Teach me glaucoma, an Ophthalmology topic in sufficient detail to excel in my theory and mcq exams. Use images illustrations flowcharts and summary table to make me remember the topic. Teach in a way like you are teaching a high school student. And enough detail to cover every aspect.
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
Here is your complete, exam-ready guide to Glaucoma - based on Kanski's Clinical Ophthalmology 10th Edition.
🎯 GLAUCOMA - Complete Study Guide
"Glaucoma is the silent thief of sight - it slowly steals your vision before you even notice."
📌 SECTION 1: WHAT IS GLAUCOMA? (Definition)
Think of your eye like a ball filled with fluid. The fluid is called aqueous humor. It is constantly being made and drained. When the drainage doesn't work properly, pressure builds up inside the eye - just like squeezing a water balloon. This raised pressure crushes the optic nerve (the cable connecting the eye to the brain), slowly killing vision.
Official definition:
Glaucoma is a group of conditions sharing a chronic progressive optic neuropathy that results in characteristic damage to the optic nerve head and retinal nerve fibre layer (RNFL). Progressive retinal ganglion cell (RGC) death and visual field loss follow. IOP is the key modifiable factor.
📌 SECTION 2: AQUEOUS HUMOR DYNAMICS (The "WHY" of Glaucoma)
How aqueous humor is made and drained:
╔══════════════════════════════════════════════════════════════════╗
║ AQUEOUS HUMOR FLOW - NORMAL EYE ║
║ ║
║ Ciliary Body ║
║ (Produces AH) ║
║ ↓ ║
║ Posterior Chamber → Pupil → Anterior Chamber ║
║ ↓ ║
║ Trabecular Meshwork (TM) ║
║ (Main drainage - 90%) ║
║ ↓ ║
║ Schlemm's Canal ║
║ ↓ ║
║ Episcleral Veins → Blood ║
║ ║
║ + Uveoscleral outflow (10%) via ciliary body face ║
╚══════════════════════════════════════════════════════════════════╝
Normal IOP = 10-21 mmHg
- IOP is highest in the morning, lowest at night
- Formula: IOP = Rate of Aqueous Production / Facility of Outflow
- If drainage is blocked → IOP rises → optic nerve is compressed → nerve fibres die → vision lost
How damage happens at the optic nerve:
High IOP
↓
Mechanical compression of optic nerve axons at lamina cribrosa
+
Reduced blood flow to optic nerve head (ischaemia)
