Explain me to 10 common heart disease with ECG changes and ECG images of those diseases
Reading File
Finding Sources
Searching the Web
common heart diseases ECG changes electrocardiogram findings with images
Finding Sources
Finding Sources
Searching the Web
STEMI ECG atrial fibrillation heart block LVH ECG images site:litfl.com OR site:ecgwaves.com
Reading File
Reading Web Page
https://litfl.com/atrial-fibrillation-ecg-library
Searching the Web
10 common heart diseases ECG findings STEMI Afib heart failure pericarditis hypertrophy ECG images litfl
Reading File
Reading Web Page
https://mesimedical.com/insights/frequently-diagnosed-condit…
Loading Image
Loading Image
Finding Sources
Finding Sources
Loading Image
Finding Sources
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
Searching the Web
ECG pericarditis diffuse ST elevation PR depression site:litfl.com OR site:ecgwaves.com
Loading Image
Loading Image
Searching the Web
Wolff-Parkinson-White syndrome ECG delta wave image pulmonary embolism S1Q3T3 ECG image site:litfl.com
I now have comprehensive information from Harrison's Principles of Internal Medicine, Goldman-Cecil Medicine, Braunwald's Heart Disease, and multiple authoritative ECG sources. Let me compile the full detailed response:
10 Common Heart Diseases: ECG Changes & Images
Background: How to Read ECG Changes
The ECG records the heart's electrical activity as waves (P, QRS, T) across 12 leads. Disease states alter these waves in characteristic patterns. The diagram below from Harrison's illustrates the core mechanism - subendocardial ischemia pushes the ST vector inward (causing ST depression), while transmural ischemia pushes it outward (causing ST elevation):

1. ST-Elevation Myocardial Infarction (STEMI)
What it is: Complete occlusion of a coronary artery causing transmural (full-thickness) myocardial necrosis.
ECG Changes:
- Hyperacute T waves - earliest sign, tall peaked T waves
- ST elevation - ≥1 mm in 2 contiguous limb leads, or ≥2 mm in 2 contiguous precordial leads (convex/tombstone shape)
