroid antibodies - anti-thyroid peroxidase (anti-TPO, also called antimicrosomal antibody) and anti-thyroglobulin antibodies are present in nearly all patients. These may contribute via antibody-dependent cell-mediated cytotoxicity (ADCC) or complement-dependent mechanisms, though it remains unclear if they are the cause or consequence of injury.
Genetic factors:
- ~40% concordance in monozygotic twins
- ~50% of asymptomatic siblings carry antithyroid antibodies
- Associated with polymorphisms in CTLA4 (an inhibitor of T-cell responses) and other immune-regulatory genes
Morphology / Histology
- Thyroid is usually diffusely and symmetrically enlarged
- Microscopy (classic features):
- Widespread mononuclear inflammatory infiltrate: lymphocytes, plasma cells, macrophages
- Well-developed germinal centers (lymphoid follicle formation)
- Thyroid follicles are atrophic
- Hürthle (oxyphil) cell metaplasia - follicular epithelial cells with abundant eosinophilic, granular cytoplasm due to numerous mitochondria (metaplastic response to injury)
- Interstitial fibrosis (variable, may be abundant)
- Fibrosing variant - forms a massive, firm goiter; can be difficult to distinguish from Riedel thyroiditis
Clinical Features
| Feature | Detail |
|---|---|
| Presentation | Painless, firm, symmetric goiter in a middle-aged woman |
| Thyroid function | Usually euthyroid at presentation; hypothyroidism develops in ~20% and progresses over time |
| Hashitoxicosis | Transient thyrotoxicosis early in disease from follicular destruction releasing stored hormone; elevated free T4/T3, suppressed TSH, low radioiodine uptake |
| Compressive symptoms | Dyspnea, dysphagia, cough, hoarseness, choking (if goiter is large) |
| Persistent symptoms | Fatigue, muscle/joint pain, poor sleep, dry mouth/eyes - may not resolve with hormone replacement (thought to be autoimmune-mediated) |
On ultrasound: Diffuse heterogeneity of the gland is the hallmark finding.
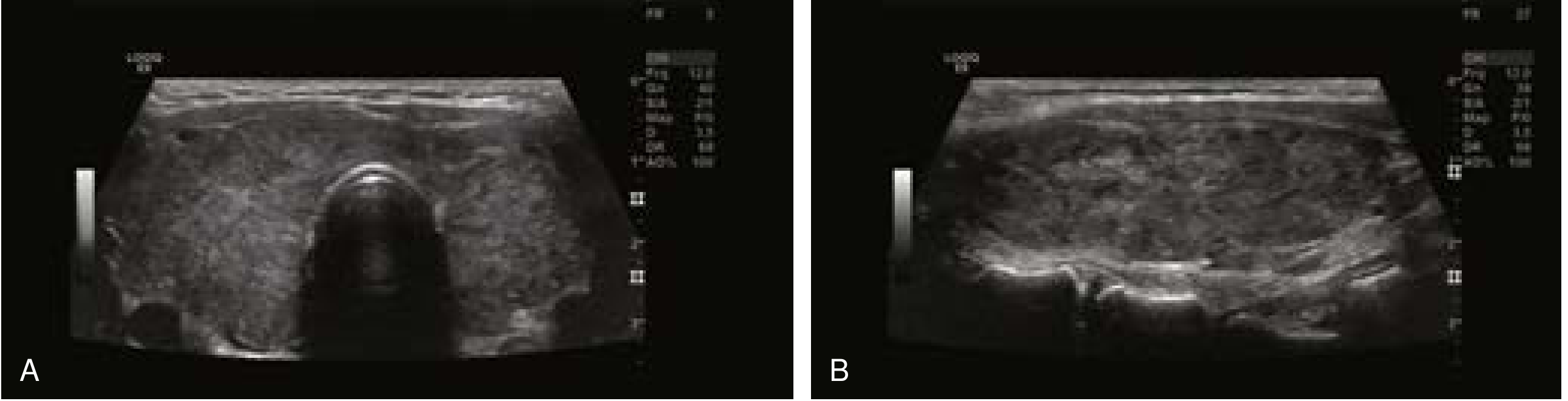
Fig. 3 - Diffuse heterogeneity characteristic of Hashimoto thyroiditis (Current Surgical Therapy, 14e)
Laboratory Findings
- Anti-TPO antibodies (antimicrosomal): elevated in 70-90% of patients - most sensitive marker
- Anti-thyroglobulin antibodies: also commonly elevated
- TSH: elevated in hypothyroid phase; suppressed in hashitoxicosis phase
- Free T4/T3: low in hypothyroid phase; elevated transiently in hashitoxicosis
- Inflammatory cytokines elevated
Thyroid Nodules and Cancer Risk
- Hürthle cell metaplasia leads to associated thyroid nodules (most are benign Hürthle cell nodules)
- FNAB findings: follicular epithelial cells, colloid, lymphocytes, Hürthle cells - classified as Bethesda II (benign)