↓
Retinal Ganglion Cell (RGC) death
↓
RNFL thinning + Optic disc cupping
↓
Visual field defects (peripheral first → tunnel vision → blindness)
📌 SECTION 3: CLASSIFICATION OF GLAUCOMA
GLAUCOMA
│
┌────────────────┴─────────────────┐
PRIMARY SECONDARY
(no other cause) (another disease causes it)
│
┌─────┴──────┐
Open Angle Angle Closure
│ │
POAG PACG
(most (pupillary block
common common cause)
worldwide)
│
┌─────┴──────┐
Acute PACG Chronic PACG
(emergency!) (gradual)
Also:
• Normal-Tension Glaucoma (NTG) - IOP normal but nerve damaged
• Ocular Hypertension (OHT) - IOP high but no nerve damage (yet)
• Congenital/Developmental Glaucoma
📌 SECTION 4: PRIMARY OPEN-ANGLE GLAUCOMA (POAG)
The Most Common Type - "The Silent Thief"
Key features:
- Adult onset, chronic, bilateral (usually asymmetric)
- Anterior chamber angle is OPEN
- No known cause (primary)
- Asymptomatic until late - patient loses peripheral vision first
Risk Factors:
| Risk Factor | Detail |
|---|---|
| Raised IOP | Most important modifiable factor |
| Age | Risk doubles every decade after 40 |
| Race | Black/African-American: 4-5x higher risk, more severe |
| Family history | First-degree relative: 3-9x risk |
| Thin cornea (CCT) | <555 µm is a risk factor |
| Myopia | High myopia increases risk |
| Disc haemorrhage | Marker of progression risk |
POAG Pathophysiology:
Trabecular meshwork dysfunction (increased resistance)
↓
Aqueous can't drain properly despite OPEN angle
↓
IOP rises
↓
Optic nerve head damage (cupping of disc)
↓
Loss of RNFL → Visual field defects
↓
Starts peripherally → concentric narrowing → tunnel vision → blindness
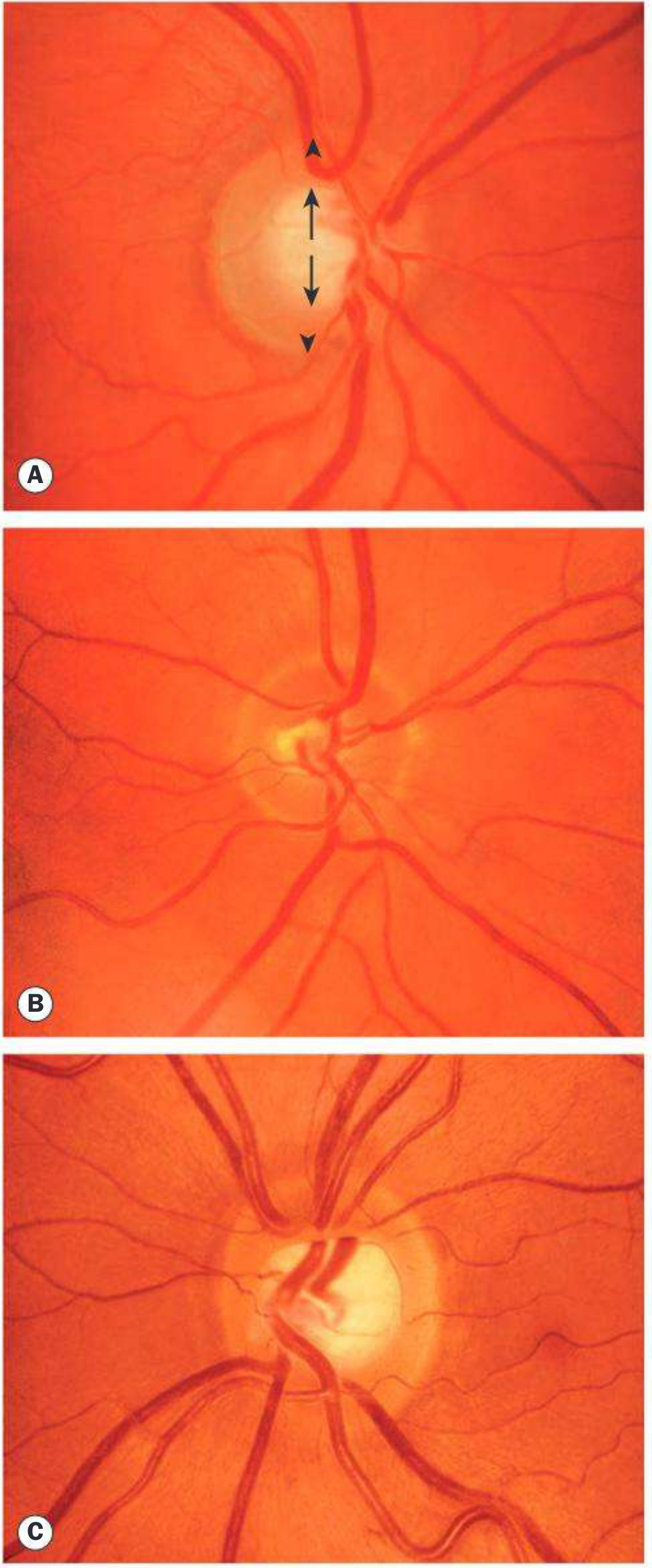
The Optic Disc in Glaucoma:
Normal optic disc vs Glaucomatous disc:
| Feature | Normal | Glaucoma |
|---|---|---|
| Cup:Disc ratio (C/D) | <0.5 (usually) | >0.6, asymmetry >0.2 |
| Neuroretinal rim (NRR) | Pink, healthy | Thinned/notched |
| ISNT Rule | Inf > Sup > Nas > Temp | Violated |
| Disc haemorrhage | Absent | May be present |
| RNFL | Intact | Thinned, wedge defects |
ISNT Rule (important MCQ): In a normal disc, the rim is thickest Inferiorly, then Superiorly, then Nasally, then Temporally. Glaucoma violates this rule.
