Show me branches and blood supply of brachial artery around the elbow.
Brachial Artery: Branches and Blood Supply Around the Elbow
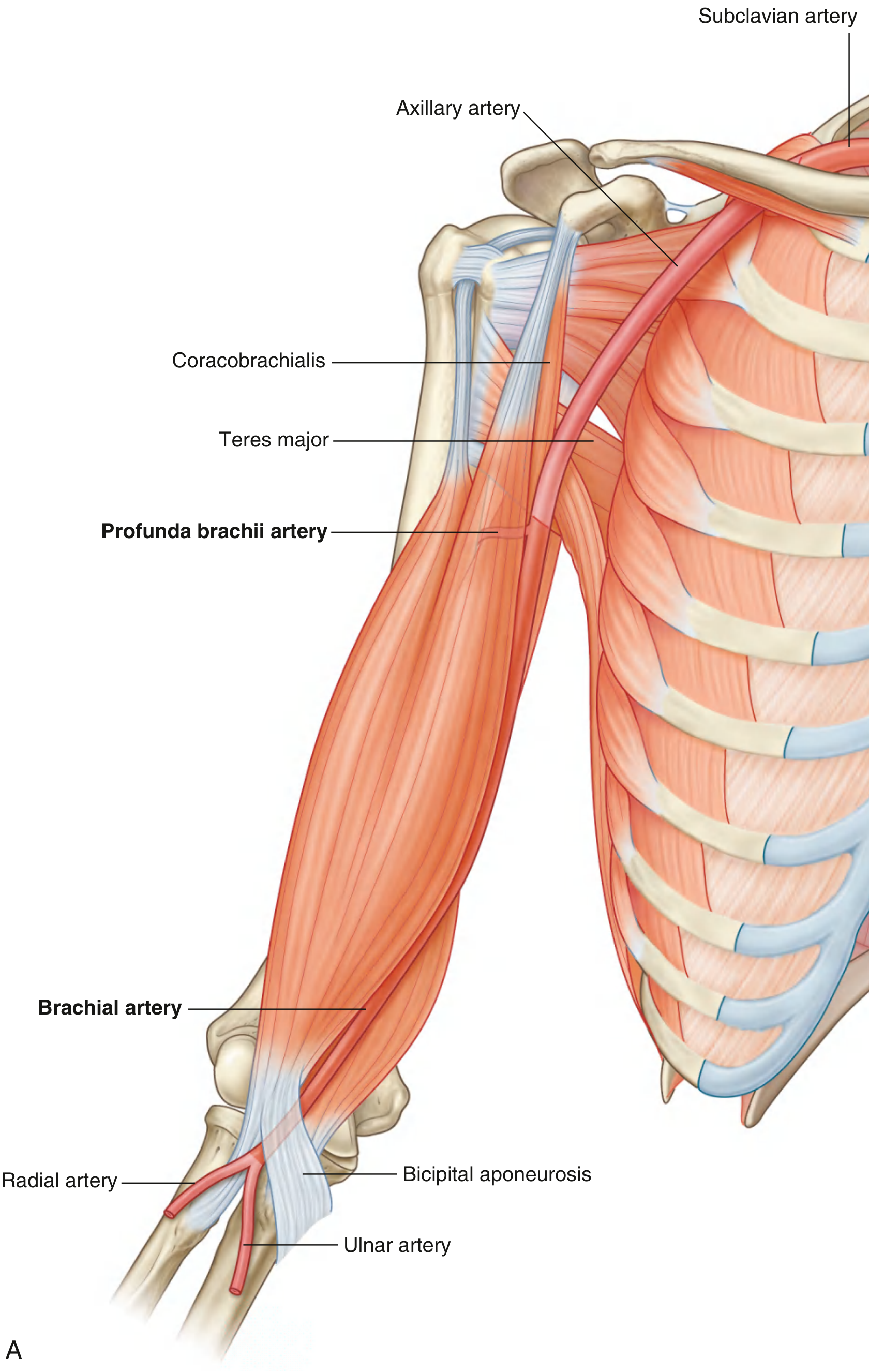
Overview and Course
Branches of the Brachial Artery
| Branch | Origin | Course and Supply |
|---|---|---|
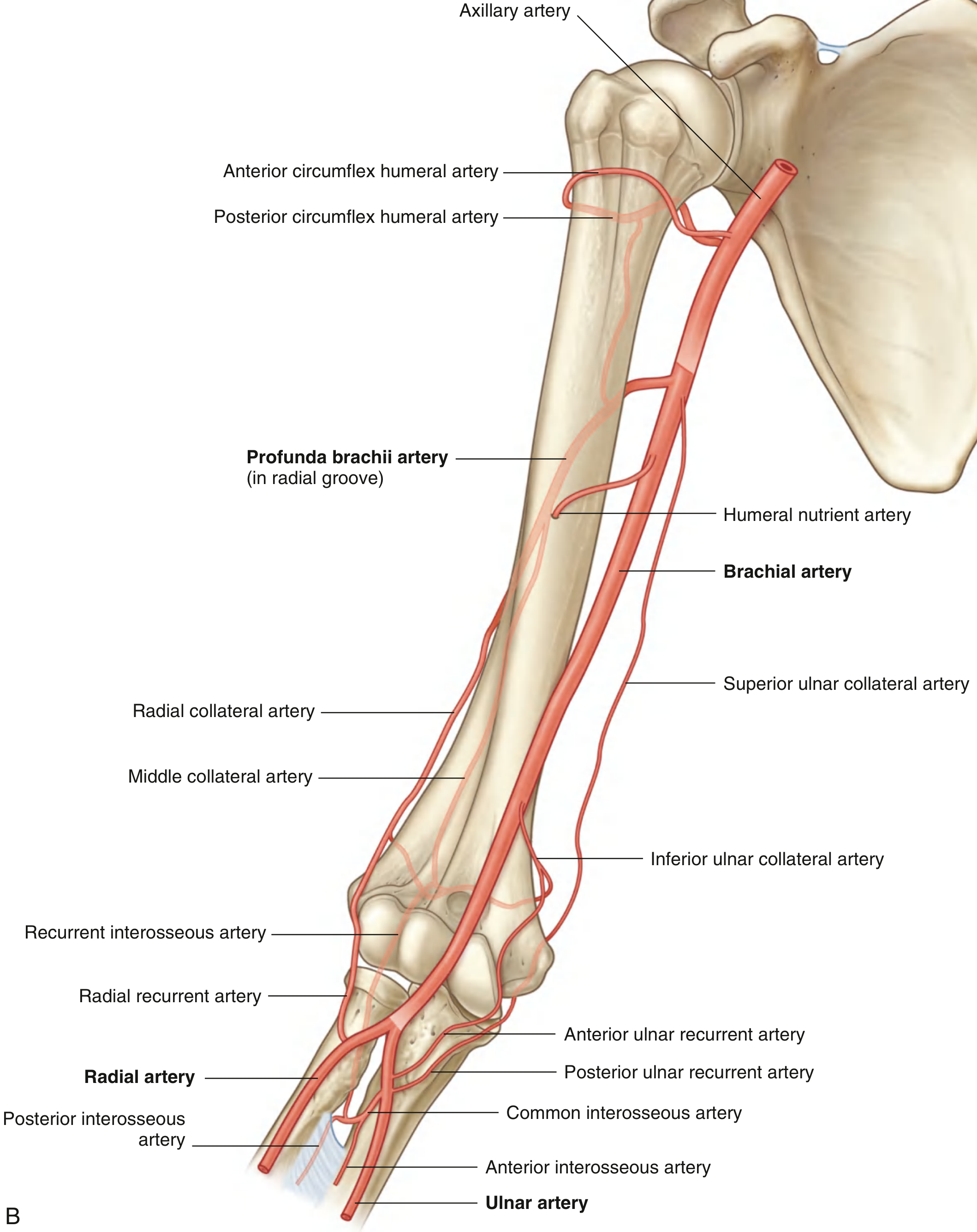
| Profunda brachii (deep brachial) artery | Largest branch; arises proximally | Enters posterior compartment with the radial nerve through the triangular interval; runs in the radial groove deep to the lateral head of triceps; supplies posterior arm muscles and anastomoses with the posterior circumflex humeral artery |
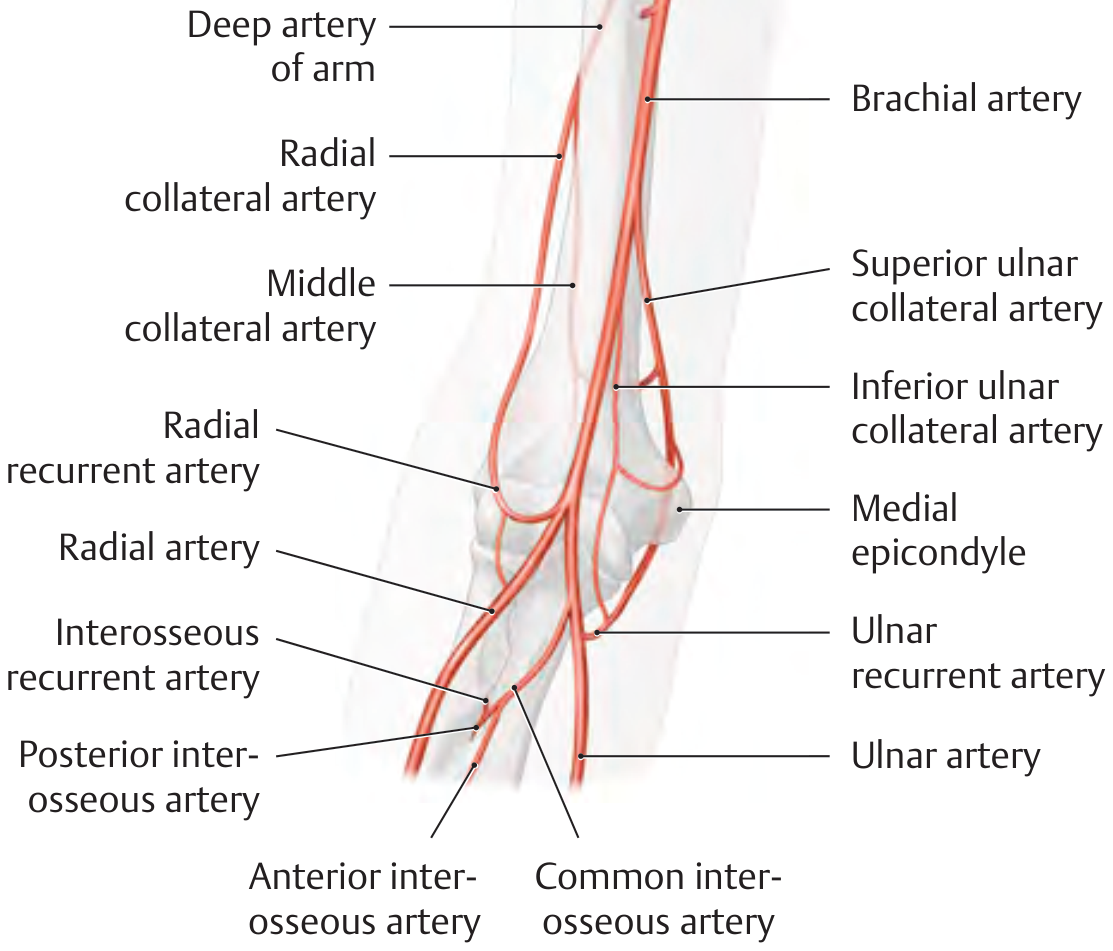
| Middle collateral artery | Terminal branch of profunda brachii | Descends to lateral/posterior elbow; anastomoses with the interosseous recurrent artery |
| Radial collateral artery | Terminal branch of profunda brachii | Accompanies radial nerve anteriorly to the lateral epicondyle; anastomoses with the radial recurrent artery |
| Superior ulnar collateral artery | Brachial artery, mid-arm | Follows ulnar nerve around medial epicondyle to posterior elbow; anastomoses with posterior ulnar recurrent artery |
| Inferior ulnar collateral artery | Brachial artery, distal arm | Passes anterior to medial epicondyle; anastomoses with anterior ulnar recurrent artery |
| Muscular branches | Along the course | Supply the biceps brachii, brachialis, and coracobrachialis |
| Humeral nutrient artery | Variable | Enters nutrient foramen on anteromedial surface of humeral shaft |
The Arterial Network (Anastomosis) Around the Elbow
Contributions to the network:
