What's cardiac temponad
Reading File
Finding Sources
Searching PubMed
"cardiac tamponade"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I have everything needed for a complete, well-sourced answer.
Cardiac Tamponade
Definition
Cardiac tamponade is a life-threatening condition in which fluid accumulates in the pericardial space and the resulting rise in intrapericardial pressure compresses the heart, impairs chamber filling, and ultimately reduces cardiac output. It is a medical emergency requiring urgent drainage.
Pathophysiology
Under normal conditions, the pericardium accommodates only a small amount of fluid. Once that limit is reached, a steep pressure-volume relationship means even small additional fluid volumes cause a rapid rise in pericardial pressure.
The rate of accumulation matters enormously:
- A rapidly developing effusion (e.g., trauma, aortic dissection, cardiac perforation) can cause tamponade with as little as 100-200 mL of blood.
- A slowly developing effusion gradually stretches the pericardium, shifting that curve to the right - which is why large chronic effusions (sometimes >1 L) may cause no tamponade at all.
When intrapericardial pressure exceeds cardiac chamber pressures, chamber compression occurs. This forces the chambers to compete for the fixed volume within the pericardial sac - a phenomenon called ventricular interdependence. With each inspiration, right ventricular filling is enhanced, the interventricular septum shifts leftward, and left ventricular filling (and stroke volume) drops. This is reversed on expiration. In tamponade, this normal respiratory variation becomes exaggerated, producing pulsus paradoxus.
- Goldman-Cecil Medicine, p. 716-717
- Miller's Anesthesia, 10e, p. 5025-5026
Causes
Common causes of pericardial effusion that can progress to tamponade:
| Cause | Approximate % |
|---|---|
| Idiopathic / viral | 37% |
| Neoplastic (malignant) | 19% |
| Iatrogenic / trauma | 13% |
| Tuberculous / purulent | 6% |
| Acute MI | 6% |
| Collagen vascular disease (e.g., lupus) | 4% |
| Uremia | 4% |
| Radiation-induced | 2% |
| Aortic dissection | 2% |
Drugs that can cause pericardial effusion include hydralazine, procainamide, phenytoin, isoniazid, and cromolyn.
- Goldman-Cecil Medicine, p. 716
Clinical Features
Patients with tamponade are typically anxious, tachycardic, and may complain of dyspnea, orthopnea, and chest discomfort.
Beck's Triad (the classic trio, though seen in fewer than half of cases):
- Hypotension - reduced cardiac output
- Elevated jugular venous pressure (JVD / distended neck veins)
- Muffled heart sounds
Other findings:
- Pulsus paradoxus - an inspiratory fall in systolic BP of >10 mmHg. This is the most sensitive sign: sensitivity ~98%, specificity ~83%, LR+ 5.9, LR- 0.03.
- Tachycardia - 100% sensitive for tamponade (though not specific)
- JVD - 100% sensitive
- The jugular venous waveform typically shows a prominent x descent with absent y descent
- Kussmaul sign (JVP paradoxically rising with inspiration) is more typical of constrictive pericarditis but can be seen
Important caveat: In hemorrhagic tamponade or hypovolemia, JVD may be absent ("low-pressure tamponade"), and hypotension may dominate the picture. Positive pressure ventilation worsens hemodynamics by further increasing intrathoracic pressure.
- Symptom to Diagnosis, 4th ed., p. 5199-5204
- Goldman-Cecil Medicine, p. 717
Diagnosis
Tamponade is ultimately a clinical diagnosis, supported by imaging.
ECG
- Electrical alternans - beat-to-beat alternation in QRS axis/amplitude due to the heart swinging within the fluid-filled sac. Low voltage may also be seen.
