Here's everything about gait explained in simple, everyday language - like a teacher explaining it to you in class.
🚶 GAIT - Everything in Simple Language
PART 1: What IS Gait?
Gait simply means: the way you walk.
Every time you take a step, your body does a very complex, coordinated series of movements involving your brain, spine, muscles, bones, and joints - all working together automatically. Scientists have broken this down into phases, measurements, and patterns to understand what's "normal" and what's "abnormal."
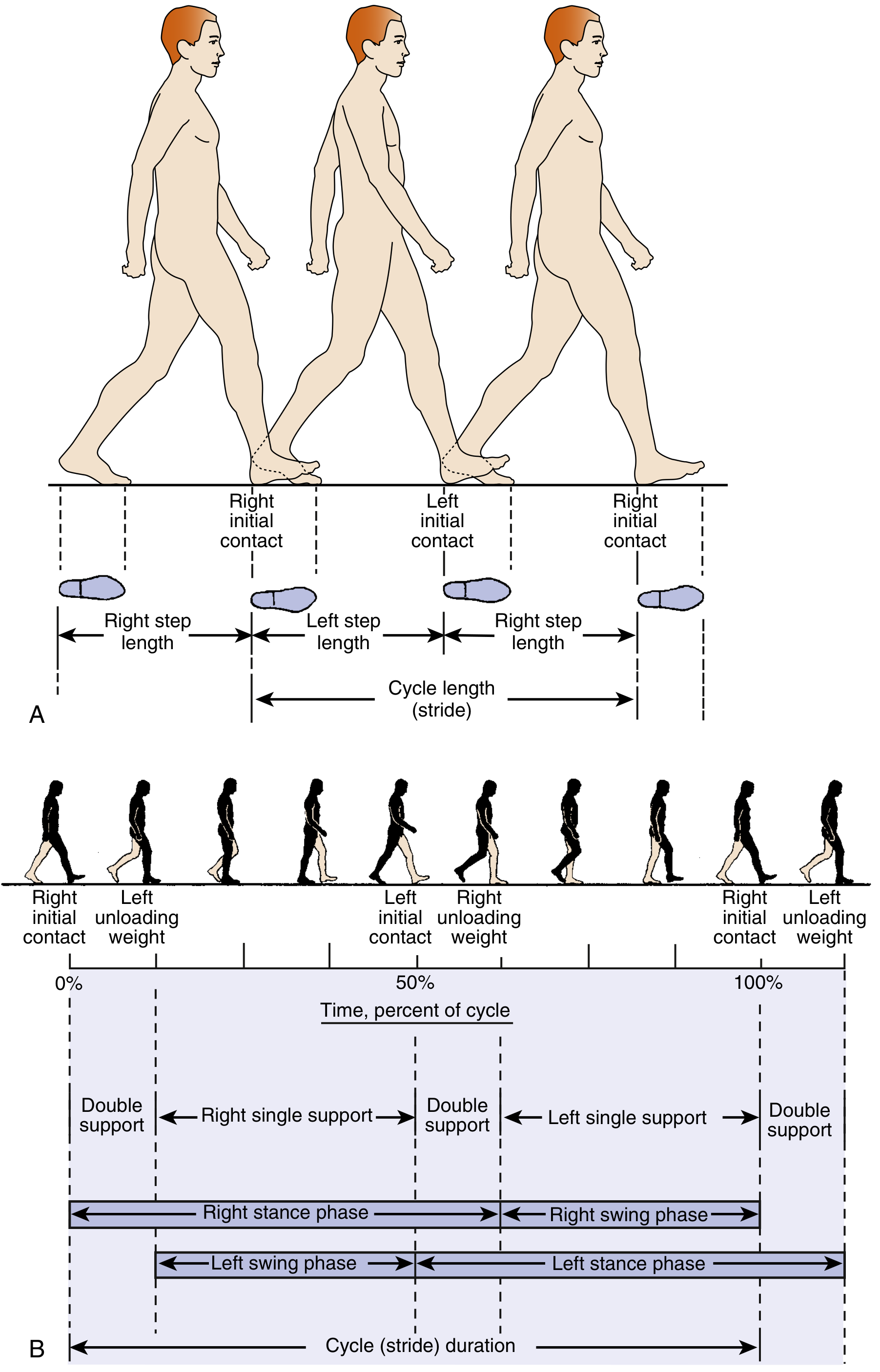
PART 2: The Gait Cycle - "One Full Walk Step"
Think of it like this:
One gait cycle = from the moment your RIGHT heel hits the ground → to the next time your RIGHT heel hits the ground again.