- Pathological Q waves - develop within hours to days (>40 ms wide or >25% of QRS height), indicating necrosis
- T wave inversion - follows the ST elevation as infarction evolves
- Reciprocal ST depression in opposite leads
Lead Localisation:
| Territory | Artery | ECG Leads |
|---|---|---|
| Anterior | LAD | V1-V4, I, aVL |
| Inferior | RCA/LCx | II, III, aVF |
| Lateral | LCx | I, aVL, V5-V6 |
| Posterior | RCA | Reciprocal changes V1-V3 (tall R, ST depression) |
ECG - Anterior STEMI evolution (Acute → Evolving):
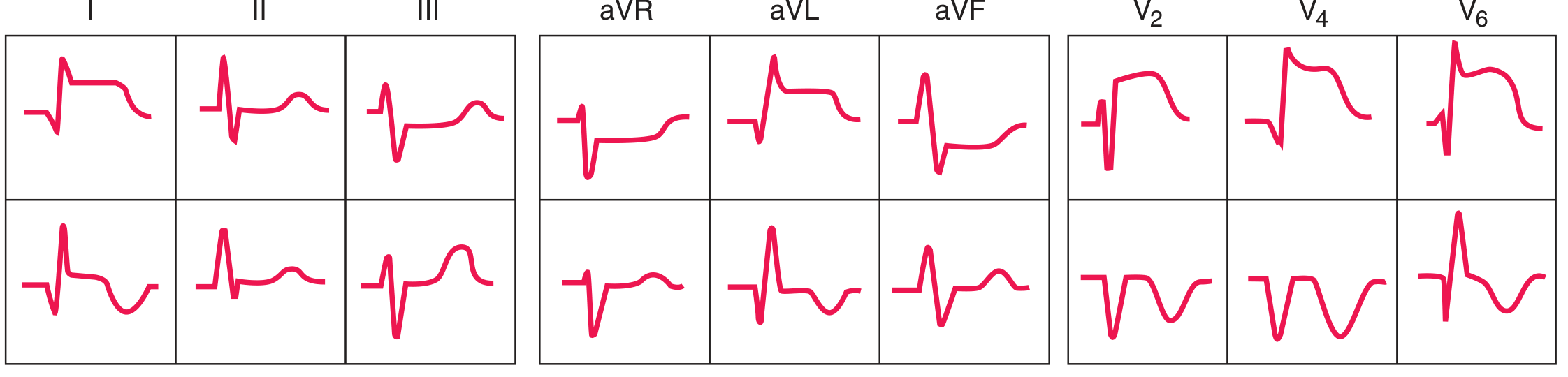 Harrison's Principles of Internal Medicine 22E - Anterior ST-elevation/Q-wave infarction sequence
Harrison's Principles of Internal Medicine 22E - Anterior ST-elevation/Q-wave infarction sequence
ECG - Inferior STEMI evolution:
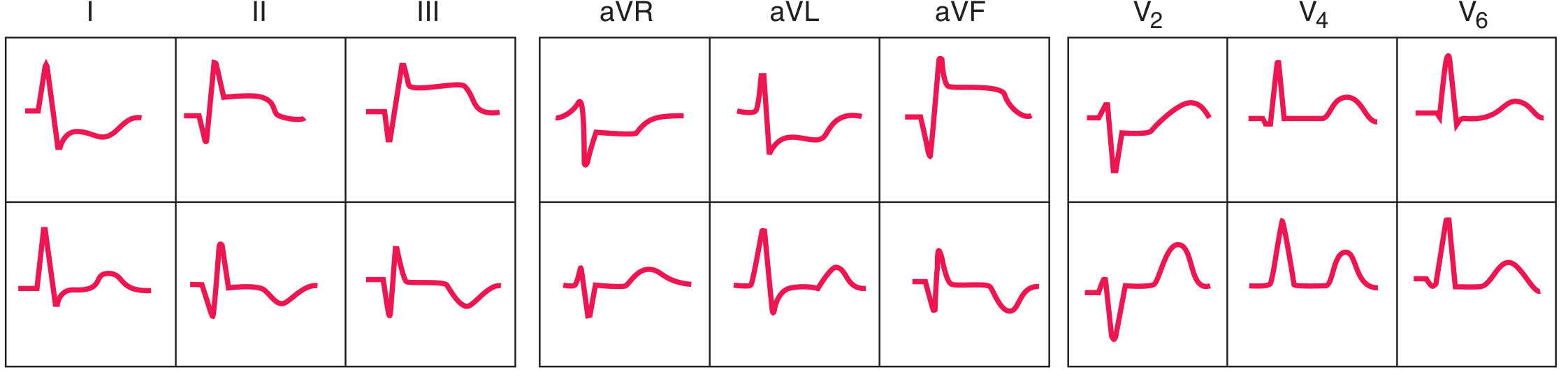 Harrison's Principles of Internal Medicine 22E - Inferior ST-elevation/Q-wave infarction sequence
Harrison's Principles of Internal Medicine 22E - Inferior ST-elevation/Q-wave infarction sequence
2. Non-ST-Elevation Myocardial Infarction (NSTEMI) / Unstable Angina
What it is: Partial coronary occlusion or severe narrowing - subendocardial ischemia without full-thickness necrosis.
ECG Changes:
- ST depression (horizontal or downsloping, ≥0.5 mm) - the hallmark
- T wave inversion - often widespread or in distribution of ischemic vessel
- Wellens T-waves - deep symmetrical T inversions in V1-V4 (sign of critical LAD stenosis)
- No ST elevation (by definition)
- ECG may be normal in up to 30% - diagnosis requires troponin elevation
Wellens Syndrome ECG (LAD critical stenosis):
 Harrison's Principles of Internal Medicine 22E - Deep T-wave inversions (Wellens sign) indicating critical LAD stenosis
Harrison's Principles of Internal Medicine 22E - Deep T-wave inversions (Wellens sign) indicating critical LAD stenosis
- Source: Harrison's Principles of Internal Medicine 22E (2025)
3. Atrial Fibrillation (AF)
What it is: Disorganised rapid atrial electrical activity (400-600 impulses/min) with chaotic, irregular ventricular response. Most common sustained arrhythmia.