- Radial collateral artery (lateral side)
- Middle collateral artery (posterior side)
- Superior ulnar collateral artery (medial/posterior)
- Inferior ulnar collateral artery (medial/anterior)
- Radial recurrent artery (from radial a.) - anastomoses with radial collateral
- Interosseous recurrent artery (from posterior interosseous a.) - anastomoses with middle collateral
- Anterior ulnar recurrent artery (from ulnar a.) - anastomoses with inferior ulnar collateral
- Posterior ulnar recurrent artery (from ulnar a.) - anastomoses with superior ulnar collateral
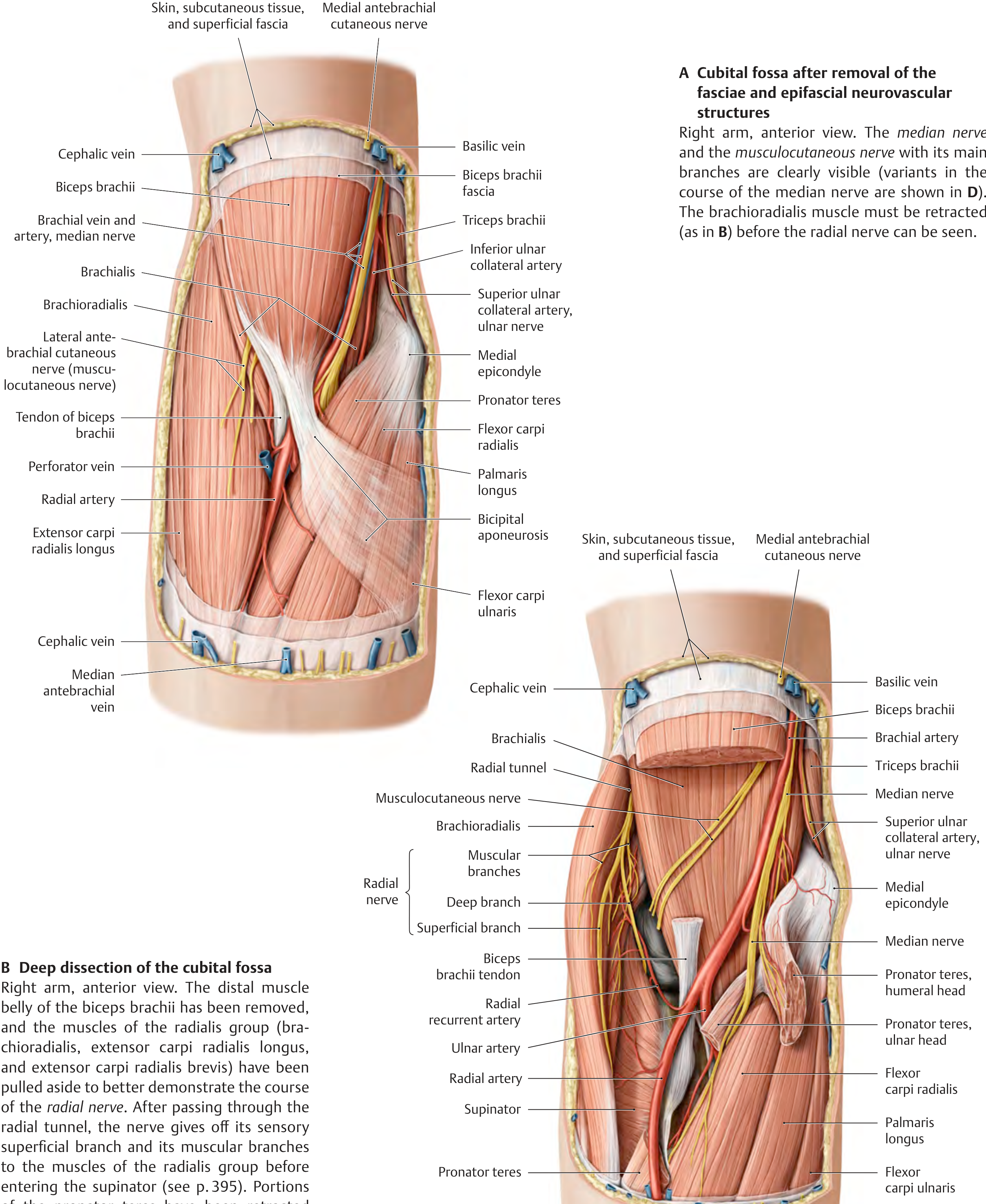
Cubital Fossa Relationships
Clinical Significance
-
Ligation safety: The brachial artery can be safely ligated distal to the origin of the profunda brachii because the periarticular anastomotic network provides adequate collateral circulation to the forearm. - THIEME Atlas of Anatomy, p. 394
-
Blood pressure measurement: The brachial artery is compressed against the humerus in the mid-arm when using a sphygmomanometer; the pulse is auscultated in the cubital fossa. - Gray's Anatomy for Students, p. 876
-
Variant anatomy: In ~20% of individuals, the brachial artery gives off a superficial brachial artery that courses superficial to the median nerve. This can present as a high-origin radial artery (10%), high-origin ulnar artery (3%), or early bifurcation (7%). - Fischer's Mastery of Surgery, p. 6991
-
Supracondylar process: A rare anomaly (0.7%) - a bony outgrowth above the medial epicondyle connected by Struthers' ligament can create a fibro-osseous canal that traps both the brachial artery and median nerve.