This is called one stride.
That stride is split into two big parts:
🦶 Stance Phase (60% of the cycle)
"When your foot is ON the ground"
Your foot is touching the ground for 60% of the time. This is when you're bearing your weight.
It has 5 sub-phases (think of them like events in a race):
| Sub-phase | What's Happening | Simple Analogy |
|---|
| Initial Contact (IC) | Your heel first touches the ground | "Heel hits the floor" |
| Loading Response (LR) | Weight shifts onto that foot | "You're landing" |
| Midstance | Your body passes over the foot | "Balancing on one leg" |
| Terminal Stance | Your heel starts rising, body moves forward | "Pushing forward, heel coming up" |
| Preswing | Your toes push off, getting ready to swing | "The push-off moment" |
🦵 Swing Phase (40% of the cycle)
"When your foot is IN THE AIR"
Your foot is off the ground for 40% of the time. Your leg swings forward to take the next step.
| Sub-phase | What's Happening |
|---|
| Initial Swing | Foot just left the ground, starts moving forward |
| Midswing | Foot is directly under the body, clearing the floor |
| Terminal Swing | Leg is fully forward, about to make contact again |
⚡ Double Support
During normal walking, there are two brief moments when BOTH feet are on the ground at the same time. This is called double limb support.
Key rule: The faster you walk → the shorter the double support time. When you RUN, double support disappears entirely and becomes a "float phase" where NEITHER foot touches the ground!
PART 3: Gait Parameters - The Measurements
Think of these like measuring how you walk with a ruler and a stopwatch.
Spatial Parameters (Distance measurements)
These are about how far:
| Term | What it means | Simple way to remember |
|---|
| Step length | Distance from where your RIGHT heel lands to where your LEFT heel lands | One step forward |
| Stride length | Distance from RIGHT heel strike to the NEXT RIGHT heel strike | = 2 steps combined (~1.5 m normally) |
| Step width | How far apart your feet are side-to-side | Width of your footprints |
| Foot angle | How much your foot points outward | ~7° outward is normal |
Temporal Parameters (Time measurements)
These are about how long:
| Term | What it means |
|---|
| Cadence | Number of steps per minute (~100-120 steps/min normally) |
| Gait velocity | Your walking speed (step length × cadence) |
| Stance time | How long each foot is on the ground |
| Swing time | How long each foot is in the air |
| Double support time | How long both feet are on the ground together |
PART 4: The 6 Determinants of Gait - "How Your Body Saves Energy"
Here's a great way to think about this:
Walking is your body's way of moving forward as efficiently as possible - using the least energy.
If you walked like a robot (completely stiff), your head would bob up and down massively and you'd waste enormous energy. Your body uses 6 clever tricks to keep your center of gravity (your body's "balance point") as smooth and level as possible.
Your center of gravity sits just in front of your spine (S2 level) - roughly below your belly button. During walking it moves:
- Up and down: 5 cm (like a gentle wave)
- Side to side: 6 cm
The 6 tricks that keep this motion smooth:
Trick 1: Pelvic Rotation
🔄 Your pelvis rotates forward with each step
Imagine your pelvis like a propeller - it slightly rotates left and right as you walk. This rotation extends the effective leg length and allows you to take longer steps without raising your body higher. Without it, your head would bounce up and down more.
Trick 2: Pelvic Tilt (List)
↘️ The pelvis dips on the non-weight-bearing side by about 5 degrees
When your left leg is in the air (swing), your left hip drops slightly. This smooths out the "height" of your body's path - instead of rising too high over the stance leg, it's dampened.
Trick 3: Knee Flexion at Loading
🦵 Your knee bends about 15° when your heel hits the ground
Think of it like the suspension of a car. When the heel hits the ground, the knee bends slightly to absorb the shock. Without this, every heel strike would send a jarring impact up your leg.
Trick 4: Foot & Ankle Motion
👣 The foot and ankle act as a series of "rockers"
Your foot rolls over the ground smoothly:
- Heel rocker (heel strike to foot flat)
- Ankle rocker (foot flat through midstance)
- Forefoot rocker (heel rise to toe-off)
This rolling motion keeps forward progression smooth and efficient. The subtalar joint also absorbs shock by allowing the heel to evert (roll inward) at landing.