ECG Changes:
- Absent P waves - replaced by irregular fibrillatory (f) waves of varying morphology
- Irregularly irregular RR intervals - the hallmark
- Narrow QRS complexes (unless aberrant conduction or bundle branch block)
- Atrial rate 400-600 bpm; ventricular rate typically 100-180 bpm (uncontrolled)
- Fibrillatory baseline - fine or coarse oscillations replacing the isoelectric line
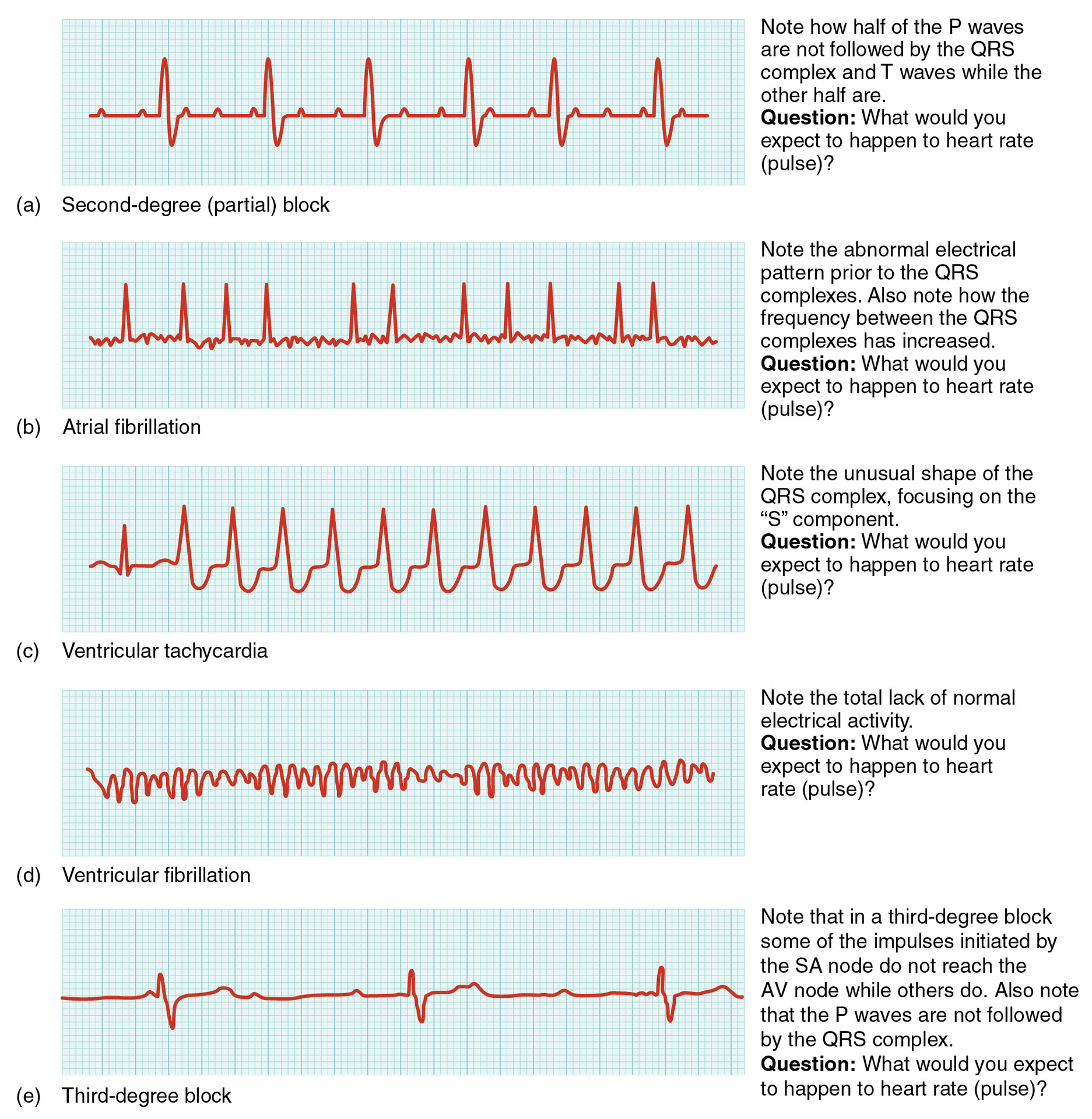
ECG - Atrial fibrillation patterns:
4. Complete (Third-Degree) AV Heart Block
What it is: Complete failure of impulse conduction from atria to ventricles. Atria and ventricles beat independently. Can be caused by acute MI (inferior > anterior), myocarditis, infiltrative cardiomyopathy, or drug toxicity.
ECG Changes:
- P waves and QRS complexes are completely dissociated - atria and ventricles beat independently
- Atrial rate > ventricular rate (e.g., atria at 80 bpm, ventricles at 30-40 bpm)
- Regular P waves at one rate (P-P interval constant)
- Regular but slow QRS at a different (escape) rate
- Wide QRS if ventricular escape rhythm; narrow QRS if junctional escape
- No PR relationship
ECG - Third-degree (Complete) Heart Block shown in panel (e) above:
The image clearly shows P waves occurring at regular intervals that bear no relationship to the QRS complexes.