Here is what a normal optic disc looks like - note the cup (white centre), the neuroretinal rim (orange ring), and the blood vessels:
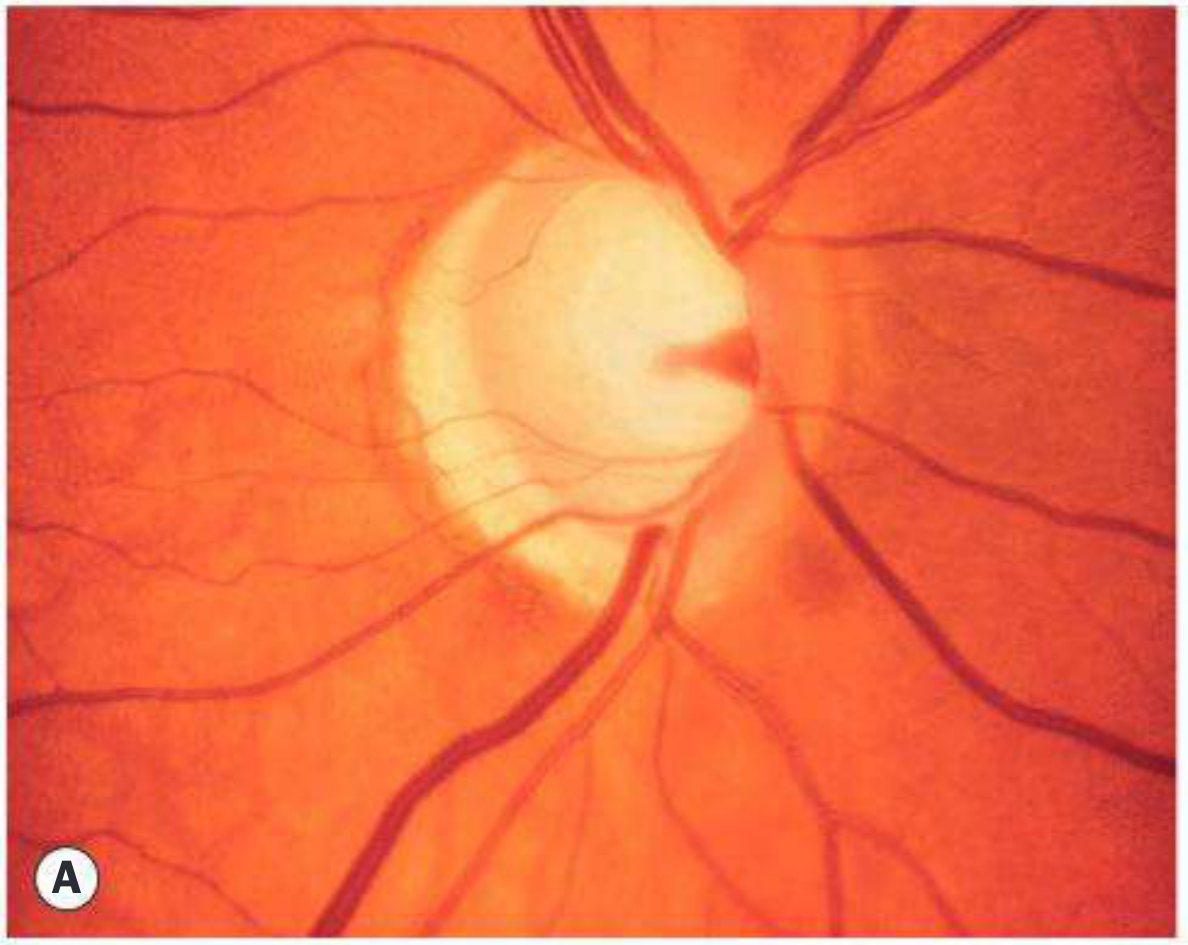
And here is advanced glaucomatous cupping - note the massively enlarged pale cup taking up most of the disc:
Visual Field Defects in Glaucoma (MCQ Favourite!):
Progression of visual field loss in glaucoma:
1. Baring of blind spot (early)
2. Paracentral scotoma (small blind patch near centre)
3. Arcuate scotoma (Bjerrum scotoma) - follows nerve fibre layer arc
4. Nasal step (defect crosses horizontal midline nasally)
5. Ring/annular scotoma (double arcuate)
6. Tunnel vision (only central island left)
7. Total blindness
Perimetry patterns tested:
- 24-2 pattern: Standard for glaucoma (24° temporal, 30° nasal)
- 10-2 pattern: For advanced glaucoma with central field threat
📌 SECTION 5: NORMAL-TENSION GLAUCOMA (NTG)
This is a confusing but important concept - the optic nerve is damaged even though IOP is normal (≤21 mmHg).
Why?
- The optic nerve is hypersensitive to normal pressure
- Vascular insufficiency / ischaemia plays a big role
- Associated with nocturnal hypotension, vasospasm, migraines, Raynaud's
Key associations of NTG:
- Flammer syndrome (vasospasm)
- Sleep apnea
- Systemic hypotension (especially nocturnal dips)
- Helicobacter pylori infection
How to distinguish NTG from other causes of low-IOP optic neuropathy:
Refer for neuroimaging if:
• VA loss out of proportion to cupping
• Color vision loss (Ishihara)
• Rapid progression despite normal IOP
• Optic disc pallor (pale NRR) → suggests compressive/ischaemic lesion
• Visual field defect not matching RNFL pattern