-
Elbow dislocation/fracture: Despite complete brachial artery disruption, the hand may remain well perfused due to the rich collateral network. - Campbell's Operative Orthopaedics, 15th Ed 2026
Just draw me a table for management of pink pulseless supracondylar humerus fracture.
Management of Pink Pulseless Hand in Supracondylar Humerus Fracture
Definition: The hand is pink and warm (adequate perfusion via collaterals) but the radial pulse is absent. This distinguishes it from the white/pale pulseless hand, which is a true vascular emergency with absent perfusion.
| Step | Action | Detail |
|---|---|---|
| 1. Initial assessment | Confirm hand is pink and warm | Check capillary refill, skin colour, temperature - perfusion present despite absent pulse |
| 2. First-line treatment | Urgent CRPP (Closed Reduction + Percutaneous Pinning) | Reduction often relieves arterial kinking or spasm; pulse returns in the majority of cases after reduction |
| 3. Post-reduction: pulse returns | Inpatient observation + splinting | Monitor hourly neurovascular checks; no further vascular intervention needed |
| 4. Post-reduction: pulse still absent but hand remains pink | Inpatient observation + splinting | Continue close monitoring; collateral flow is maintaining perfusion |
| 5. Hand becomes poorly perfused at any point | Vascular surgery consultation | Proceed to surgical exploration of brachial artery (arteriotomy / repair) |
| 6. Arteriography | Generally not warranted | Location of injury (brachial artery at fracture site) is almost always known |
Key Points
| Feature | Pink Pulseless | White/Pale Pulseless |
|---|---|---|
| Hand perfusion | Maintained (collaterals intact) | Absent |
| Urgency | Urgent (not emergent) | Emergent |
| First step | CRPP | Emergent CRPP |
| Vascular exploration | Only if hand becomes poorly perfused | If perfusion not restored after CRPP |
| Prognosis | Pulse returns in most after reduction | Higher risk of ischaemia / arterial repair needed |
Create a quick-reference PDF on supracondylar fracture complications
mkdir -p /home/daytona/workspace/supracondylar-pdf && python3 - << 'PYEOF' from reportlab.lib.pagesizes import A4 from reportlab.lib import colors from reportlab.lib.units import cm from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle from reportlab.platypus import (SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle, HRFlowable, KeepTogether) from reportlab.lib.enums import TA_CENTER, TA_LEFT, TA_JUSTIFY OUTPUT = "/home/daytona/workspace/supracondylar-pdf/Supracondylar_Fracture_Complications.pdf" doc = SimpleDocTemplate( OUTPUT, pagesize=A4, rightMargin=1.8*cm, leftMargin=1.8*cm, topMargin=1.5*cm, bottomMargin=1.5*cm, title="Supracondylar Fracture – Complications Quick Reference", author="Orris Medical Reference" ) W = A4[0] - 3.6*cm # usable width # ── colour palette ──────────────────────────────────────────────────────────── NAVY = colors.HexColor("#1A3A5C") TEAL = colors.HexColor("#1B7A8A") AMBER = colors.HexColor("#E8881A") RED = colors.HexColor("#C0392B") GREEN = colors.HexColor("#1E8449") LGREY = colors.HexColor("#F2F5F7") MGREY = colors.HexColor("#D5DDE5") WHITE = colors.white BLACK = colors.HexColor("#1A1A1A") # ── styles ──────────────────────────────────────────────────────────────────── styles = getSampleStyleSheet() def S(name, **kw): return ParagraphStyle(name, **kw) titleStyle = S("Title", fontSize=20, leading=26, textColor=WHITE, fontName="Helvetica-Bold", alignment=TA_CENTER, spaceAfter=0) subtitleStyle = S("Sub", fontSize=10, leading=14, textColor=colors.HexColor("#CFE2F0"), fontName="Helvetica", alignment=TA_CENTER) sectionHead = S("SecHead", fontSize=11, leading=15, textColor=WHITE, fontName="Helvetica-Bold", alignment=TA_LEFT, spaceAfter=0) body = S("Body", fontSize=8.5, leading=13, textColor=BLACK, fontName="Helvetica", spaceAfter=2) bodyB = S("BodyB", fontSize=8.5, leading=13, textColor=BLACK, fontName="Helvetica-Bold", spaceAfter=2) small = S("Small", fontSize=7.5, leading=11, textColor=colors.HexColor("#444444"), fontName="Helvetica-Oblique") bullet = S("Bullet", fontSize=8.5, leading=13, textColor=BLACK, fontName="Helvetica", leftIndent=10, bulletIndent=0, spaceAfter=1) tableHead = S("TH", fontSize=8.5, leading=12, textColor=WHITE, fontName="Helvetica-Bold", alignment=TA_CENTER) tableCell = S("TC", fontSize=8, leading=11, textColor=BLACK, fontName="Helvetica", alignment=TA_LEFT) tableCellC = S("TCC", fontSize=8, leading=11, textColor=BLACK, fontName="Helvetica", alignment=TA_CENTER) tableCellB = S("TCB", fontSize=8, leading=11, textColor=BLACK, fontName="Helvetica-Bold", alignment=TA_LEFT) footerStyle = S("Footer", fontSize=7, leading=10, textColor=colors.HexColor("#888888"), fontName="Helvetica-Oblique", alignment=TA_CENTER) # ── helper: section header row ───────────────────────────────────────────── def sec_header(title, color=NAVY): tbl = Table([[Paragraph(title, sectionHead)]], colWidths=[W]) tbl.setStyle(TableStyle([ ("BACKGROUND", (0,0), (-1,-1), color), ("TOPPADDING", (0,0), (-1,-1), 5), ("BOTTOMPADDING",(0,0),(-1,-1), 5), ("LEFTPADDING", (0,0), (-1,-1), 