Anatomy of anterior chamber
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Finding Sources
I now have rich material from multiple authoritative sources with excellent diagrams. Let me compile the full, detailed answer.
Anatomy of the Anterior Chamber
Overview
The anterior chamber (AC) is the fluid-filled space in the anterior segment of the eye. It is part of the anterior segment along with the cornea, iris, ciliary body, and lens.
Boundaries:
- Anterior wall: Posterior surface of the cornea (corneal endothelium)
- Posterior wall: Anterior surface of the iris and the anterior surface of the crystalline lens (within the pupillary space)
- Periphery (laterally): The iridocorneal (anterior chamber) angle - formed by the trabecular meshwork at the junction of the peripheral cornea and root of the iris
"The anterior chamber is bounded anteriorly by the cornea, laterally by the trabecular meshwork, and posteriorly by the iris." - Robbins & Cotran Pathologic Basis of Disease
Key Structural Diagram
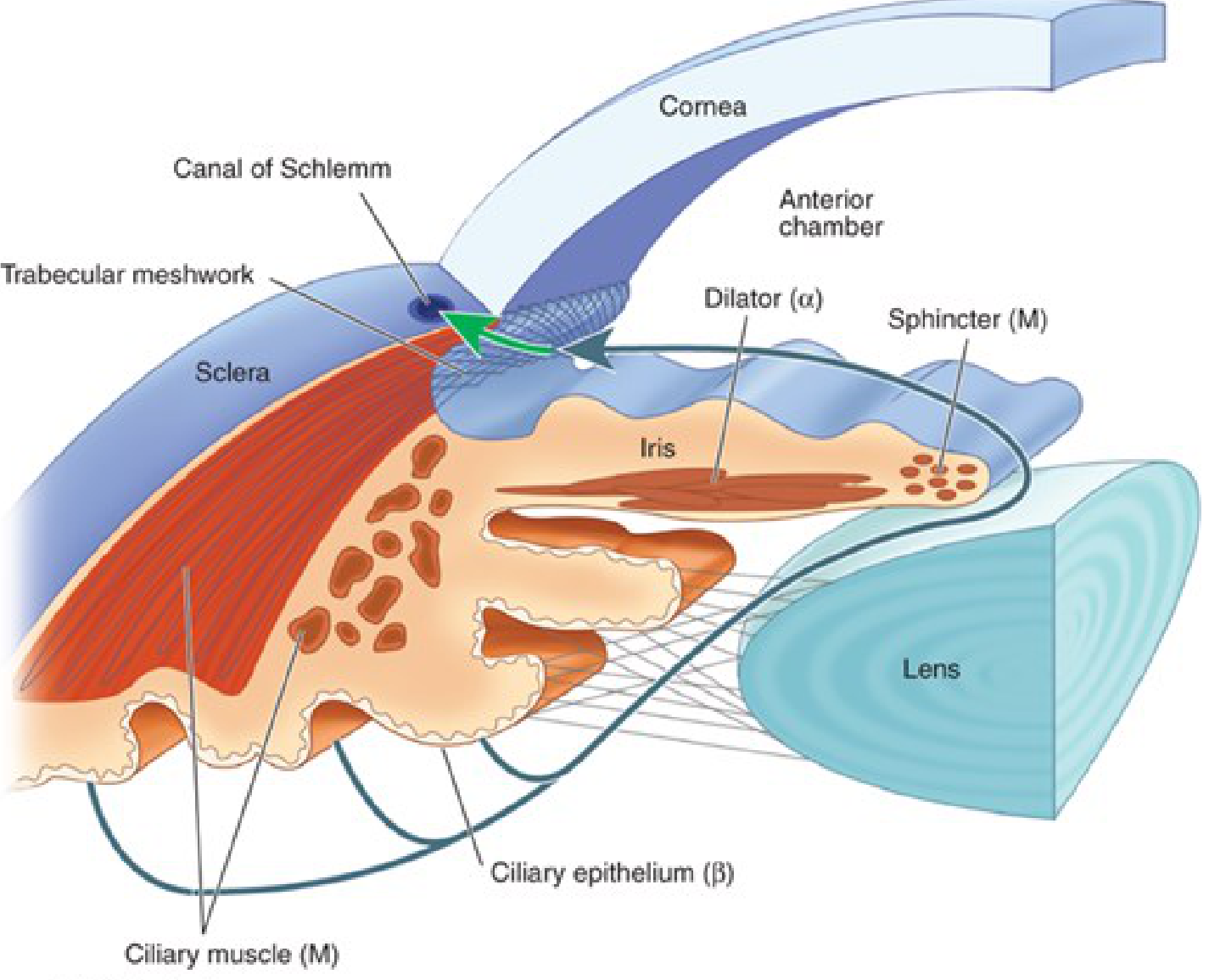
Contents
The anterior chamber is filled with aqueous humor - a clear, watery fluid produced by the pars plicata of the ciliary body (non-pigmented ciliary epithelium). Aqueous humor:
- Is secreted into the posterior chamber (space between the iris posteriorly and lens anteriorly)
- Passes through the pupil into the anterior chamber
- Drains through the trabecular meshwork at the iridocorneal angle into the canal of Schlemm, and then into collector veins
Normal aqueous humor is transparent; it provides oxygen, glucose, and amino acids to the avascular cornea and lens.
