Citizen
Hello! How can I help you today?
Explain me
It looks like your message got cut off! Could you finish your thought?
For example:
- "Explain me [topic]"
- "Explain me how [something] works"
What would you like me to explain?
Heart attack
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Here is a thorough explanation of a heart attack, drawing from leading medical textbooks (Robbins & Kumar Basic Pathology, Guyton & Hall Textbook of Medical Physiology, and Medical Physiology):
Heart Attack (Myocardial Infarction)
What Is It?
A myocardial infarction (MI) - commonly called a "heart attack" - is the death (necrosis) of heart muscle tissue caused by a lack of blood supply (ischemia). The 2018 joint definition from U.S. and European Cardiology groups describes it as "the presence of acute myocardial injury detected by abnormal cardiac biomarkers in the setting of evidence of acute myocardial ischemia."
- Robbins & Kumar Basic Pathology, p. 353
Who Gets It?
- Risk rises with age, but ~10% of MIs occur before age 40; 45% occur before age 65
- Men are at higher risk, but the gap narrows with age
- Women are somewhat protected during reproductive years due to estrogen, but after menopause, risk rises sharply
- Key risk factors: atherosclerosis, high blood pressure, diabetes, smoking, high cholesterol, obesity
What Causes It? (Pathogenesis)
The vast majority of heart attacks follow this sequence:
- Plaque disruption - A fatty (atheromatous) plaque inside a coronary artery gets eroded or suddenly ruptures, exposing its contents to the bloodstream
- Platelet activation - Platelets rush to the site, stick together, and release chemicals (thromboxane A2, ADP, serotonin) that trigger more clotting and blood vessel spasm
- Clot formation - The coagulation cascade activates, and a growing blood clot (thrombus) forms rapidly
- Complete blockage - Within minutes, the thrombus can fully block the artery