8), ("RIGHTPADDING",(0,0), (-1,-1), 8), ])) return tbl def b(txt): return f"<b>{txt}</b>" def i(txt): return f"<i>{txt}</i>" def col(txt, c): return f'<font color="{c}">{txt}</font>' # ── STORY ───────────────────────────────────────────────────────────────────── story = [] # ── TITLE BANNER ────────────────────────────────────────────────────────────── banner_data = [[ Paragraph("Supracondylar Humerus Fracture", titleStyle), Paragraph("Complications – Quick Reference", titleStyle), ]] # Use two rows banner1 = Table([[Paragraph("Supracondylar Humerus Fracture", titleStyle)]], colWidths=[W]) banner1.setStyle(TableStyle([ ("BACKGROUND",(0,0),(-1,-1), NAVY), ("TOPPADDING",(0,0),(-1,-1), 10), ("BOTTOMPADDING",(0,0),(-1,-1), 2), ("LEFTPADDING",(0,0),(-1,-1), 8), ])) banner2 = Table([[Paragraph("Complications Quick Reference", subtitleStyle)]], colWidths=[W]) banner2.setStyle(TableStyle([ ("BACKGROUND",(0,0),(-1,-1), NAVY), ("TOPPADDING",(0,0),(-1,-1), 0), ("BOTTOMPADDING",(0,0),(-1,-1), 10), ("LEFTPADDING",(0,0),(-1,-1), 8), ])) story += [banner1, banner2, Spacer(1, 0.3*cm)] # ── SOURCE PILL ─────────────────────────────────────────────────────────────── src = Table([[Paragraph( i("Sources: Campbell's Operative Orthopaedics 15th Ed 2026 · Miller's Review of Orthopaedics 9th Ed · " "Bailey & Love's 28th Ed · Rosen's Emergency Medicine"), small)]], colWidths=[W]) src.setStyle(TableStyle([ ("BACKGROUND",(0,0),(-1,-1), LGREY), ("TOPPADDING",(0,0),(-1,-1), 4),("BOTTOMPADDING",(0,0),(-1,-1), 4), ("LEFTPADDING",(0,0),(-1,-1), 8),("ROUNDEDCORNERS",[3]*4), ])) story += [src, Spacer(1, 0.35*cm)] # ════════════════════════════════════════════════════════════════════════════ # SECTION 1 – OVERVIEW BOX # ════════════════════════════════════════════════════════════════════════════ story.append(sec_header("1. Overview")) story.append(Spacer(1, 0.2*cm)) overview_data = [ [Paragraph(b("Epidemiology"), tableHead), Paragraph(b("Mechanism"), tableHead), Paragraph(b("Classification"), tableHead)], [Paragraph("Most common elbow fracture in children (peak age 5–7 yrs). Rate: 60–70/100,000 children. 98% extension-type. 5–10% have ipsilateral distal radius fracture.", tableCell), Paragraph("Fall on outstretched hand (FOOSH) in extension → posterior displacement of distal fragment. Flexion-type (2%): fall on flexed elbow.", tableCell), Paragraph("<b>Gartland Classification:</b><br/>I – Non-displaced<br/>II – Intact posterior hinge (IIA stable, IIB unstable)<br/>III – Complete displacement<br/>IV – Unstable in flexion & extension (high-energy)", tableCell)], ] ov_tbl = Table(overview_data, colWidths=[W*0.32, W*0.32, W*0.36]) ov_tbl.setStyle(TableStyle([ ("BACKGROUND",(0,0),(-1,0), TEAL), ("BACKGROUND",(0,1),(-1,1), LGREY), ("GRID",(0,0),(-1,-1), 0.4, MGREY), ("TOPPADDING",(0,0),(-1,-1), 5),("BOTTOMPADDING",(0,0),(-1,-1), 5), ("LEFTPADDING",(0,0),(-1,-1), 6),("RIGHTPADDING",(0,0),(-1,-1), 6), ("VALIGN",(0,0),(-1,-1), "TOP"), ])) story += [ov_tbl, Spacer(1, 0.35*cm)] # ════════════════════════════════════════════════════════════════════════════ # SECTION 2 – COMPLICATIONS TABLE (main) # ════════════════════════════════════════════════════════════════════════════ story.append(sec_header("2. Complications at a Glance", color=RED)) story.append(Spacer(1, 0.2*cm)) hdr = [Paragraph(b("Complication"), tableHead), Paragraph(b("Incidence"), tableHead), Paragraph(b("Mechanism / Notes"), tableHead), Paragraph(b("Management"), tableHead)] rows = [ # Vascular [Paragraph(col(b("VASCULAR INJURY"), "#C0392B"), tableCellB), Paragraph("10–20% (type III)", tableCell), Paragraph("Brachial artery kinking, spasm, or laceration. Anterior sharp end of proximal fragment injures artery.", tableCell), Paragraph("See Section 3 (vascular algorithm)", tableCell)], # Compartment syndrome [Paragraph(col(b("Compartment Syndrome"), "#C0392B"), tableCellB), Paragraph("0.1–0.3%", tableCell), Paragraph("Higher risk with floating elbow (concurrent forearm/wrist fracture). Prolonged ischemia → Volkmann contracture.", tableCell), Paragraph("Early recognition (3 As: Agitation, Anxiety, Analgesia↑). Urgent fasciotomy (forearm + hand).", tableCell)], # Volkmann [Paragraph(col(b("Volkmann Ischemic Contracture"), "#8E1A0E"), tableCellB), Paragraph("Rare; most serious", tableCell), Paragraph("End-result of untreated compartment syndrome or prolonged ischemia. Ischemic fibrosis of flexor muscles of forearm.", tableCell), Paragraph("Prevention is key. Prophylactic fasciotomy if prolonged ischemia. Established: muscle slide, Z-plasty, tendon lengthening.", tableCell)], # Nerve – AIN [Paragraph(col(b("Anterior Interosseous Nerve (AIN) Injury"), "#1B7A8A"), tableCellB), Paragraph("Most common nerve (extension-type)", tableCell), Paragraph("Neurapraxia from stretch/compression. Tests: FPL (can't make 'OK' sign), FDP index, pronator quadratus.", tableCell), Paragraph("Observe – 95%+ resolve in 6–12 wks. EMG if no recovery at 3 months.", tableCell)], # Nerve – Radial [Paragraph(col(b("Radial Nerve Injury"), "#1B7A8A"), tableCellB), Paragraph("~10% overall; ↑ with displacement", tableCell), Paragraph("Usually neurapraxia. 