Trick 5: Knee Motion (working with ankle)
The knee flexes during loading and extends at midstance - working together with the ankle to further smooth out the path of the body's center of gravity.
Trick 6: Lateral Pelvic Shift
↔️ Your body shifts 5 cm over the stance limb
As weight moves onto one leg, your pelvis shifts slightly toward that leg. This narrows your base of support and keeps you balanced without having to swing wildly side to side.
Bottom line: All 6 determinants work together like a well-tuned machine to keep your head traveling in a smooth, nearly straight line - saving enormous energy over a day of walking.
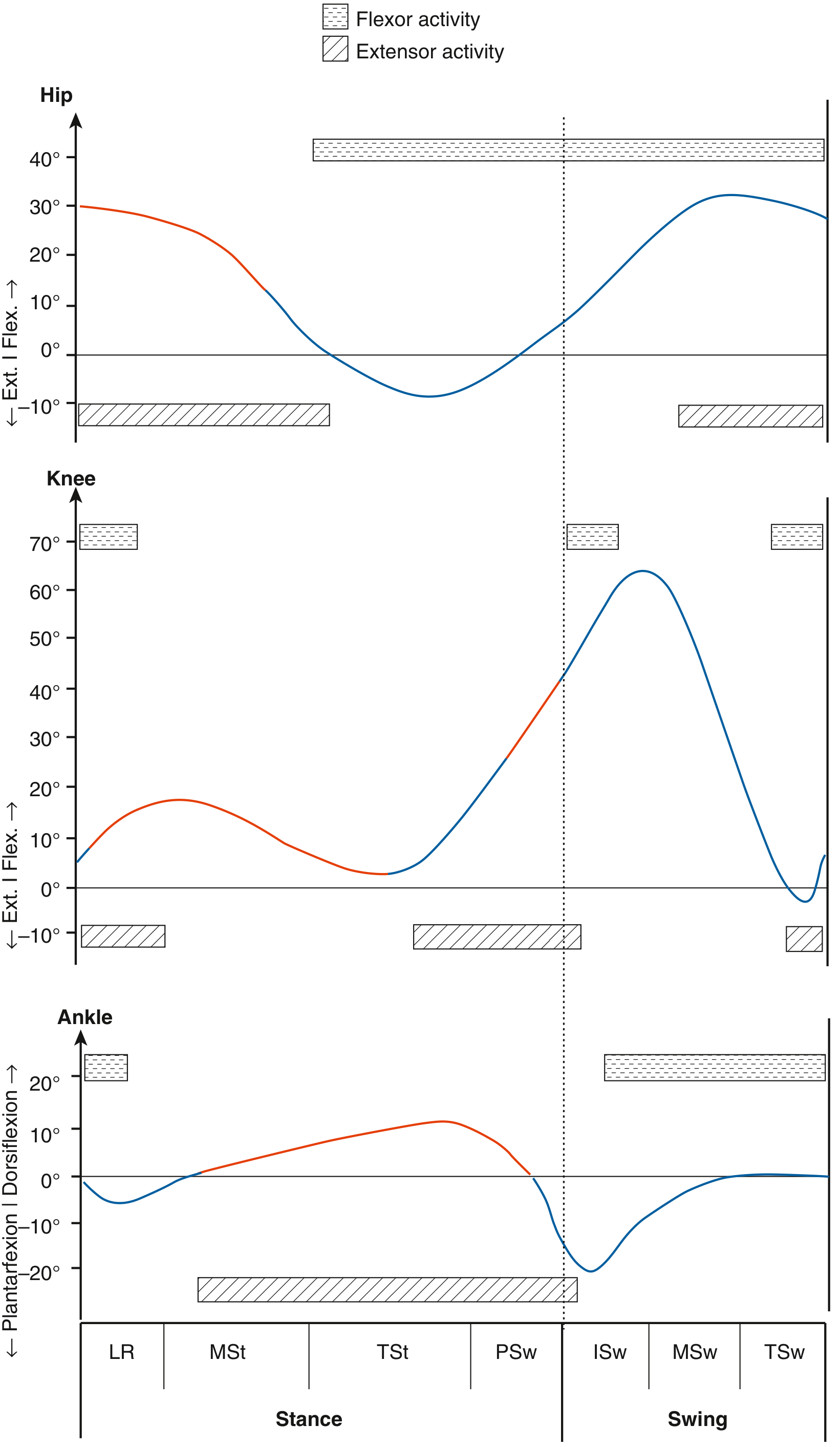
PART 5: Kinematics - "What Joints Are Doing"
Kinematics = just the motion. No forces, just angles.