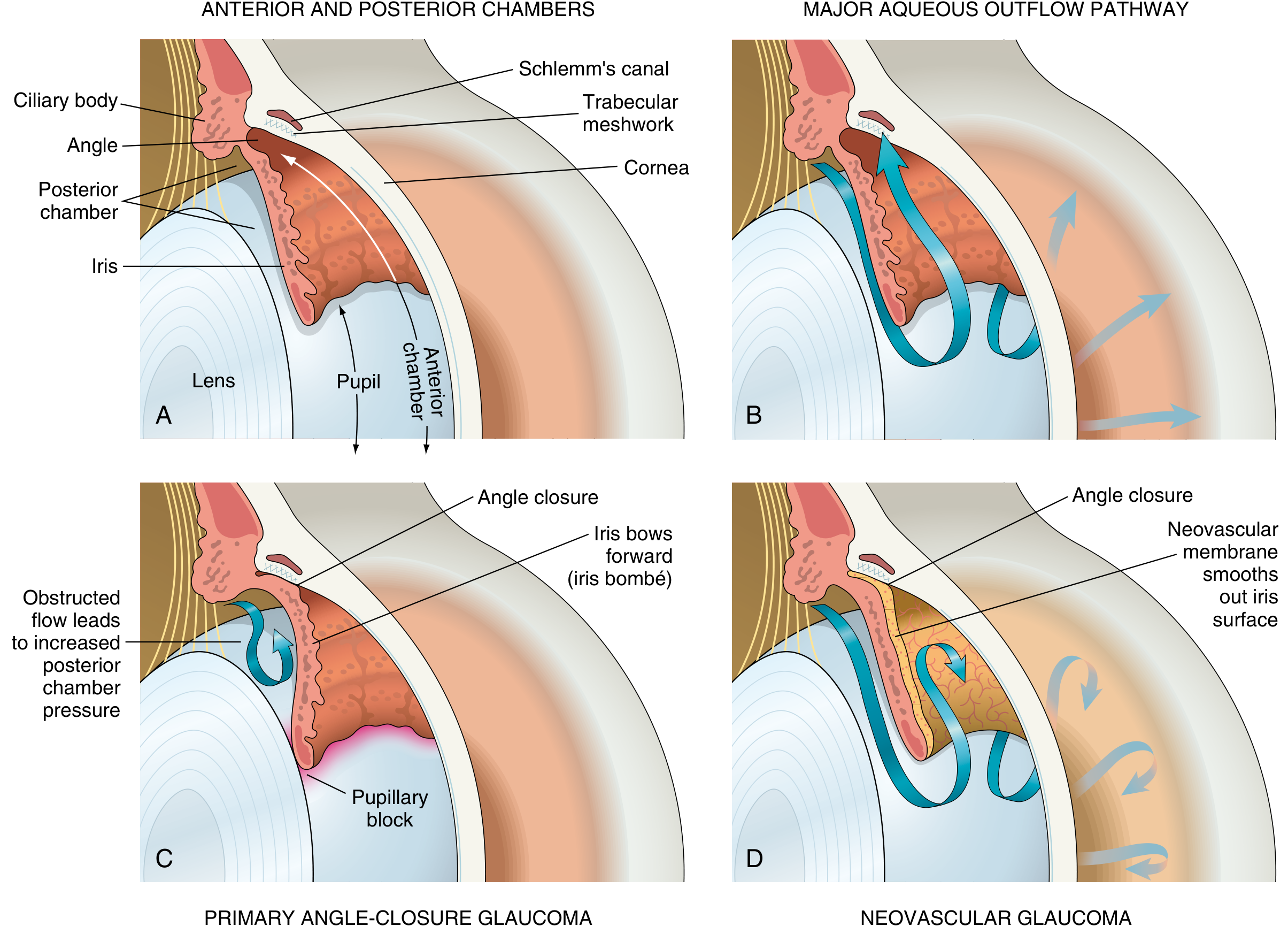
The Anterior Chamber Angle (Iridocorneal Angle)
This is the most clinically important part of the anterior chamber, assessed by gonioscopy. Moving from anterior to posterior, the structures visible at the angle are:
| Gonioscopic Landmark | Notes |
|---|---|
| Schwalbe's line | Most anterior; the peripheral termination of Descemet's membrane; marks the junction of corneal endothelium and trabecular meshwork |
| Trabecular meshwork | A meshwork of connective tissue that filters aqueous humor; the posterior (juxtacanalicular) portion is the main site of resistance to outflow |
| Scleral spur | A white/grey line; the posterior extension of sclera; attachment point for the longitudinal ciliary muscle fibers |
| Ciliary body band | A brown/grey band representing the anterior face of the ciliary body |
| Iris root | The most posterior structure; peripheral insertion of the iris |
The angle is formed at the junction of the peripheral cornea and the anterior surface of the iris root.