- Braunwald's Heart Disease: "Complete AV dissociation with an atrial rate faster than the ventricular rate" - Goldman-Cecil Medicine
Second-degree (Mobitz II) block is shown in panel (a) above - note how every other P wave fails to generate a QRS.
5. Acute Pericarditis
What it is: Inflammation of the pericardial sac - commonly viral, autoimmune, or post-MI. The inflamed pericardium causes current-of-injury pattern affecting all chambers.
ECG Changes (4 Stages):
- Stage 1 (hours-days): Diffuse concave ("saddle-shaped") ST elevation in nearly all leads EXCEPT aVR and V1; PR segment depression (most marked in II, aVF, V4-V6); PR elevation in aVR (reciprocal)
- Stage 2 (days): ST normalises, T waves flatten
- Stage 3 (1-3 weeks): Diffuse T wave inversion throughout ECG
- Stage 4: ECG normalisation
Key distinguishing features from STEMI:
- ST elevation is diffuse (not in a single coronary territory)
- ST morphology is concave (not convex)
- PR depression is present (specific for pericarditis)
- No reciprocal ST depression (unlike STEMI)
- No Q waves
ECG - Acute Pericarditis (Stage 1):
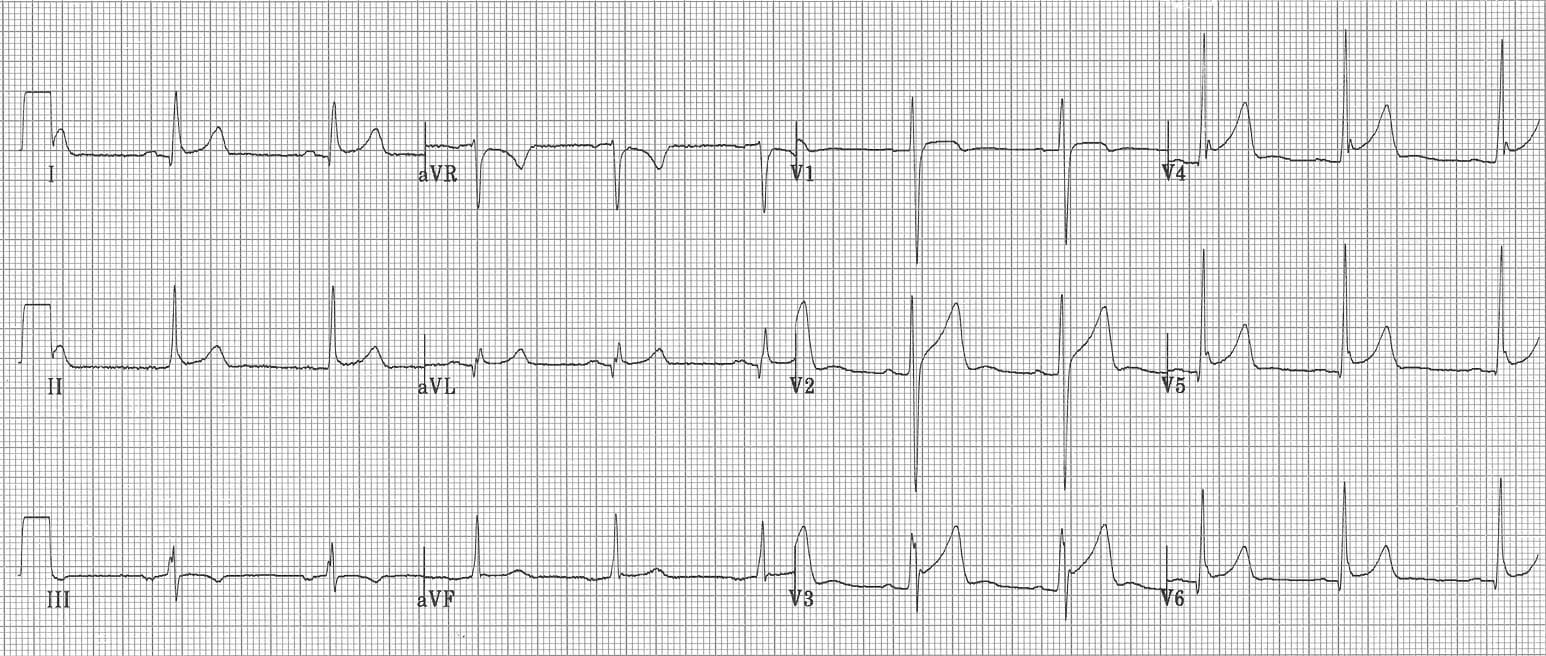 Classic pericarditis pattern: diffuse concave ST elevation, PR depression - LITFL ECG Library
Classic pericarditis pattern: diffuse concave ST elevation, PR depression - LITFL ECG Library
ECG - Acute Pericarditis (12-lead case):
 JETem: Stage 1 acute pericarditis - diffuse ST elevation with PR depression in inferior and lateral leads
JETem: Stage 1 acute pericarditis - diffuse ST elevation with PR depression in inferior and lateral leads
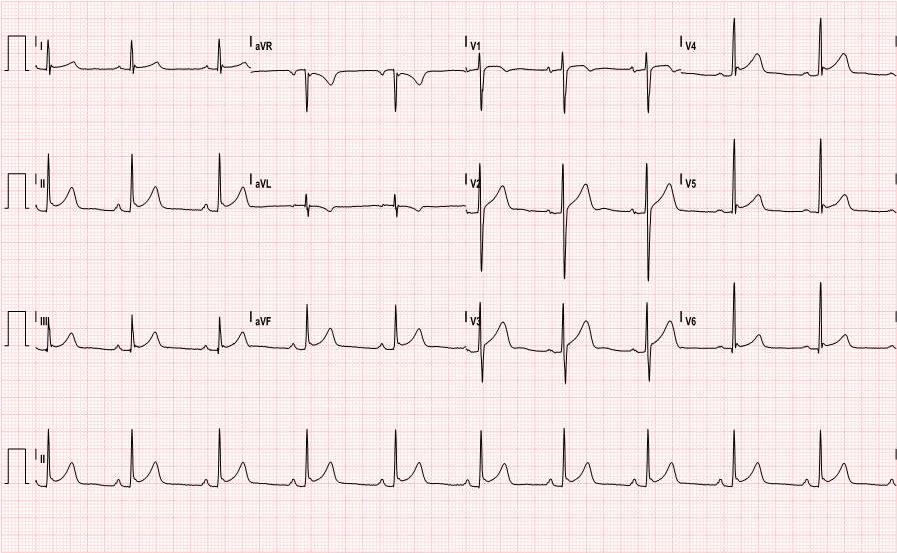
6. Left Ventricular Hypertrophy (LVH)