In about 10% of cases, there is no atheromatous plaque - instead, coronary artery spasm, blood clots from the heart (e.g., atrial fibrillation), or small vessel disease is responsible.
What Happens to the Heart Muscle?
Once blood flow stops:
- Within seconds: aerobic metabolism stops; ATP drops; lactic acid accumulates
- Within minutes: the heart muscle loses its ability to contract
- 20-40 minutes: if blood flow is not restored, irreversible cell death begins
- Hours later: the infarcted area turns bluish-brown, blood vessels become engorged with stagnant deoxygenated blood, cells swell, and muscle fibers die
The innermost layer of the heart (subendocardium) is most vulnerable because it is the last to receive blood and faces the highest internal pressure.
The diagram below shows what happens when part of the heart muscle becomes nonfunctional - healthy areas still contract, but the dead or damaged region is passively stretched outward ("systolic stretch"), dramatically reducing the heart's pumping efficiency:
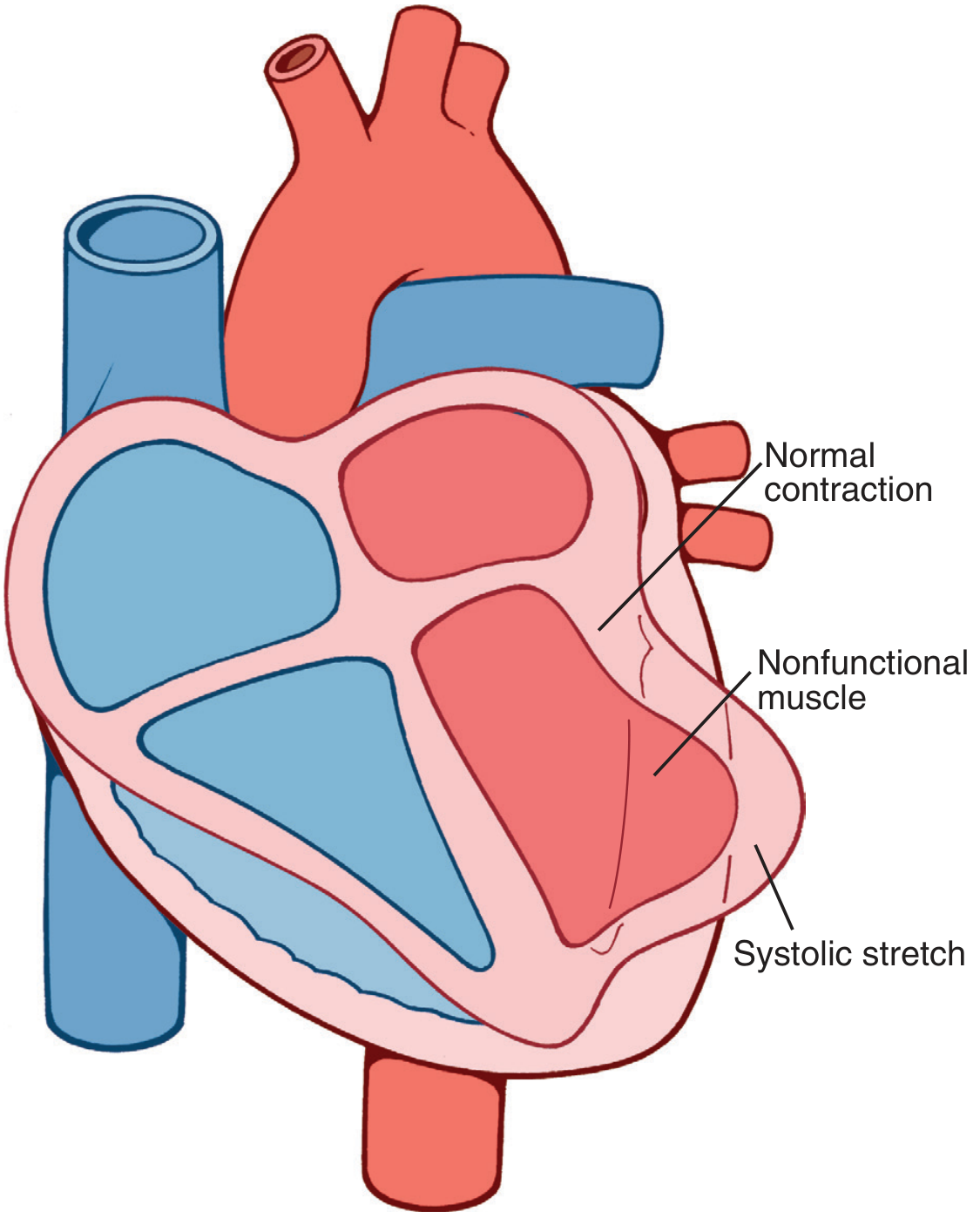
Systolic stretch: normal muscle contracts while the infarcted zone bulges outward - Guyton & Hall, p. 271
Symptoms
| Symptom | Details |
|---|---|
| Chest pain/pressure | Often described as crushing, squeezing, or heaviness |
| Radiating pain | Can spread to the left arm, jaw, neck, or back |
| Shortness of breath | Due to reduced cardiac output or pulmonary congestion |
| Sweating, nausea | Common accompanying symptoms |
| Silent MI | Some patients (especially diabetics and women) have minimal or no pain |
ECG Changes
The ECG changes in a heart attack follow a predictable pattern:
- T-wave peaking, then inversion - earliest change; reversible
- ST-segment elevation - hallmark of acute MI; indicates ongoing injury
- Deep Q waves - develop after irreversible cell death; indicate electrically silent ("dead") tissue
The specific leads showing these changes tell the doctor which part of the heart is affected (e.g., inferior, anterior, or lateral wall).