100% long-term recovery in most series.", tableCell), Paragraph("Conservative; 6–12 wk recovery. EMG if no return at 3 months.", tableCell)], # Nerve – Median [Paragraph(col(b("Median Nerve Injury"), "#1B7A8A"), tableCellB), Paragraph("Extension-type", tableCell), Paragraph("Usually neurapraxia. 88% fully recover long-term.", tableCell), Paragraph("Conservative management. Observe for 6–12 weeks.", tableCell)], # Nerve – Ulnar [Paragraph(col(b("Ulnar Nerve Injury"), "#1B7A8A"), tableCellB), Paragraph("Flexion-type (10%); iatrogenic 3–8% with medial pin", tableCell), Paragraph("Flexion-type: direct injury. Iatrogenic: medial pin placement. Worst prognosis – only 25% full recovery.", tableCell), Paragraph("If iatrogenic: small incision + retractors to protect nerve. Avoid pinning in maximal flexion. EMG at 3 months if no recovery.", tableCell)], # Cubitus varus [Paragraph(col(b("Cubitus Varus (Gunstock Deformity)"), "#1E8449"), tableCellB), Paragraph("Most common late complication", tableCell), Paragraph("Due to malunion (NOT growth arrest). Poor cosmesis. Generally does not affect function, but can predispose to lateral condyle fracture.", tableCell), Paragraph("Prevention: anatomic reduction + adequate pin fixation. Correction: lateral closing-wedge supracondylar osteotomy.", tableCell)], # Cubitus valgus [Paragraph(col(b("Cubitus Valgus"), "#1E8449"), tableCellB), Paragraph("Less common malunion", tableCell), Paragraph("Malunion in valgus. Can lead to tardy ulnar nerve palsy (late presentation).", tableCell), Paragraph("Prevention: adequate reduction. Correction osteotomy if symptomatic. Monitor for ulnar nerve function.", tableCell)], # Recurvatum [Paragraph(col(b("Recurvatum (Hyperextension)"), "#1E8449"), tableCellB), Paragraph("Uncommon", tableCell), Paragraph("Poorly tolerated deformity. Due to anterior malunion or pin failure.", tableCell), Paragraph("Flex-type osteotomy for correction. Prevention by adequate CRPP.", tableCell)], # Pin complications [Paragraph(col(b("Pin Complications"), "#7D6608"), tableCellB), Paragraph("~5% of percutaneous pinning", tableCell), Paragraph("Pin migration or irritation (most common), infection (~1%), elbow stiffness.", tableCell), Paragraph("Pin removal at 3–4 weeks. Wound care. Early mobilisation after removal.", tableCell)], # Elbow stiffness [Paragraph(col(b("Elbow Stiffness / Loss of Motion"), "#555555"), tableCellB), Paragraph("Variable", tableCell), Paragraph("More common after delayed reduction, open reduction, or prolonged immobilisation.", tableCell), Paragraph("Physiotherapy after pin removal. Usually resolves in children within 6–12 months.", tableCell)], # Avascular necrosis [Paragraph(col(b("Avascular Necrosis (Trochlea/Capitellum)"), "#555555"), tableCellB), Paragraph("Rare", tableCell), Paragraph("Disruption of blood supply during high-energy injury or open reduction.", tableCell), Paragraph("Monitor radiographically. Late reconstruction if significant joint deformity.", tableCell)], # Growth arrest [Paragraph(col(b("Growth Disturbance"), "#555555"), tableCellB), Paragraph("Rare in supracondylar (physis not crossed)", tableCell), Paragraph("Unlike lateral condyle fractures, true growth arrest is uncommon because the fracture is usually metaphyseal above the physis.", tableCell), Paragraph("Long-term follow-up radiographs.", tableCell)], ] comp_tbl = Table([hdr] + rows, colWidths=[W*0.22, W*0.13, W*0.35, W*0.30]) comp_style = [ ("BACKGROUND",(0,0),(-1,0), NAVY), ("GRID",(0,0),(-1,-1), 0.3, MGREY), ("TOPPADDING",(0,0),(-1,-1), 4), ("BOTTOMPADDING",(0,0),(-1,-1), 4), ("LEFTPADDING",(0,0),(-1,-1), 5), ("RIGHTPADDING",(0,0),(-1,-1), 5), ("VALIGN",(0,0),(-1,-1), "TOP"), # alternating rows ] for i_row in range(1, len(rows)+1): if i_row % 2 == 0: comp_style.append(("BACKGROUND",(0,i_row),(-1,i_row), LGREY)) comp_tbl.setStyle(TableStyle(comp_style)) story += [comp_tbl, Spacer(1, 0.35*cm)] # ════════════════════════════════════════════════════════════════════════════ # SECTION 3 – VASCULAR ALGORITHM # ════════════════════════════════════════════════════════════════════════════ story.append(sec_header("3. Vascular Injury Algorithm", color=RED)) story.append(Spacer(1, 0.2*cm)) alg_data = [ [Paragraph(b("Clinical Status"), tableHead), Paragraph(b("Urgency"), tableHead), Paragraph(b("First Step"), tableHead), Paragraph(b("If Pulse Returns"), tableHead), Paragraph(b("If Pulse Absent / Perfusion Lost"), tableHead)], [Paragraph(col(b("Pink Pulseless Hand"),"#E8881A")+"<br/><i>(warm, perfused, no radial pulse)</i>", tableCell), Paragraph(col(b("URGENT"),"#E8881A"), tableCellC), Paragraph("Urgent CRPP", tableCell), Paragraph("Inpatient observation + splinting. Most resolve with reduction.", tableCell), Paragraph("Vascular surgery consult. Consider brachial artery exploration.", tableCell)], [Paragraph(col(b("White/Pale Pulseless Hand"),"#C0392B")+"<br/><i>(cold, non-perfused, no pulse)</i>", tableCell), Paragraph(col(b("EMERGENT"),"#C0392B"), tableCellC), Paragraph("Emergent CRPP (no arteriography – injury site is known)", tableCell), Paragraph("Inpatient observation. Monitor