📌 SECTION 6: PRIMARY ANGLE-CLOSURE GLAUCOMA (PACG)
"The Dramatic Emergency of Glaucoma"
Key concept: The angle between the iris and the cornea is BLOCKED - aqueous cannot reach the trabecular meshwork at all.
Who gets it?
- Short (hypermetropic) eyes with shallow anterior chambers
- Asian populations (especially East and South Asian)
- Women > Men (2:1)
- Mean age: ~62 years
Mechanism - Pupillary Block (most common):
Hypermetropic (short) eye
↓
Shallow anterior chamber + anteriorly positioned lens
↓
Lens presses on iris → blocks aqueous flow through pupil
↓
Aqueous builds up in POSTERIOR chamber
↓
Pushes iris forward (iris bombe)
↓
Peripheral iris touches trabecular meshwork
↓
ANGLE CLOSES → IOP shoots up acutely
Types of PACG:
| Type | Features |
|---|---|
| Acute PACG (APAC) | Dramatic emergency, very high IOP (40-80 mmHg), painful |
| Subacute/Intermittent | Recurrent episodes of blurring + halos, resolves spontaneously |
| Chronic PACG | Gradual, like POAG but with peripheral anterior synechiae |
Clinical Features of Acute PACG (Exam Favourite!):
Symptoms:
- Sudden, severe unilateral eye pain
- Blurred vision + coloured halos around lights (like a rainbow around a streetlight - due to corneal oedema)
- Headache
- Nausea and vomiting (so severe it can mimic an abdominal emergency!)
- The attack is often precipitated by:
- Sitting in a dark room (pupil dilates → angle narrows)
- Emotional stress
- Anticholinergic drugs, topiramate, sympathomimetics
Signs:
- Eye is red (circumcorneal ciliary injection)
- Cornea is hazy/steamy (oedematous)
- Semi-dilated, fixed pupil (oval, mid-dilated, 4-6 mm) - KEY SIGN
- Shallow anterior chamber
- Very high IOP (sometimes >60 mmHg!)