Consequences / Causes of Death
- Decreased cardiac output - the damaged heart pumps less blood; can lead to cardiogenic shock
- Pulmonary edema - blood backs up into the lungs, causing fluid accumulation
- Ventricular fibrillation - the most common cause of sudden cardiac death after MI (80-90% of cardiac deaths); arises from electrical instability in the ischemic muscle
- Heart rupture - rare but catastrophic complication
Treatment Principles
The key goal is to restore blood flow as quickly as possible before irreversible damage spreads:
- Thrombolysis (clot-busting drugs) - dissolve the clot
- Angioplasty / PCI (Percutaneous Coronary Intervention) - physically open the blocked artery with a balloon and stent
- Aspirin + antiplatelet drugs - prevent further clot growth
- Beta-blockers - reduce heart oxygen demand and protect against a second MI
Early reperfusion within 90 minutes of symptom onset can save large amounts of heart muscle. Even if done quickly, the reperfused heart may remain "stunned" (temporarily non-contractile) for several days before recovering.
Bottom line: A heart attack is a medical emergency caused by a sudden blockage of a coronary artery, most often by a blood clot on a ruptured plaque. Without rapid treatment, heart muscle dies permanently. Time is muscle.
Medication
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
I now have comprehensive information from the textbooks. Here is a full breakdown of heart attack medications:
Medications for Heart Attack (Myocardial Infarction)
Medications are divided into two phases: acute (emergency) treatment and long-term (secondary prevention) therapy.
Phase 1 - Acute / Emergency Medications
These are given immediately when a heart attack is happening:
1. Aspirin (162-325 mg, chewable)
- First drug given to anyone suspected of having a heart attack
- Blocks platelet aggregation by inhibiting thromboxane A2
- Prevents the blood clot from growing larger
- Chewed (not swallowed whole) for faster absorption
2. P2Y12 / ADP Receptor Antagonists (Dual Antiplatelet Therapy)
Given alongside aspirin to further block platelet clumping:
| Drug | Loading Dose | Notes |
|---|---|---|
| Clopidogrel | 600 mg oral | Older agent, widely used |
| Prasugrel | 60 mg oral | More potent; avoid in prior stroke/TIA |
| Ticagrelor | 180 mg oral | Fast-acting; preferred in many guidelines |
- Continued for 12 months after a heart attack, regardless of whether a stent was placed
3. Anticoagulants
Prevent further clot formation:
- Unfractionated Heparin (UFH) - standard option, often combined with GP IIb/IIIa inhibitors
- Bivalirudin - direct thrombin inhibitor; alternative to heparin, lower bleeding risk
- Low-molecular-weight heparin (LMWH) - enoxaparin is a common alternative
4. Beta-Blockers (oral, within 24 hours)
- Reduce heart rate and blood pressure, decreasing the oxygen demand of the heart
- Limit the size of the infarct
- IV beta-blockers reserved for patients with severe hypertension or ongoing ischemia
- Examples: metoprolol, carvedilol, atenolol
5. Nitrates (IV or sublingual)
- Cause vasodilation - widen blood vessels to improve blood flow and relieve chest pain
- Nitroglycerin is the standard agent
- Avoid in patients with low blood pressure or those who have taken phosphodiesterase inhibitors (e.g., sildenafil/Viagra) within 24-48 hours
6. Morphine (for pain)
- Opioid analgesic used for severe chest pain not relieved by nitrates
- Also reduces anxiety, which decreases sympathetic activation and cardiac workload
- Use with caution - can reduce absorption of oral antiplatelet drugs
7. Supplemental Oxygen
- Given if oxygen saturation is low (<90%)
- Helps maintain adequate oxygen delivery to the ischemic heart muscle
Phase 2 - Long-Term / Secondary Prevention Medications
These are continued after the acute event to prevent a second heart attack:
1. Aspirin (low-dose, lifelong)