Think of it as watching someone walk and measuring "how much did the hip/knee/ankle bend at each moment?"
Hip Joint Journey Through One Gait Cycle
| Moment | What the hip does | Why |
|---|
| Heel strike | Bent (flexed) at ~30° | Reaching forward to land |
| Through stance | Gradually straightens, then goes to ~10° extension | Body moving forward over the leg |
| Push-off (preswing) | Starts bending again | Preparing to swing |
| Through swing | Bends back up to 30° | Bringing the leg forward |
Muscles doing the work:
- Gluteus maximus powers the hip from bent → straight (stance)
- Iliopsoas pulls the leg forward during swing
Knee Joint Journey
| Moment | What the knee does | Why |
|---|
| Heel strike | Slightly bent ~5-8° | Shock absorption ready |
| Loading response | Bends to ~15-18° | Absorbs impact (like suspension) |
| Midstance | Straightens to 0° | Supporting body weight efficiently |
| Preswing | Bends again | Preparing to swing |
| During swing | Bends up to 65° | Clearing the foot off the floor |
| End of swing | Straightens back to 0° | Ready to land again |
Ankle Joint Journey
| Moment | What the ankle does | Why |
|---|
| Heel strike | Slight plantarflexion (pointing down, ~5°) | Heel touches first |
| Foot flat | Moves to neutral | Controlled by tibialis anterior |
| Midstance | Bends backward (dorsiflexion) to ~10° | Body moving forward over the foot |
| Terminal stance | Maximum dorsiflexion then heel rises | Body propulsion begins |
| Push-off | Rapid plantarflexion ~20° (pointing down) | PROPULSION - the push that moves you forward |
| During swing | Returns to neutral | Tibialis anterior lifts foot to clear the ground |
PART 6: Kinetics - "The Forces Behind the Motion"
Kinetics = the forces, pushes, and pulls that cause all that motion.
Ground Reaction Force (GRF) - The Most Important Force
When you walk, the ground pushes back up on your foot. This upward push from the ground is called the Ground Reaction Force (GRF).
Think of it like this: When you push down on a trampoline, the trampoline pushes back up. That "push back" on your feet during walking is the GRF.
How big is it?
- Walking: GRF = 1.5× your body weight on each heel strike
- Running: GRF = 3-4× your body weight (much bigger because of the impact after the float phase)
- Stairs/Arthritis: Up to 4-7× body weight at the knee
Why does it matter so much?
The GRF's position relative to each joint determines whether that joint is being pushed to flex or extend - which tells us which muscles need to fire to keep you upright.
For example:
- GRF passes in front of the hip → it tries to fold your hip forward → your gluteus maximus fires to stop this
- GRF passes behind the knee → it tries to straighten the knee → minimal quadriceps work needed (the joint is passively stable)
- GRF passes in front of the ankle → it tries to bend the ankle up → gastrocnemius-soleus fires to resist this and store energy for push-off
Joint Moments (Torques)
A moment or torque is just a rotating force around a joint. The GRF creates moments at each joint, and muscles counteract those moments.
Example: When you stand on one leg, the GRF pulls your pelvis to drop on the opposite side. Your gluteus medius generates a moment to keep the pelvis level. If this muscle is weak → pelvis drops = Trendelenburg sign.
Types of Muscle Work in Gait
| Type | What it means | Simple analogy | Example in gait |
|---|
| Eccentric | Muscle works while being stretched | Like lowering a weight slowly | Quadriceps controlling knee bend at landing |
| Concentric | Muscle shortens to move a limb | Like lifting a weight | Iliopsoas pulling leg forward in swing |
| Isometric | Muscle holds without changing length | Like holding a plank | Gluteus medius holding the pelvis level |
The KEY insight: Most of gait is ECCENTRIC work - your muscles are mostly acting as brakes and shock absorbers, not as engines. Walking is controlled falling!
Energy Flow in Gait
Think of gait like a pendulum:
- In stance, your body vaults over your foot like an inverted pendulum - converting kinetic energy to potential energy and back.