hourly.", tableCell), Paragraph("Urgent brachial artery exploration → release entrapping structures → direct repair ± vein graft. Prophylactic forearm + hand fasciotomy if prolonged ischaemia.", tableCell)], ] alg_col_w = [W*0.20, W*0.09, W*0.16, W*0.25, W*0.30] alg_tbl = Table(alg_data, colWidths=alg_col_w) alg_tbl.setStyle(TableStyle([ ("BACKGROUND",(0,0),(-1,0), RED), ("BACKGROUND",(0,1),(-1,1), colors.HexColor("#FEF5E7")), ("BACKGROUND",(0,2),(-1,2), colors.HexColor("#FDEDEC")), ("GRID",(0,0),(-1,-1), 0.4, MGREY), ("TOPPADDING",(0,0),(-1,-1), 4),("BOTTOMPADDING",(0,0),(-1,-1), 4), ("LEFTPADDING",(0,0),(-1,-1), 5),("RIGHTPADDING",(0,0),(-1,-1), 5), ("VALIGN",(0,0),(-1,-1), "TOP"), ])) story += [alg_tbl, Spacer(1, 0.35*cm)] # ════════════════════════════════════════════════════════════════════════════ # SECTION 4 – NERVE INJURY SUMMARY # ════════════════════════════════════════════════════════════════════════════ story.append(sec_header("4. Nerve Injury Summary", color=TEAL)) story.append(Spacer(1, 0.2*cm)) nerve_data = [ [Paragraph(b("Nerve"), tableHead), Paragraph(b("Fracture Type"), tableHead), Paragraph(b("Clinical Test"), tableHead), Paragraph(b("Prognosis"), tableHead), Paragraph(b("Key Point"), tableHead)], [Paragraph("Anterior Interosseous N.", tableCell), Paragraph("Extension (most common)", tableCell), Paragraph("Cannot flex IP of thumb (FPL) or DIP of index (FDP). Cannot make 'OK' sign.", tableCell), Paragraph(col("Excellent","#1E8449"), tableCellC), Paragraph("Usually neurapraxia. Resolves 6–12 wks.", tableCell)], [Paragraph("Radial Nerve", tableCell), Paragraph("Extension-type", tableCell), Paragraph("Wrist drop, loss of finger extension, loss of sensation dorsal 1st web space.", tableCell), Paragraph(col("Excellent (100%)","#1E8449"), tableCellC), Paragraph("Neurapraxia. Best prognosis of all nerve injuries.", tableCell)], [Paragraph("Median Nerve", tableCell), Paragraph("Extension-type", tableCell), Paragraph("Thenar wasting, loss of opposition, sensory loss over lateral 3½ fingers.", tableCell), Paragraph(col("Good (88%)","#1E8449"), tableCellC), Paragraph("Usually neurapraxia.", tableCell)], [Paragraph("Ulnar Nerve", tableCell), Paragraph("Flexion-type (direct); medial pin placement (iatrogenic)", tableCell), Paragraph("Clawing ring/little finger, loss of intrinsics, sensory loss medial 1½ fingers.", tableCell), Paragraph(col(b("Poor (25%)"), "#C0392B"), tableCellC), Paragraph("Worst prognosis. Avoid medial pin in flexion. Protect with small incision.", tableCell)], ] nerve_tbl = Table(nerve_data, colWidths=[W*0.18, W*0.17, W*0.25, W*0.14, W*0.26]) nerve_style = [ ("BACKGROUND",(0,0),(-1,0), TEAL), ("GRID",(0,0),(-1,-1), 0.3, MGREY), ("TOPPADDING",(0,0),(-1,-1), 4),("BOTTOMPADDING",(0,0),(-1,-1), 4), ("LEFTPADDING",(0,0),(-1,-1), 5),("RIGHTPADDING",(0,0),(-1,-1), 5), ("VALIGN",(0,0),(-1,-1), "TOP"), ] for i_row in range(1, 5): if i_row % 2 == 0: nerve_style.append(("BACKGROUND",(0,i_row),(-1,i_row), LGREY)) nerve_tbl.setStyle(TableStyle(nerve_style)) story += [nerve_tbl, Spacer(1, 0.35*cm)] # ════════════════════════════════════════════════════════════════════════════ # SECTION 5 – ANGULAR DEFORMITY # ════════════════════════════════════════════════════════════════════════════ story.append(sec_header("5. Angular Deformity (Late Complications)", color=GREEN)) story.append(Spacer(1, 0.2*cm)) ang_data = [ [Paragraph(b("Deformity"), tableHead), Paragraph(b("Cause"), tableHead), Paragraph(b("Clinical Features"), tableHead), Paragraph(b("Treatment"), tableHead), Paragraph(b("Notes"), tableHead)], [Paragraph(col(b("Cubitus Varus"), "#C0392B"), tableCellB), Paragraph("Malunion (NOT growth arrest)", tableCell), Paragraph("'Gunstock deformity'. Cosmetic; rarely affects function. Can predispose to later lateral condyle fracture.", tableCell), Paragraph("Lateral closing-wedge supracondylar osteotomy when symptomatic or severe.", tableCell), Paragraph("Most common late complication of supracondylar fractures.", tableCell)], [Paragraph(col(b("Cubitus Valgus"), "#E8881A"), tableCellB), Paragraph("Malunion in valgus", tableCell), Paragraph("Carrying angle increased. Risk of tardy ulnar nerve palsy (years later).", tableCell), Paragraph("Osteotomy if symptomatic. Ulnar nerve transposition if tardy palsy develops.", tableCell), Paragraph("Monitor ulnar nerve function at follow-up.", tableCell)], [Paragraph(col(b("Recurvatum"), "#555555"), tableCellB), Paragraph("Anterior malunion / pin failure", tableCell), Paragraph("Hyperextension deformity. Poorly tolerated functionally.", tableCell), Paragraph("Flexion-type corrective osteotomy.", tableCell), Paragraph("Rare. Prevention by ensuring adequate anterior cortical apposition.", tableCell)], ] ang_tbl = Table(ang_data, colWidths=[W*0.15, W*0.17, W*0.25, W*0.23, W*0.20]) ang_tbl.setStyle(TableStyle([ ("BACKGROUND",(0,0),(-1,0), GREEN), ("BACKGROUND",(0,1),(-1,1), colors.HexColor("#FDEDEC")), ("BACKGROUND",(0,2),(-1,2), colors.HexColor("#FEF5E7")), ("BACKGROUND",(0,3),(-1,3), LGREY), ("GRID",(0,0),(-1,-1), 0.3, MGREY), ("TOPPADDING",(0,0),(-1,-1), 4),("BOTTOMPADDING",(0,0),(-1,-1), 