- Tender eyeball
Precipitating Drugs to Remember (MCQ):
AVOID these drugs in narrow angle glaucoma:
• Anticholinergics (atropine, hyoscine, tricyclic antidepressants)
• Sympathomimetics (adrenaline, decongestants, phenylephrine)
• Topiramate (causes ciliary body swelling → anterior rotation of lens)
• Sulfa drugs
📌 SECTION 7: GONIOSCOPY (The Essential Examination)
Gonioscopy is the use of a special mirrored lens placed on the eye to look at the anterior chamber angle - the area between the iris and cornea where aqueous drains out. You CANNOT see this area without gonioscopy.
Structures seen from outside to inside (front to back):
Schwalbe's line (anterior border of TM)
↓
Trabecular meshwork (TM) - where aqueous drains
↓
Scleral spur (whitish ridge)
↓
Ciliary body band (brownish)
↓
Iris root
Mnemonic: "Silly Teenagers Should Climb Inward" → Schwalbe's, TM, Scleral spur, Ciliary body, Iris
Shaffer Grading System (Angle Width):
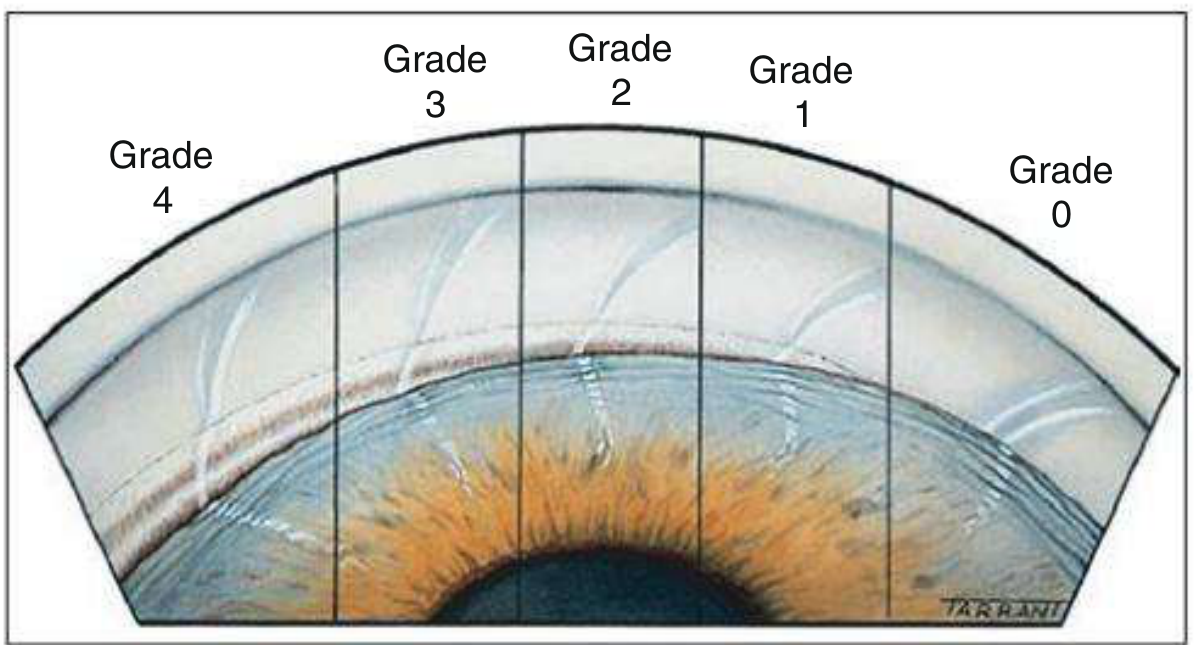
| Grade | Angle | Structures Visible | Closure Risk |
|---|---|---|---|
| 4 | 35-45° | All structures + ciliary body | None |
| 3 | 25-35° | Scleral spur visible | None |
| 2 | 20° | TM only, no scleral spur | Possible |
| 1 | 10° | Only Schwalbe's line | Likely |
| 0 | 0° | No structures, iridocorneal contact | Closed |
MCQ tip: Grade 0 and 1 are at risk of closure. Grade 3 and 4 are safe.