- The muscles store and release energy efficiently (especially the Achilles tendon at push-off).
- The 6 determinants minimize the distance the CoM has to travel, so less energy is wasted.
PART 7: Pathological Gait - "When Walking Goes Wrong"
Pathological gait = any abnormal walking pattern caused by disease, injury, weakness, or pain.
Think of each abnormal gait as your body's "best attempt" to walk despite a problem. Usually, what you see is a compensation - the body adapting to make walking possible even when something isn't working right.
1. 😣 Antalgic Gait - "Pain Walk"
The simplest of all - the body avoids pain.
What it looks like: The person takes a very short step on the sore leg and quickly shifts weight off it. It's a limp where the painful side has a shorter stance phase.
Why: Standing on a painful limb hurts. So the brain says "get off it as quickly as possible" → shortened stance phase on the painful side.
Causes: Arthritis, fracture, infection, any painful hip/knee/ankle
Memory trick: "Antalgic" = anti-algos (against pain). The gait is anti-pain.
2. 🦁 Trendelenburg Gait - "Sailor's Walk" or "Waddling"
Gluteus medius muscle is weak → pelvis droops on the opposite side.
What it looks like: When you stand on the RIGHT leg, the LEFT side of your pelvis drops down (instead of staying level). To compensate, the person leans their WHOLE UPPER BODY over to the right side.
Why: The gluteus medius (on the stance side) normally acts like a rope holding the pelvis level. If it's too weak to hold it up, the far side falls.
The compensation: Leaning the trunk over the weak side reduces the moment arm (the leverage the body weight has to pull the pelvis down), so less muscle force is needed to keep balance.
Bilateral weakness → both sides flop → looks like a waddling duck (waddling gait).
Causes: OA hip, fractured neck of femur, DDH, polio, post-op THA
Memory trick: Picture a ship listing (leaning) to one side - "Trendelenburg = trunk leans to the weak/bad side"
3. 🦆 Steppage Gait (High-Stepping Gait) - "Footdrop Walk"
The foot can't lift up (no dorsiflexion) → foot drags.
What it looks like: The person lifts their knee and hip extra high during the swing phase (like marching) to stop their toes dragging on the floor. When the foot does land, it slaps down loudly (foot slap).
Why: Tibialis anterior (the muscle on the front of the shin that lifts the foot) is paralyzed or weak → the foot hangs down limply. Without compensation, the toes would catch on the floor and the person would trip.
At heel strike: Because the tibialis anterior can't eccentrically control the foot's descent, the whole foot slaps down loudly onto the ground.
Causes: Common peroneal nerve palsy (due to fibular head fracture, prolonged crossing of legs), L4/L5 disc prolapse, Charcot-Marie-Tooth, stroke
Memory trick: "Step-PAGE" = you have to lift the foot extra HIGH like turning a page upward.
4. ✂️ Scissor Gait - "Scissors Crossing"
Both legs cross each other like scissors - too much adductor pull.
What it looks like: Both thighs rub together or cross as the person walks. The legs swipe past each other in a scissoring motion.
Why: The hip adductor muscles (inner thigh) are in spasm/spasticity. They pull both legs toward the midline constantly. Both legs end up trying to occupy the same space.
Causes: Cerebral palsy (spastic diplegia), spinal cord injury, severe bilateral spasticity
5. 🩰 Equinus Gait - "Toe Walking"
The ankle is stuck pointing down → person walks on their toes.
What it looks like: Walking entirely on tiptoe. May look like ballet walking.
Why: The ankle is contractured in plantarflexion (pointing down) and can't come back to neutral. This creates two secondary problems:
- During swing → foot too low → steppage gait develops to compensate (high knee lift)
- During stance → GRF is pushed forward → the knee tends to hyperextend backward (genu recurvatum)
Causes: Cerebral palsy (gastrocnemius spasticity), prolonged immobilization, Achilles contracture, idiopathic toe walking in children
6. 🦶 Calcaneus Gait - "All Heel, No Push"
The calf muscles (gastrocnemius-soleus) are too weak → can't push off.
What it looks like: The person heavily stamps on their heel throughout stance; heel never rises; no push-off phase; short shuffling steps.
Why: Gastrocnemius-soleus provides the propulsive force (push-off) at terminal stance. Without it, forward propulsion is lost.