4), ("LEFTPADDING",(0,0),(-1,-1), 5),("RIGHTPADDING",(0,0),(-1,-1), 5), ("VALIGN",(0,0),(-1,-1), "TOP"), ])) story += [ang_tbl, Spacer(1, 0.35*cm)] # ════════════════════════════════════════════════════════════════════════════ # SECTION 6 – CLINICAL PEARLS # ════════════════════════════════════════════════════════════════════════════ story.append(sec_header("6. Clinical Pearls", color=AMBER)) story.append(Spacer(1, 0.2*cm)) pearls = [ ("Compartment Syndrome Watch", "In children: the '3 As' – Agitation, Anxiety, increasing Analgesia requirements are the most sensitive indicators of impending compartment syndrome."), ("Timing of Surgery", "No difference in complication rates between urgent (<12 h) or delayed (>12 h) treatment for type III – but only if neurovascular exam is stable and closely monitored."), ("Pin Configuration", "Two or three lateral divergent pins = equivalent to crossed pins in clinical outcomes, but with lower iatrogenic nerve injury rate (lateral: ~0% vs medial pin: 3–8%)."), ("Arteriography", "Generally NOT warranted in supracondylar fractures – location of injury is known. Never delay closed reduction for arteriography."), ("Nerve Loss After Reduction", "New neurological deficit after reduction = suspect nerve entrapment. Urgent open exploration is necessary."), ("Ligation Safety", "Brachial artery can be ligated distal to profunda brachii origin if needed – periarticular collateral network maintains forearm perfusion."), ("Radiographic Clues", "Posterior fat pad sign or abnormal anterior humeral line (should transect middle third of capitellum) = presumptive evidence of fracture even if subtle."), ("Cubitus Varus ≠ Growth Arrest", "Cubitus varus is due to malunion (rotational ± varus reduction), NOT physeal growth arrest – an important distinction."), ] pearl_rows = [] for title, text in pearls: pearl_rows.append([ Paragraph(col(b("⬥ " + title), NAVY), tableCellB), Paragraph(text, tableCell) ]) pearl_tbl = Table(pearl_rows, colWidths=[W*0.28, W*0.72]) pearl_style = [ ("GRID",(0,0),(-1,-1), 0.3, MGREY), ("TOPPADDING",(0,0),(-1,-1), 4),("BOTTOMPADDING",(0,0),(-1,-1), 4), ("LEFTPADDING",(0,0),(-1,-1), 6),("RIGHTPADDING",(0,0),(-1,-1), 6), ("VALIGN",(0,0),(-1,-1), "TOP"), ] for i_row in range(len(pearls)): if i_row % 2 == 0: pearl_style.append(("BACKGROUND",(0,i_row),(-1,i_row), LGREY)) pearl_tbl.setStyle(TableStyle(pearl_style)) story += [pearl_tbl, Spacer(1, 0.3*cm)] # ── FOOTER ──────────────────────────────────────────────────────────────────── story.append(HRFlowable(width=W, thickness=0.5, color=MGREY)) story.append(Spacer(1, 0.1*cm)) story.append(Paragraph( "Quick Reference compiled by Orris Medical · Sources: Campbell's Operative Orthopaedics 15th Ed 2026 · " "Miller's Review of Orthopaedics 9th Ed · Bailey & Love's Short Practice of Surgery 28th Ed · " "Rosen's Emergency Medicine · For educational use only.", footerStyle)) doc.build(story) print("PDF created:", OUTPUT) PYEOF
Supracondylar Fracture Complications
PDF Document · PDF
| Section | Content |
|---|---|
| 1. Overview | Epidemiology, mechanism, Gartland classification (I–IV) |
| 2. Complications at a Glance | 14-row colour-coded table - vascular injury, compartment syndrome, Volkmann contracture, all 4 nerve injuries, cubitus varus/valgus, recurvatum, pin complications, stiffness, AVN, growth disturbance |
| 3. Vascular Injury Algorithm | Pink pulseless vs white pulseless - urgency, first step, post-reduction management |
| 4. Nerve Injury Summary | AIN, radial, median, ulnar - clinical test, prognosis (AIN/radial excellent → ulnar only 25%) |
| 5. Angular Deformity | Cubitus varus, valgus, recurvatum - cause, features, treatment |
| 6. Clinical Pearls | 8 high-yield points including the 3 As of compartment syndrome, pin configuration, arteriography rule, and cubitus varus ≠ growth arrest |
Detailed anatomy of posterolateral corner of knee joint.
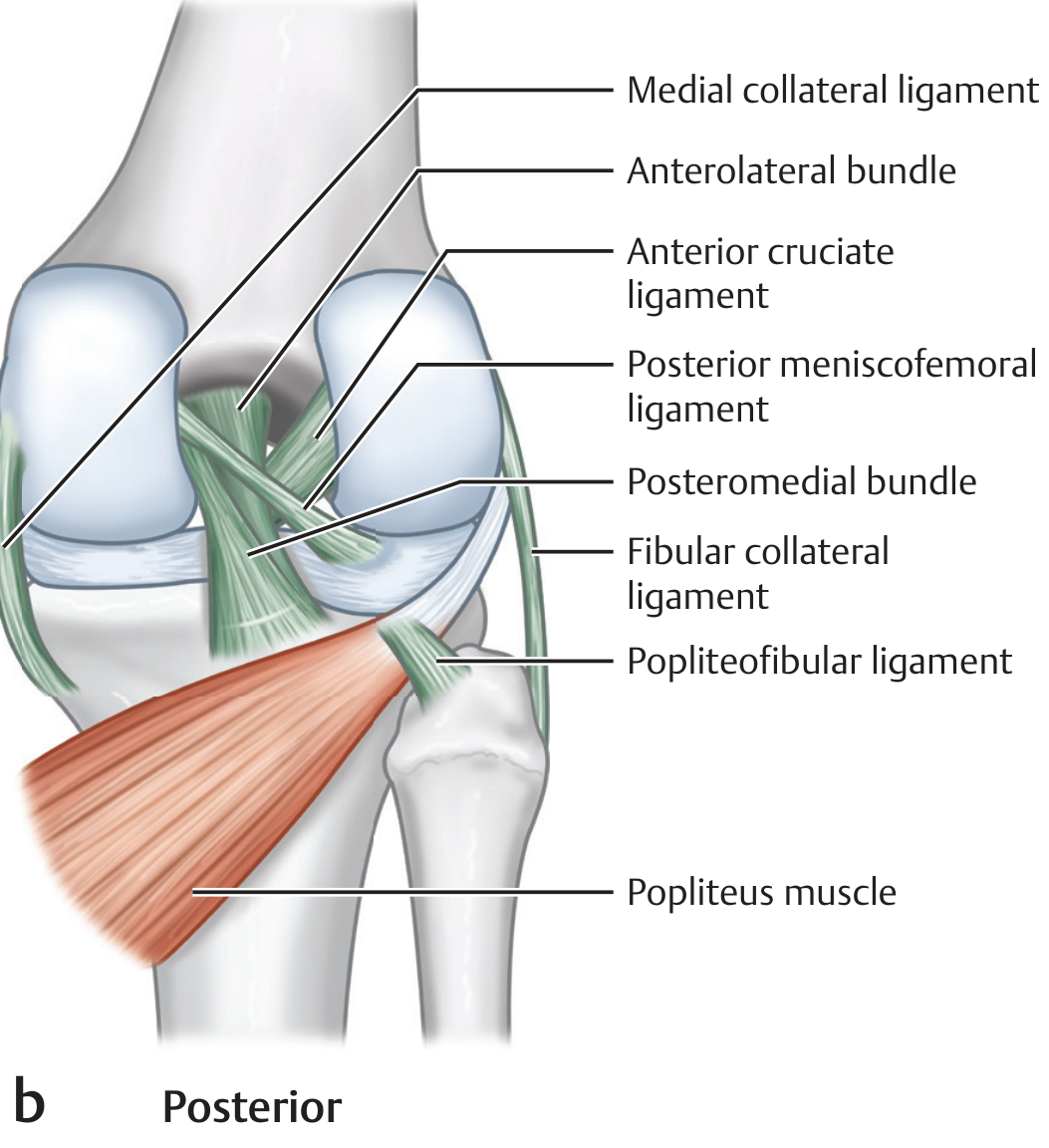
Posterolateral Corner (PLC) of the Knee - Detailed Anatomy
Anatomical Overview
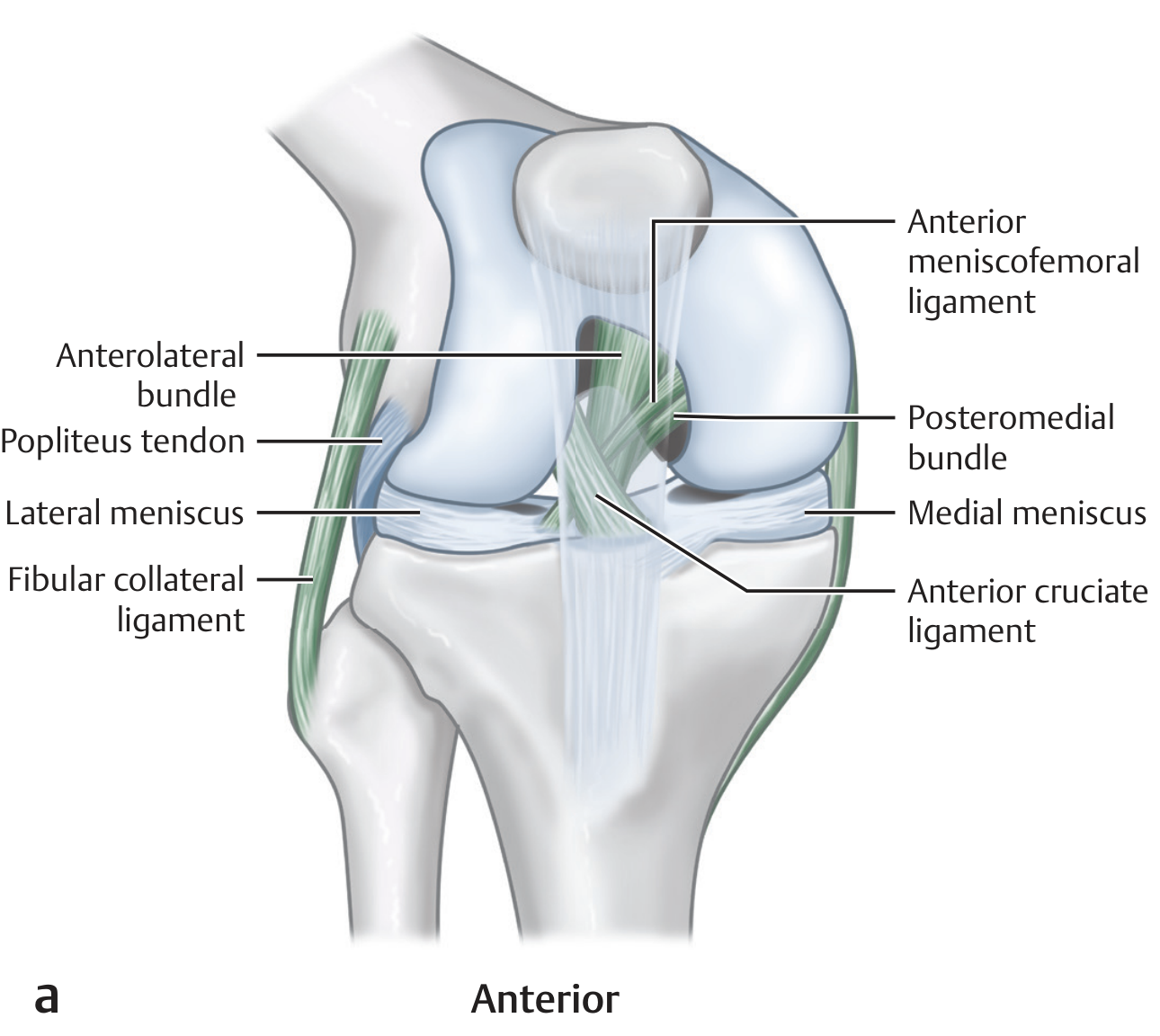
Primary Structures of the PLC
1. Fibular (Lateral) Collateral Ligament (FCL / LCL)
- Femoral origin: Proximal and posterior to the lateral femoral epicondyle; posterior, superficial, and proximal to the insertion of the popliteus tendon
- Distal insertion: Anterior to the midpoint of the lateral fibular head (8 mm posterior to the anterior margin of the fibular head, 28 mm distal to the tip of the fibular styloid) - it is the most anterior structure inserting on the proximal fibula
- Length: 63-71 mm
- Mechanics: Tight in extension, lax in flexion (lies posterior to the axis of knee rotation). Primary restraint to varus stress in all degrees of knee flexion
- Relation to biceps: The FCL cleaves the distal biceps femoris tendon immediately proximal to the fibular head - the direct and anterior arms of biceps long head become lateral to it, while the short head arms sit medial to it
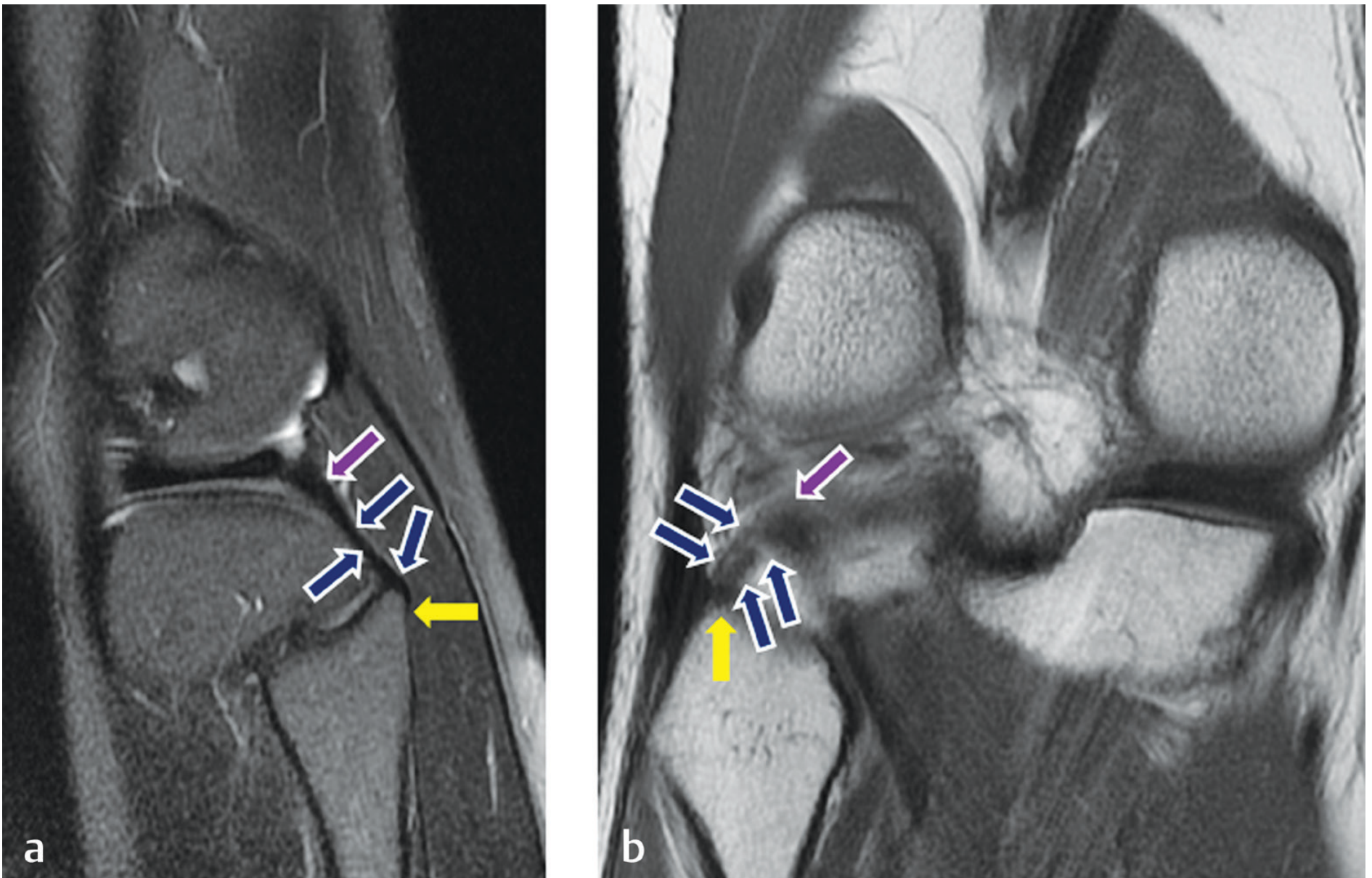
2. Popliteus Tendon
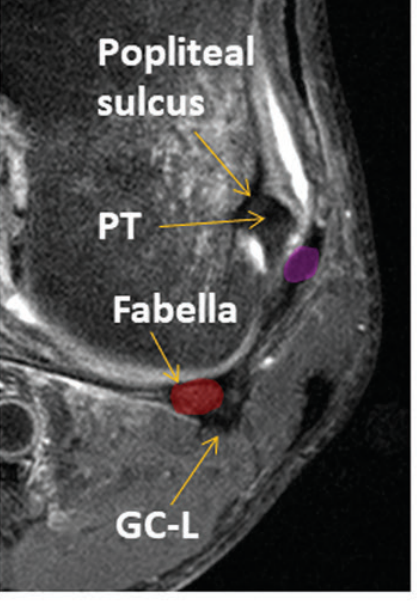
- Femoral attachment: Anterior aspect of the femoral popliteal sulcus, on the lateral femoral condyle - distal, anterior, and deep to the LCL (mnemonic: "DAD")