- 81-100 mg daily, continued indefinitely
- Reduces risk of recurrent MI, stroke, and cardiovascular death
2. Beta-Blockers (long-term)
- Proven to reduce mortality after MI
- Protect against sudden cardiac death from arrhythmias
- Especially important in patients with reduced heart function (EF <40%)
- Examples: metoprolol succinate, carvedilol, bisoprolol
3. ACE Inhibitors (or ARBs)
- Reduce the workload on the heart by lowering blood pressure and reducing fluid retention
- Most important in patients with:
- Reduced ejection fraction (EF <40%)
- Heart failure after MI
- Anterior wall MI
- Diabetes or hypertension
- Examples: lisinopril, ramipril, enalapril
- If the patient cannot tolerate ACE inhibitors (due to cough), switch to an ARB (e.g., valsartan, losartan)
4. Statins (high-intensity, lifelong)
- Reduce LDL cholesterol and stabilize remaining plaques to prevent future rupture
- High-intensity statin recommended for all MI patients regardless of baseline cholesterol
- Examples: atorvastatin 40-80 mg, rosuvastatin 20-40 mg
5. Aldosterone Antagonists
- Added in patients who are already on a beta-blocker + ACE inhibitor AND have:
- EF <40%
- Symptomatic heart failure OR diabetes
- Examples: eplerenone, spironolactone
- Reduce fluid overload and risk of sudden cardiac death
Summary Table
| Phase | Drug Class | Example | Goal |
|---|---|---|---|
| Acute | Aspirin | Aspirin 162-325 mg | Stop clot growth |
| Acute | P2Y12 inhibitor | Ticagrelor, clopidogrel | Block platelet activation |
| Acute | Anticoagulant | Heparin, bivalirudin | Prevent clot extension |
| Acute | Beta-blocker | Metoprolol IV/oral | Reduce O2 demand |
| Acute | Nitrate | Nitroglycerin | Relieve pain, vasodilate |
| Acute | Opioid | Morphine | Pain control |
| Long-term | Aspirin (low dose) | Aspirin 81 mg | Prevent recurrence |
| Long-term | Beta-blocker | Carvedilol | Reduce mortality |
| Long-term | ACE inhibitor/ARB | Lisinopril, valsartan | Heart protection |
| Long-term | Statin | Atorvastatin 80 mg | Cholesterol + plaque |
| Long-term | Aldosterone antagonist | Eplerenone | Heart failure prevention |
Key principle: The faster the artery is reopened (by PCI or thrombolysis) and the sooner medications are started, the more heart muscle is saved and the better the long-term outcome.
- Textbook of Family Medicine 9e, p. 681
- Braunwald's Heart Disease, Textbook of Cardiovascular Medicine
Pregnancy
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Here is a detailed explanation of heart attack in pregnancy, drawing from Braunwald's Heart Disease, Creasy & Resnik's Maternal-Fetal Medicine, and Fuster & Hurst's The Heart:
Heart Attack During Pregnancy
How Common Is It?
Acute MI complicates approximately 1 in 16,000 pregnancies - rare, but life-threatening. The incidence is 3 times higher than in age-matched non-pregnant women of the same age, due to the cardiovascular stress pregnancy places on the body.
- Highest risk: third trimester and in women over 30 (older multigravidas)
- Creasy & Resnik's Maternal-Fetal Medicine
Why Does It Happen in Pregnancy? (Causes)
The causes differ from typical heart attacks in the general population:
| Cause | % of Cases |
|---|---|
| SCAD (Spontaneous Coronary Artery Dissection) | 43% |
| Atherosclerosis (plaque rupture) | 27% |
| Blood clot without atherosclerosis | 17% |
| Normal coronary anatomy (vasospasm) | 9% |
| Coronary spasm | 2% |
| Takotsubo (stress) cardiomyopathy | 2% |
SCAD (a tear in the coronary artery wall) is the most common cause - very different from non-pregnant adults where atherosclerotic plaque rupture dominates. Pregnancy hormones weaken the arterial wall structure, making it prone to spontaneous tearing, often affecting the left anterior descending (LAD) artery.
Additional risk factors in pregnancy: hypertension, diabetes, obesity, hyperlipidemia, and preeclampsia (which is over-represented in pregnancy-associated MI).