- Predominance of Hürthle cells may be Bethesda III (AUS) or IV (Hürthle cell neoplasm)
- Can cause false-positive FNAB suspicious for papillary thyroid cancer (Bethesda V)
- Any discrete palpable nodule not part of diffuse goiter should be evaluated with FNA regardless of the Hashimoto diagnosis
- Increased risk of B-cell non-Hodgkin lymphoma (primary thyroid lymphoma) - a rapidly enlarging mass within a Hashimoto gland warrants urgent biopsy
- Possible increased predisposition to papillary thyroid carcinoma (controversial)
Treatment
1. Asymptomatic / Euthyroid
- Observation; no treatment required
2. Hypothyroidism
- Levothyroxine (T4) replacement - resolves hypothyroid symptoms and typically reduces goiter size
- Dose titrated to normalize TSH
3. Persistent Symptoms Despite Adequate Hormone Replacement
- Many symptoms (fatigue, myalgia, dry eyes) may be autoimmune-mediated and do not resolve with T4 alone
- Total thyroidectomy is an option in this setting: removes the antigenic target, reduces the systemic inflammatory response, and lowers anti-TPO titers and pro-inflammatory cytokines
- The Norwegian Trial on Surgery for Hashimoto Disease (prospective RCT) demonstrated improved health-related quality of life, reduced fatigue, and normalization of anti-TPO titers in surgically treated patients vs. controls
4. Compressive Goiter / Surgical Indications
- Surgery for large, symptomatic, or refractory goiter
- Thyroid lobectomy + isthmusectomy for unilateral disease; total thyroidectomy for bilateral or extensive disease
- Intraoperative nerve monitoring recommended (inflamed, firm gland increases risk of recurrent laryngeal nerve traction injury)
- Enlarged reactive central compartment lymph nodes are common; frozen section can exclude metastatic thyroid cancer
5. Radioiodine (I-131)
- Typically contributes little useful information to the workup (I-123 scanning also not usually helpful)
Associated Conditions and Variants
| Condition | Notes |
|---|---|
| Painless (silent) thyroiditis | Variant of Hashimoto; autoimmune follicular destruction with spontaneously resolving hyperthyroidism |
| Postpartum thyroiditis | Specific type of painless thyroiditis; occurs within 1 year of delivery or abortion; up to 10% of pregnancies; may recur with subsequent pregnancies |
| Fibrosing variant | Massive firm goiter; mimics Riedel thyroiditis |
| Graves disease | Can coexist (both share autoimmune thyroid pathogenesis) |
| Other autoimmune diseases | Type 1 DM, Addison disease, pernicious anemia, vitiligo, etc. |
Sources: Robbins & Kumar Basic Pathology, p. 731 | Current Surgical Therapy, 14e, pp. 885-886 | K.J. Lee's Essential Otolaryngology, p. 727
This is a shared conversation. Sign in to Orris to start your own chat.