Dimensions
- Depth: The central AC depth is approximately 2.5-3.0 mm in adults (shallower in hyperopes, deeper in myopes and pseudophakic eyes)
- Volume: Approximately 250 µL
- The depth decreases with age as the lens enlarges
Aqueous Humor Formation and Drainage
Formation: The non-pigmented ciliary epithelium secretes aqueous humor via:
- Active secretion (Na/K-ATPase dependent) - primary mechanism
- Ultrafiltration
- Simple diffusion
Drainage pathways:
- Conventional (trabecular) pathway (~75-90%): Aqueous flows through the trabecular meshwork → Schlemm's canal → aqueous collector channels → episcleral veins → general circulation. This is the main resistance site in glaucoma.
- Uveoscleral (unconventional) pathway (~10-25%): Aqueous passes through the ciliary muscle bundles into the suprachoroidal space and drains via the scleral vasculature. Prostaglandin analogs enhance this pathway.
"Most of the aqueous humor drains through the trabecular meshwork situated in the angle formed by the intersection between the corneal periphery and the anterior surface of the iris." - Robbins, Cotran & Kumar
The Posterior Chamber
The posterior chamber is anatomically distinct from but continuous with the anterior chamber through the pupil:
- Bounded by: posterior surface of the iris (anteriorly), the ciliary body (circumferentially), and the anterior surface of the vitreous
- The crystalline lens is located entirely within the posterior chamber
- The lens is suspended by zonular fibers (zonules of Zinn) attached to the ciliary body
Anterior Segment Composition and Embryology
"The anterior segment is composed of the cornea and the anterior and posterior chambers. Most of the anterior segment is derived from the skin and neural crest tissue." - Goldman-Cecil Medicine
Key structures in summary:
- Cornea - 5 layers (epithelium, Bowman's layer, stroma, Descemet's membrane, endothelium); avascular, maintained by aqueous humor and tear film
- Iris - Contains sphincter pupillae (M receptor; miosis) and dilator pupillae (alpha-1 receptor; mydriasis)
- Ciliary body - Produces aqueous; ciliary muscle (M receptor) controls accommodation via zonular relaxation
- Trabecular meshwork - Main site of aqueous outflow resistance
- Canal of Schlemm - Circumferential channel that collects aqueous
Autonomic Innervation of Anterior Chamber Structures
| Structure | Receptor | Effect |
|---|---|---|
| Sphincter pupillae | Muscarinic (M) | Miosis |
| Dilator pupillae | Alpha-1 (α) | Mydriasis |
| Ciliary muscle | Muscarinic (M) | Contraction → accommodation |
| Ciliary epithelium | Beta-2 (β) | Aqueous secretion (beta-blockers reduce IOP by blocking this) |
Clinical Correlations
| Condition | Mechanism |
|---|---|
| Acute angle-closure glaucoma | Pupillary block causes iris bombé, peripheral iris occludes trabecular meshwork → IOP spike |
| Hyphema | Blood in the anterior chamber from trauma or neovascularization |
| Hypopyon | Pus layering inferiorly in the AC - seen in severe uveitis, endophthalmitis, corneal ulcer |
| Cell and flare | Protein and cells in aqueous due to inflammation; seen on slit-lamp |
| Shallow anterior chamber | Seen in hyperopia, nanophthalmos, post-operative states, choroidal detachment |
Sources:
- Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 1211-1212
- Robbins & Kumar Basic Pathology, p. 2362
- Goldman-Cecil Medicine, pp. 2596-2601
- Katzung's Basic & Clinical Pharmacology, 16th Ed., p. 166
- Kanski's Clinical Ophthalmology, 10th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.