📌 SECTION 8: INVESTIGATIONS
GLAUCOMA WORKUP FLOWCHART
Patient suspected of Glaucoma
│
┌──────┴───────┐
│ HISTORY │ (symptoms, family history, medications, risk factors)
└──────┬───────┘
↓
┌──────┴───────┐
│ TONOMETRY │ IOP measurement
│ │ • Goldmann Applanation Tonometry (Gold Standard)
└──────┬───────┘ • Non-contact (air puff) - screening only
↓
┌──────┴───────┐
│ GONIOSCOPY │ Classify: Open angle vs Closed angle
└──────┬───────┘
↓
┌──────┴───────┐
│ FUNDOSCOPY │ Optic disc assessment
│ │ • C/D ratio, NRR, ISNT rule
│ │ • Disc haemorrhages
└──────┬───────┘
↓
┌──────┴───────┐
│ PERIMETRY │ Visual field testing
│ (Humphrey) │ • 24-2 or 30-2 standard
└──────┬───────┘ • 10-2 for advanced
↓
┌──────┴───────┐
│ OCT │ Structural imaging
│ │ • RNFL thickness map
│ │ • Ganglion Cell Layer analysis
│ │ • Optic disc parameters
└──────┬───────┘
↓
┌──────┴───────┐
│ PACHYMETRY │ Central Corneal Thickness (CCT)
│ │ • Thin cornea = underestimated IOP + more risk
│ │ • Thick cornea = overestimated IOP
└──────────────┘
Goldmann Applanation Tonometry (GAT):
- Gold standard for IOP measurement
- Principle: force required to flatten a fixed area (3.06 mm diameter) of cornea
- Correction for CCT: Thin cornea (CCT <555 µm) → add correction (IOP underestimated); Thick cornea → subtract
📌 SECTION 9: SECONDARY GLAUCOMAS (Quick Reference)
Open-Angle Secondary Glaucomas:
| Type | Mechanism | Key Features |
|---|---|---|
| Pseudoexfoliation Glaucoma | Flaky material clogs TM | Most common secondary glaucoma worldwide; white flakes on lens capsule |
| Pigmentary Glaucoma | Pigment from iris clogs TM | Young myopic males; Krukenberg spindle on cornea; iris transillumination defects |
| Steroid-induced | Steroids reduce TM outflow | Any steroid route (drops, inhaled, systemic); reversible early |
| Phacolytic | Lens proteins leak into AC, clog TM | Hypermature cataract |
| Ghost cell glaucoma | Degenerated RBCs after vitreous haemorrhage clog TM | Post-traumatic |
| Neovascular glaucoma | Fibrovascular membrane over angle | Caused by DR, CRVO, carotid disease; very difficult to treat |
Closed-Angle Secondary Glaucomas:
| Type | Mechanism | Key Features |
|---|---|---|
| Phacomorphic | Swollen lens → pushes iris forward | Intumescent cataract; treat by removing lens |
| Seclusio pupillae | 360° posterior synechiae block pupil | Chronic uveitis; iris bombe appearance |
| Malignant (ciliolenticular block) | Aqueous trapped in vitreous → pushes iris-lens diaphragm forward | Worsens with miotics; treat with cycloplegics + vitrectomy |
📌 SECTION 10: CONGENITAL GLAUCOMA (Primary)
Age of onset: Birth to 3 years (majority in first year)