- Course: The tendon is intracapsular but extra-articular and extrasynovial. It passes from the popliteal sulcus inferolaterally, then curves inferomedially toward the posterior proximal tibia
- Hiatus: Traverses the coronary ligament via the popliteal hiatus (bounded by popliteomeniscal fascicles) to become intraarticular
- Muscle belly: Originates on the posterior tibia above the soleal line; the myotendinous junction lies at the lateral third of the popliteal fossa
- Function: Internally rotates the tibia; acts as a retractor of the lateral meniscus preventing impingement
3. Popliteofibular Ligament (PFL)
- Origin: Inferolateral aspect of the popliteus myotendinous junction
- Insertion: Apex of the fibular styloid process, and slightly medial to this apex - posteromedial to both the FCL and biceps femoris fibular attachments
- Fibular attachment order (anterior to posterior): LCL → PFL → Biceps femoris
- Structure: Two divisions (anterior and posterior) described; the posterior is more substantive
- Significance: A fairly constant structure; biomechanical studies show the FCL, popliteus tendon, and PFL together are the most important stabilisers of the PLC
Secondary / Accessory Structures
| Structure | Description | Status |
|---|---|---|
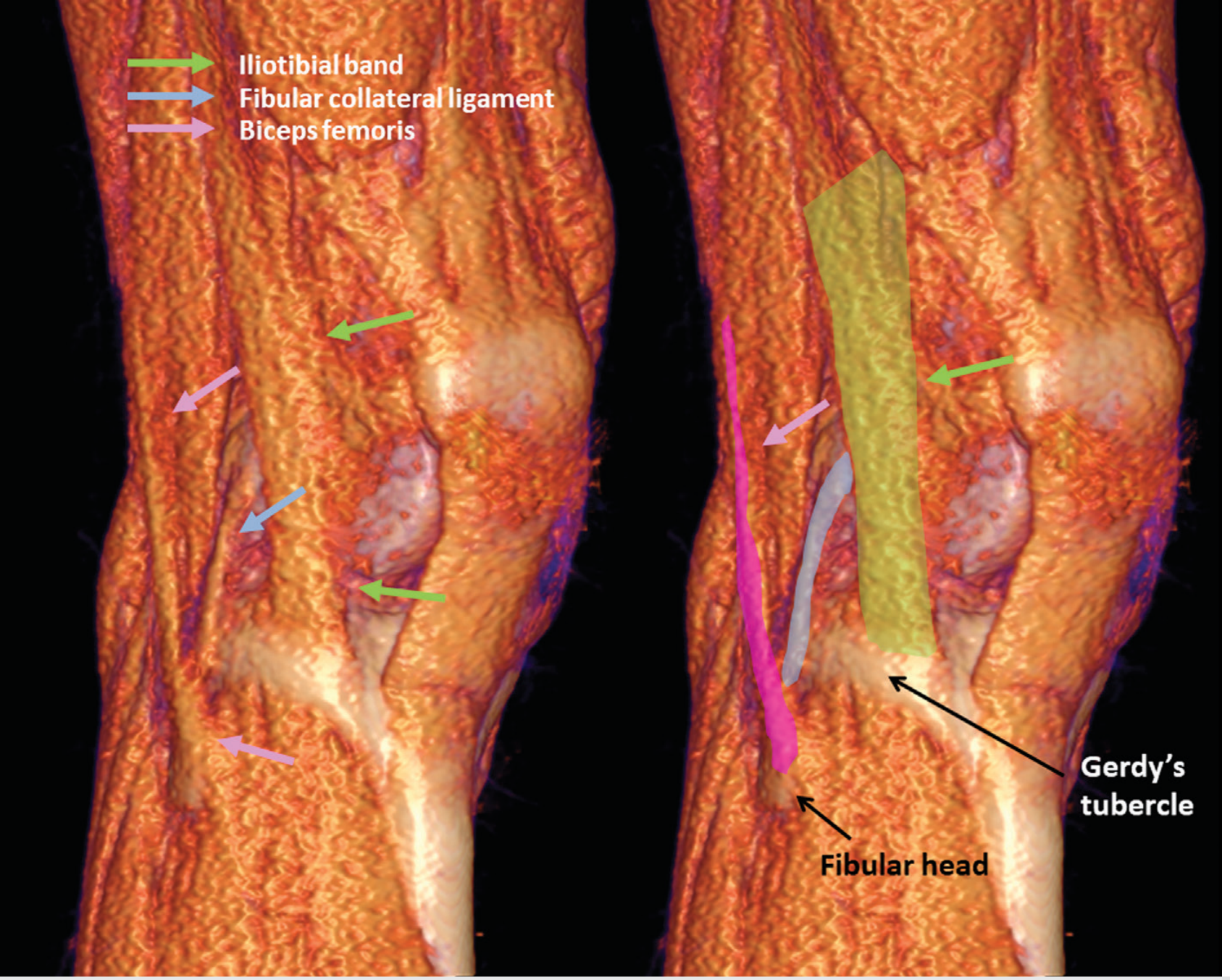
| Iliotibial band (ITB) | Runs from Gerdy's tubercle to the lateral femoral epicondyle; contributes to anterolateral stability | Constant |
| Biceps femoris tendon | Long and short heads converge and insert on the fibular head; reinforces the PLC laterally | Constant |
| Anterolateral ligament (ALL) | Origin: immediately anterior to popliteus tendon insertion on femur. Insertion: midway between Gerdy's tubercle and fibular head with firm attachments to lateral meniscus. Stabilises against internal tibial rotation | Constant |
| Fabellofibular ligament | Runs from the fabella (or lateral gastrocnemius tendon if fabella absent) to the fibular styloid; reinforces the posterolateral capsule | Variable (~20-35%) |
| Arcuate ligament | Y-shaped thickening of the posterolateral capsule; lateral limb to posterolateral capsule and oblique popliteal ligament, base to fibular styloid apex. Some recommend retiring this term as it is inconsistent | Variable; often absent |
| Lateral gastrocnemius tendon | Arises from the fabella/posterolateral femur; contributes to posterolateral capsule reinforcement | Constant |
| Mid-third lateral capsular ligament | Thickening of the mid-lateral capsule | Variable |
| Coronary ligament of lateral meniscus | Meniscotibial attachment; contributes to lateral meniscal stabilisation | Constant |
| Popliteomeniscal fascicles | Three fascicles (posteroinferior, posterosuperior, anteroinferior) from popliteus to posterior horn of lateral meniscus; form the popliteal hiatus | Posterosuperior + anteroinferior constant on MRI |
| Oblique popliteal ligament (Winslow's) | Extension of semimembranosus tendon; crosses the posterior capsule obliquely; reinforces the posterocentral capsule | Constant |
Layers of the Lateral Knee (Seebacher Classification)
| Layer | Contents |
|---|---|
| Layer I (superficial) | Iliotibial band anteriorly; biceps femoris and its expansion posteriorly |
| Layer II (middle) | Quadriceps retinaculum anteriorly; two patellofemoral ligaments |
| Layer III (deep / capsular) | Joint capsule; FCL (superficial lamina); popliteus tendon; fabellofibular + arcuate ligaments (deep lamina) |
Biomechanics and Functional Anatomy
| Motion Resisted | Primary Restraint | Secondary Restraint |
|---|---|---|
| External tibial rotation | Popliteus tendon + PFL | FCL, biceps femoris, ALL |
| Varus stress | FCL | Popliteus, IT band |
| Posterior tibial translation | PCL (primary) | PLC structures (secondary) |
| Internal tibial rotation | ACL (primary) | ALL, IT band |
| Genu recurvatum | PLC + PCL | Posterior capsule |
- The PLC provides its greatest contribution to posterolateral stability between 30° and 60° of knee flexion
- The FCL is tight in extension and lax in flexion, while the popliteus tendon shows increasing tension with internal tibial rotation at all degrees of flexion
- Isolated PLC injury rarely occurs; it is most commonly associated with PCL tears and/or ACL tears
- Brachial artery can be safely ligated: the common peroneal (fibular) nerve is the critical neural structure at risk in the PLC region, passing posterior to the biceps femoris tendon and around the neck of the fibula
Vascular Relations
Nerve at Risk
- PLC injuries (direct trauma / traction)
- Surgical approaches to the posterolateral knee
- Varus corrective osteotomies
Clinical Assessment Points
- Varus stress test: 0° and 30° flexion - isolates FCL (LCL) at 30°
- Dial test (external rotation): Asymmetric external rotation >10-15° at 30° only = isolated PLC; at 30° and 90° = combined PLC + PCL injury
- Posterolateral drawer test: External tibial rotation at 80-90° flexion
- Reverse pivot shift: Reduction of externally rotated/posterolaterally subluxed tibia during knee extension