Causes: Gastrocnemius-soleus weakness (post-surgery, nerve injury, compartment syndrome), Achilles tendon rupture
7. 🙇 Crouch Gait - "Bent Knee Throughout"
Knees stay bent even during stance - the person walks in a constant squat.
What it looks like: Exaggerated bending of hips AND knees throughout the entire walking cycle. Very energy-inefficient.
Why: Hamstrings too tight (won't let knee straighten) OR the plantarflexors too weak (ankle collapses into dorsiflexion, which pulls the knee into flexion by the lever effect). Sometimes leg is too long.
Causes: Cerebral palsy, hamstring contracture, long limb
8. 🧠 Hemiplegic Gait - "Stroke Walk"
One side of the body is weak and spastic after a stroke.
What it looks like: Very distinctive. The affected arm is bent and held against the chest. The affected leg swings outward in a semicircle (circumduction) because the knee can't bend properly to clear the floor during swing. The person leans slightly to the unaffected side.
The key features are:
- Ankle equinus (foot pointing down)
- Knee doesn't bend in swing (knee stiffness/extension spasticity)
- Hip can't flex well in swing → circumduction to clear the floor
- Prolonged stance on the UNAFFECTED side (the good leg bears weight longer)
Causes: Stroke (CVA), TBI, brain tumor, any upper motor neuron lesion
9. 🦆 Waddling Gait
Both sides Trendelenburg together → exaggerated side-to-side rocking of the trunk.
Causes: Bilateral hip pathology, muscular dystrophy (Duchenne's), bilateral CDH
10. ACL-Deficient (Quadriceps-Avoidance) Gait
The knee avoids bending to prevent the tibia from sliding forward.
With an ACL tear, activating the quadriceps forcefully (especially in mid-range knee flexion) would pull the tibia forward (anterior tibial translation) → pain and instability. So the brain unconsciously reduces quadriceps activation during midstance.
Compensation: The person leans their trunk forward, plantarflexes the ankle, or presses their hand on the knee to passively extend it - all to avoid needing the quadriceps to stabilize the knee.
PART 8: Running Gait - "Walking's Faster Cousin"
| Feature | Walking | Running |
|---|
| Double support | ✅ Yes (~10-20%) | ❌ No |
| Float phase | ❌ No | ✅ Yes (BOTH feet off ground) |
| GRF | ~1.5× body weight | ~3-4× body weight |
| Stance % | 60% | Less than 40% |
| Speed | Slower | Faster |
The float phase is the key difference. In running, both feet are off the ground simultaneously - which is why landing is so much more impactful. Your muscles and tendons (especially the Achilles) must store and release more energy.
The higher the running speed → the longer the float phase → the shorter the stance phase → the bigger the landing impact.
PART 9: Stair Climbing - "Gait Gone Uphill"
Stairs are much harder on your joints than level walking because:
- Your knee must bend to 90-120° (much more than the 65° in normal swing)
- Your quadriceps must work very hard concentrically to lift your body weight against gravity
- Stair descent is even harder - quadriceps work eccentrically to control the lowering → very high patellofemoral joint forces
Joint forces during stair climbing: 4-7× body weight at the knee (vs 1.5× during level walking).
Going up stairs (ascent):
- Leading leg: controls eccentric loading → pulls body upward
- Trailing leg: pushes off concentrically (quads + calf)
Going down stairs (descent):
- The leading leg must eccentrically control the knee bending against gravity - this requires MORE quadriceps force, not less
- Explains why people with knee OA struggle MORE with stairs down than stairs up
Quick Memory Cheat Sheet
| Gait | Muscle Problem | Simple clue |
|---|
| Antalgic | Pain | Limp, short stance on bad side |
| Trendelenburg | Gluteus medius weak | Pelvis drops away, trunk leans to bad side |
| Steppage | Tibialis anterior weak (footdrop) | High stepping, foot slap |
| Scissor | Adductors spastic | Legs crossing |
| Equinus | Ankle plantarflexion contracture | Toe walking |
| Calcaneus | Gastrocnemius-soleus weak | No push-off, heel walk |
| Crouch | Hamstrings tight/plantar flexors weak | Bent-knee squat walking |
| Hemiplegic | UMN lesion (stroke) | Circumduction, bent arm |
| Waddling | Bilateral abductor weakness | Side-to-side trunk sway |
That's the entire topic of Gait - broken down from first principles to clinical patterns. Ask me about any specific part you want to go deeper on!