What it is: Thickening of the left ventricular wall due to chronic pressure overload (hypertension, aortic stenosis) or volume overload. More muscle = greater electrical voltage.
ECG Changes:
- Voltage criteria (Sokolow-Lyon): S in V1 + R in V5 or V6 ≥ 35 mm
- Cornell criteria: R in aVL + S in V3 > 28 mm (men) or >20 mm (women)
- Left axis deviation
- Repolarisation abnormalities (LV strain pattern): ST depression and asymmetric T-wave inversion in lateral leads (I, aVL, V5-V6) - the "strain" pattern
- Prolonged QRS (but <120 ms)
- Tall R waves in V5-V6; deep S waves in V1-V2
- Left atrial enlargement often coexists: broad notched P waves (P mitrale) in II, negative terminal P deflection in V1
ECG - LVH with strain pattern:
 (Image may not render - available at ECGWaves LVH guide)
(Image may not render - available at ECGWaves LVH guide)
7. Ventricular Tachycardia (VT)
What it is: A rapid life-threatening arrhythmia originating from ventricular muscle or His-Purkinje system (≥3 consecutive ventricular beats at ≥100 bpm). Common in ischemic heart disease, cardiomyopathy.
ECG Changes:
- Wide QRS complexes (≥120 ms, usually ≥140 ms) - broad, bizarre morphology
- Rate typically 100-250 bpm
- AV dissociation - P waves (when visible) have no relationship to QRS (independent atrial activity)
- Capture beats - occasional narrow QRS when sinus impulse captures ventricles (pathognomonic of VT)
- Fusion beats - hybrid beat when sinus and VT impulses merge
- Concordance - all precordial leads (V1-V6) show QRS deflections in same direction
- North West axis (extreme left axis deviation)
ECG - Ventricular Tachycardia in panel (c) above:
The rapid, wide, bizarre QRS complexes with regular rhythm are clearly visible in the comparison image (panel c).