Cause: Maldevelopment of the angle (trabeculodysgenesis) - the trabecular meshwork fails to develop properly
The Classic Triad (MCQ):
┌─────────────────────────────┐
│ 1. EPIPHORA (watering) │
│ 2. PHOTOPHOBIA │ ← "3 Ps" in infants
│ 3. BLEPHAROSPASM │
│ (squeezing eyelids) │
└─────────────────────────────┘
Buphthalmos = "ox eye" = enlargement of the entire eyeball in infants due to high IOP (the infant eye is distensible, unlike adult eyes)
- Corneal diameter >12 mm in a neonate = abnormal
- Haab's striae = horizontal breaks in Descemet's membrane from corneal stretching
Treatment: Surgery first (not medical) - Goniotomy or Trabeculotomy
📌 SECTION 11: MEDICAL TREATMENT
Mechanism and Examples:
TARGET: REDUCE IOP by either ↓ Aqueous Production OR ↑ Aqueous Outflow
| Drug Class | Example | Mechanism | IOP Reduction | Side Effects |
|---|---|---|---|---|
| Prostaglandin analogues ⭐ (1st line) | Latanoprost, Bimatoprost, Travoprost | ↑ Uveoscleral outflow | 25-35% | Iris pigmentation, eyelash growth (hypertrichosis), periorbital fat loss |
| Beta-blockers ⭐ (1st or 2nd line) | Timolol, Betaxolol | ↓ Aqueous production | 20-25% | Bradycardia, bronchospasm, depression; AVOID in asthma |
| Alpha-2 agonists | Brimonidine | ↓ Production + ↑ uveoscleral outflow | 20-25% | Allergy, dry mouth, drowsiness in children |
| Carbonic anhydrase inhibitors | Dorzolamide (eye drops), Acetazolamide (oral) | ↓ Aqueous production | 15-20% | Oral: metabolic acidosis, renal stones, paraesthesia; Avoid in sulfa allergy |
| Miotics (cholinergic) | Pilocarpine | ↑ Trabecular outflow (contracts ciliary muscle) | 20-25% | Pupil constriction, browache, myopia in young; used in angle closure |
| Rho-kinase inhibitor | Netarsudil | ↑ Trabecular outflow | ~20% | Eye redness (most common) |
MCQ Tip: Prostaglandins are used once daily at night. Beta-blockers reduce morning IOP peak effectively. Fixed combinations (e.g., Timolol + Dorzolamide = Cosopt) improve compliance.
📌 SECTION 12: LASER TREATMENT
| Procedure | Used For | How It Works |
|---|---|---|
| Laser Peripheral Iridotomy (LPI) | Acute/chronic PACG; pupillary block | Creates a hole in peripheral iris → aqueous bypasses pupillary block → angle opens |
| Laser Trabeculoplasty (SLT/ALT) | POAG; adjunct to meds | Burns/stimulates TM → improves outflow |
| Laser Iridoplasty | Plateau iris syndrome | Burns peripheral iris, pulling it away from angle |
| Cyclodiode laser | Last resort; refractory glaucoma | Destroys part of ciliary body → ↓ aqueous production |
LPI is the treatment for ALL cases of angle-closure - it is also done prophylactically in the fellow eye after acute PACG (since both eyes tend to have narrow angles).