How Pregnancy Changes the Heart
Pregnancy creates significant cardiovascular stress:
- Blood volume increases by ~50%
- Heart rate increases
- Cardiac output rises by 30-50%
- Blood is in a more pro-thrombotic (clotting) state
- Hormonal changes weaken arterial walls
All of this raises the risk of both coronary artery dissection and clot formation.
Treatment - What Is Safe and What Is Not?
Management must protect both mother and fetus. Many standard heart attack drugs have fetal risks.
Acute Treatment (Emergency)
| Treatment | Safe in Pregnancy? | Notes |
|---|---|---|
| Aspirin | Yes | Given as standard antiplatelet therapy |
| IV Anticoagulants (Heparin/LMWH) | Yes | Heparin and LMWH do NOT cross the placenta - preferred |
| Primary PCI (angioplasty/stenting) | Yes (preferred) | Treatment of choice for STEMI; fetus shielded with lead |
| Thrombolytics (e.g., tPA, streptokinase) | Relatively contraindicated | High risk of maternal bleeding; used only if PCI unavailable |
| P2Y12 inhibitors (clopidogrel, ticagrelor) | Caution | Limited data; used when benefit outweighs risk |
| Nitrates | Caution | Can be used for pain/ischemia with monitoring |
| Beta-blockers (metoprolol, labetalol) | Generally safe | May cause fetal bradycardia or reduced birth weight (IUGR) - use lowest effective dose |
| Morphine | Caution | Can be used short-term; crosses placenta |
Long-Term Medications - Safety in Pregnancy
| Drug | Pregnancy Safety | Reason |
|---|---|---|
| Statins | Contraindicated | Teratogenic - may harm fetal development; must be stopped |
| ACE Inhibitors / ARBs | Contraindicated in 2nd & 3rd trimester | Cause fetal kidney damage, oligohydramnios, limb defects, death |
| Warfarin | Teratogenic (1st trimester) | Causes warfarin embryopathy; switch to LMWH heparin |
| LMWH (e.g., enoxaparin) | Safe | Does not cross placenta; preferred anticoagulant throughout pregnancy |
| Beta-blockers | Relatively safe | Labetalol/metoprolol used; watch for IUGR, neonatal bradycardia |
| Calcium channel blockers (nifedipine) | Relatively safe | Used for blood pressure control |
| Aspirin (low dose) | Safe | Also used to prevent preeclampsia |
Special Consideration: SCAD (Spontaneous Coronary Artery Dissection)
Since SCAD - not plaque rupture - is the dominant cause of MI in pregnancy:
- Conservative management is preferred for stable NSTEMI with SCAD
- Coronary angiography carries extra risk of catheter-induced dissection in pregnancy
- For stable patients without ongoing angina: medical management without invasive procedures is recommended
- A CT coronary angiogram with lead shielding can be considered if angina persists
Labor and Delivery After a Heart Attack
- Women should ideally wait 1 year after an MI before becoming pregnant
- During labor: ECG monitoring is standard
- If large MI occurred during pregnancy: invasive hemodynamic monitoring is required (arterial line, central venous pressure, pulmonary artery pressures)
- Watch for sudden preload surge at delivery (when the uterus contracts and returns blood to circulation) and blood loss after placental delivery
Maternal Mortality
With modern care, maternal mortality from pregnancy-associated MI is approximately 5-7% - lower than historical figures but still significantly elevated compared to MI in non-pregnant women.
- Creasy & Resnik's Maternal-Fetal Medicine, p. 1529-1534
- Braunwald's Heart Disease, Textbook of Cardiovascular Medicine
- Fuster & Hurst's The Heart, 15th Edition - Table 27-2
Key takeaway: Heart attack in pregnancy is dominated by SCAD rather than atherosclerosis. Treatment priorities are emergency PCI for STEMI, heparin/LMWH as safe anticoagulants, and avoidance of statins, ACE inhibitors, and warfarin to protect the fetus.
This is a shared conversation. Sign in to Orris to start your own chat.