8. Ventricular Fibrillation (VF)
What it is: Completely chaotic, disorganised ventricular electrical activity - no coordinated contraction, no cardiac output. Immediately life-threatening - causes sudden cardiac death within minutes.
ECG Changes:
- No recognisable P waves, QRS complexes, or T waves
- Irregular, chaotic deflections of varying amplitude and morphology
- Rate impossible to determine (electrical chaos)
- Coarse VF: larger oscillations (>3 mm) - more likely to respond to defibrillation
- Fine VF: small oscillations (<3 mm) - longer duration, worse prognosis
ECG - Ventricular Fibrillation in panel (d) above:
Panel (d) in the comparison image shows the characteristic chaotic waveline with total absence of organised electrical activity.
9. Pulmonary Embolism (PE)
What it is: Acute obstruction of pulmonary vasculature causes acute right heart strain, elevated RV pressure, and RV dilatation. ECG changes reflect acute cor pulmonale.
ECG Changes:
- Most common finding: Sinus tachycardia (in >40% of cases)
- S1Q3T3 pattern (McGinn-White sign): Deep S wave in lead I + Q wave in lead III + T wave inversion in lead III
- Right bundle branch block (RBBB) - new, incomplete or complete
- Right axis deviation
- ST depression in V1-V4 and T-wave inversions in right precordial leads
- P pulmonale - tall peaked P waves in II (right atrial enlargement)
- Atrial fibrillation or flutter may develop
- ECG may be normal in 20-30% of cases
Note: The classic S1Q3T3 pattern is actually present in only ~20% of PE cases. Sinus tachycardia is far more common and sensitive.
10. Wolff-Parkinson-White Syndrome (WPW)
What it is: Congenital accessory bypass tract (Bundle of Kent) directly connects atria to ventricles, bypassing the AV node. Causes ventricular pre-excitation and predisposes to life-threatening tachyarrhythmias (SVT, AF with rapid ventricular response).
ECG Changes (in sinus rhythm):
- Short PR interval (<120 ms) - ventricles pre-excited before normal AV node conduction
- Delta wave - slurred slow upstroke at the start of the QRS (the pre-excitation wave)
- Wide QRS (>110 ms) - total widening from delta wave
- Pseudo ST-T changes - secondary repolarisation abnormalities (can mimic MI)
- Pseudo-Q waves in some leads (can mimic infarction)
Type A WPW (positive delta in V1): left-sided accessory pathway
Type B WPW (negative delta in V1): right-sided accessory pathway
ECG - Atrial fibrillation with rapid ventricular response in WPW:
The pericarditis ECG above also illustrates how broad bizarre complexes can occur when AF conducts via an accessory pathway.
See the LITFL WPW delta wave guide for example ECGs with delta waves clearly labelled.
Summary Table
| # | Condition | Key ECG Finding | Leads Affected |
|---|---|---|---|
| 1 | STEMI | ST elevation + Q waves | Territory-specific |
| 2 | NSTEMI/UA | ST depression + T inversion | Widespread or localised |
| 3 | Atrial Fibrillation | No P waves, irregular RR | All leads |
| 4 | Complete Heart Block | P-QRS dissociation, slow escape | All leads |
| 5 | Acute Pericarditis | Diffuse concave ST elevation + PR depression | All except aVR, V1 |
| 6 | LVH | High voltage + lateral strain | V5-V6, I, aVL |
| 7 | Ventricular Tachycardia | Wide QRS >120ms, rate 100-250 | All leads |
| 8 | Ventricular Fibrillation | Chaotic baseline, no QRS | All leads |
| 9 | Pulmonary Embolism | S1Q3T3, RBBB, sinus tach | I, III, V1-V4 |
| 10 | WPW Syndrome | Short PR, delta wave, wide QRS | All leads (varies by pathway) |
Sources:
- Harrison's Principles of Internal Medicine 22E (2025), Chapter 247: Electrocardiography
- Braunwald's Heart Disease, 2 Vol Set, Chapter 68: High-Grade AV Block
- Goldman-Cecil Medicine, Chapter 51: Bradyarrhythmias
- The Washington Manual of Medical Therapeutics: AV conduction disturbances
- LITFL ECG Library (litfl.com)
- JETem: Acute Pericarditis ECG
This is a shared conversation. Sign in to Orris to start your own chat.