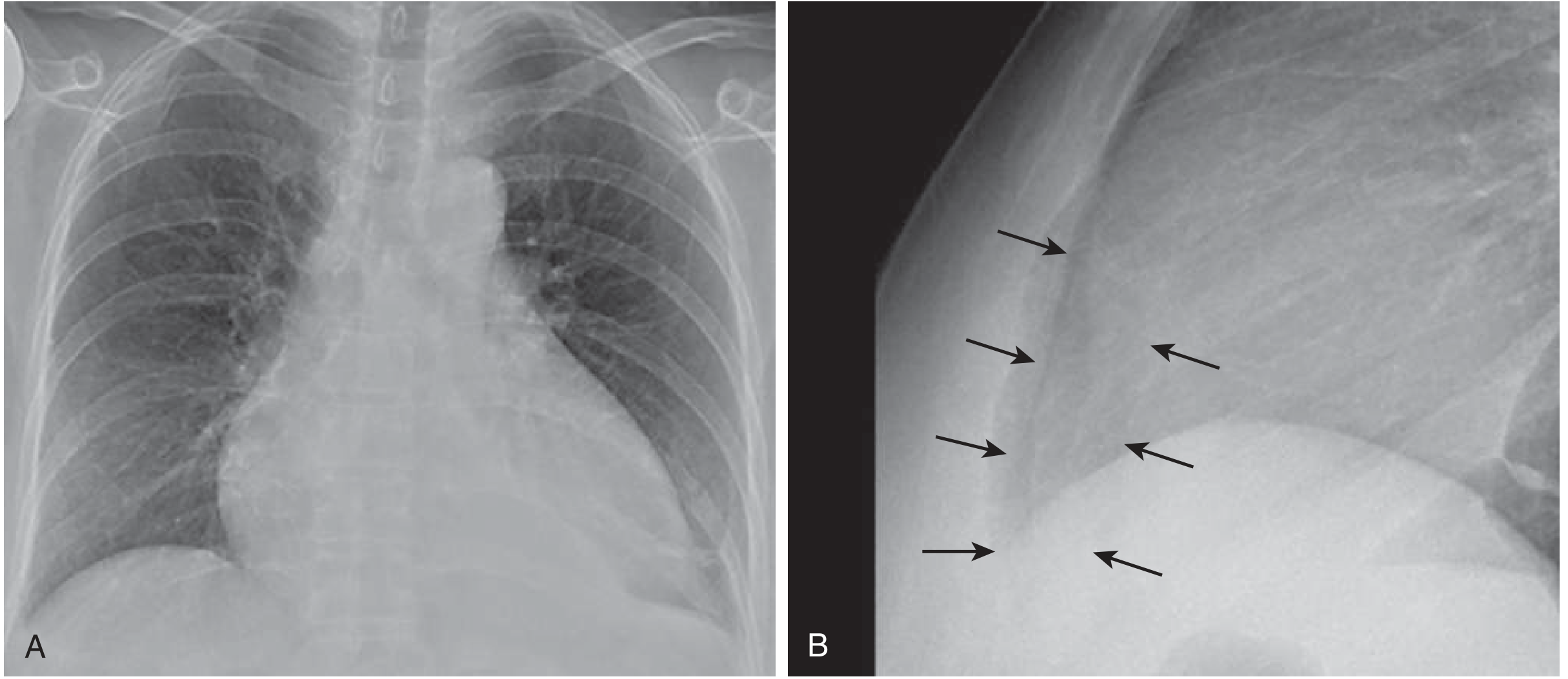
Chest X-Ray
- Enlarged cardiac silhouette with a "water bottle" configuration (globular shape)
- On lateral view: separation of the pericardial and epicardial fat stripes
Echocardiography (gold standard)
- Pericardial fluid appears as an echolucent space around the heart
- Right atrial collapse during ventricular systole - most sensitive (50-100%) but least specific (33-100%)
- RV diastolic collapse - appears later, more specific (75-90%) but lower sensitivity (48-60%)
- Absence of any right-sided collapse has high negative predictive value for clinical tamponade
- Respiratory variation in Doppler flows - >25% variation in mitral inflow, >40% in tricuspid inflow
Note: In pulmonary hypertension, right-sided collapse may be absent even with tamponade physiology (elevated baseline RV pressures prevent it from being compressed).
- Miller's Anesthesia, 10e, p. 5026-5027
Treatment
Treatment is urgent drainage of the pericardial effusion. There is no effective medical substitute.
Temporizing measures:
- IV fluid bolus may transiently help in hypovolemic tamponade by increasing venous pressure
- Inotropes are generally ineffective (endogenous adrenergic drive is already maximal)
- Avoid initiating mechanical ventilation if possible - positive intrathoracic pressure further impairs filling and can precipitate cardiovascular collapse
Definitive treatment:
-
Echocardiography-guided pericardiocentesis (first-line for most patients)
- Indicated when ≥1 cm of fluid is seen anterior to the mid-RV free wall throughout diastole
- A needle enters the pericardial space (usually from the subxiphoid/apical approach), and a catheter is left in for continued drainage to reduce recurrence risk
- Fluid is sent for LDH, protein, cell count, cytology, TB PCR, and cultures
-
Surgical drainage (pericardial window or pericardiectomy)
- Preferred when tissue is needed for diagnosis, effusion is <1 cm, organized/multiloculated, or recurrent
- Malignant effusions frequently recur and often require a surgical window into the pleural space
-
Emergency thoracotomy
- For pulseless patients with penetrating cardiac trauma
Prognosis: In-hospital mortality with appropriate drainage is <10%, but subsequent mortality is ~75% for malignant effusions vs. 3-5% annually for other causes.
- Goldman-Cecil Medicine, p. 718
- Roberts & Hedges' Clinical Procedures in Emergency Medicine, p. 522
Summary Table
| Feature | Detail |
|---|---|
| Core mechanism | Intrapericardial pressure exceeds chamber filling pressure |
| Key triad | Hypotension + JVD + muffled heart sounds (Beck's triad) |
| Most sensitive sign | Pulsus paradoxus (>10 mmHg inspiratory BP drop) |
| ECG finding | Electrical alternans, low voltage |
| CXR finding | "Water bottle" heart |
| Echo finding | Chamber collapse (RA first, then RV) |
| Treatment | Pericardiocentesis (emergent drainage) |
This is a shared conversation. Sign in to Orris to start your own chat.