📌 SECTION 13: SURGICAL TREATMENT
Trabeculectomy (Filtering Surgery) - Gold Standard
What happens in trabeculectomy:
Conjunctiva flap lifted
↓
Partial thickness scleral flap made
↓
Small block of trabecular tissue removed
↓
Creates a new drainage pathway
↓
Aqueous flows under conjunctival flap
↓
Forms a "bleb" (blister) under conjunctiva
↓
IOP controlled
Antimetabolites used to prevent scarring:
- Mitomycin C (MMC) - more potent, used in high-risk cases
- 5-Fluorouracil (5-FU) - less potent
Complications of trabeculectomy:
- Hypotony (IOP too low) → maculopathy
- Bleb-related infection (blebitis, endophthalmitis) - risk persists for life
- Cataract formation
- Flat anterior chamber
Other Surgical Options:
| Procedure | Indication |
|---|---|
| Glaucoma Drainage Devices (GDD/tubes) - e.g., Ahmed, Molteno, Baerveldt | Failed trabeculectomy; NVG; uveitic glaucoma |
| Goniotomy / Trabeculotomy | Congenital glaucoma (surgery of choice) |
| MIGS (Minimally Invasive Glaucoma Surgery) - e.g., iStent, Kahook, OMNI | Mild-moderate glaucoma; combined with cataract surgery |
📌 SECTION 14: MANAGEMENT OF ACUTE ANGLE CLOSURE - EMERGENCY PROTOCOL
ACUTE ANGLE CLOSURE ATTACK - EMERGENCY MANAGEMENT
IMMEDIATE MEASURES:
1. Lay patient SUPINE (gravity pulls lens back)
2. IV Acetazolamide 500 mg (↓ aqueous production rapidly)
3. Topical Timolol 0.5% (↓ production)
4. Topical Brimonidine 0.15% (↓ production)
5. Topical Pilocarpine 2% (constricts pupil, pulls iris away from angle)
⚠️ Pilocarpine is less effective when IOP is very high
6. IV Mannitol 1-2 g/kg (osmotic agent, reduces vitreous volume)
7. Oral/IV analgesics, antiemetics
Once IOP controlled:
8. Laser Peripheral Iridotomy (LPI) - DEFINITIVE TREATMENT
(+ prophylactic LPI to the other eye)
Target: Bring IOP below 35 mmHg within 1 hour, then <21 mmHg for LPI.
📌 SECTION 15: TARGET IOP CONCEPT
Not everyone needs the same pressure. The target IOP is the pressure below which further damage is unlikely:
Setting Target IOP:
Severe damage + high baseline IOP → lower target (e.g., <12 mmHg)
Mild damage + young patient → more aggressive (e.g., <15 mmHg)
Advanced Glaucoma Intervention Study (AGIS):
→ IOP consistently <18 mmHg = minimal progression risk
Initial reasonable goal = IOP < 18 mmHg
Progression despite target → lower target further OR consider surgery
📌 SECTION 16: SPECIAL SECONDARY GLAUCOMAS TO KNOW
Pseudoexfoliation Syndrome + Glaucoma
- White flaky material deposits on anterior lens capsule (classic "bull's eye" pattern), corneal endothelium, iris
- Causes: Weak zonules → lens subluxation; raised IOP → glaucoma
- Most common secondary open-angle glaucoma worldwide
- Responds poorly to medical treatment; often needs surgery early
Pigment Dispersion Syndrome (PDS) + Pigmentary Glaucoma
- Pigment rubs off iris by lens zonules → goes into aqueous → clogs TM
- Classic features:
- Krukenberg spindle (vertical brown spindle on cornea)
- Radial spoke-like iris transillumination defects
- Dense band of trabecular hyperpigmentation
- Typically: Young, myopic males
- Exercise can precipitate pigment dispersion attacks
- Treatment: Laser iridotomy, prostaglandins, miotics (poorly tolerated)
Neovascular Glaucoma (NVG)
- New blood vessels grow over the angle (rubeosis iridis) from ischaemic retinal disease
- Causes: Diabetic retinopathy, CRVO (central retinal vein occlusion), carotid occlusive disease
- Treatment: Anti-VEGF injections + panretinal photocoagulation (treat cause); GDD surgery
📌 SECTION 17: MASTER COMPARISON TABLE - POAG vs PACG
| Feature | POAG | PACG (Acute) |
|---|---|---|
| Onset | Insidious (silent) | Sudden (dramatic emergency) |
| Symptoms | Asymptomatic until late | Severe pain, redness, blurred vision, haloes, nausea/vomiting |
| IOP | Gradually raised | Markedly raised (40-80 mmHg) |
| Anterior chamber | Deep | Shallow |
| Cornea | Clear | Hazy/steamy (oedematous) |
| Pupil | Normal | Mid-dilated, fixed, oval |
| Angle (gonioscopy) | Open | Closed |
| Iris | Flat | Bombé (pushed forward) |
| Vision loss | Peripheral first | Sudden, severe |
| Racial predilection | Black/Caucasian | Asian |
| Refraction | Myopia | Hypermetropia |
| First-line treatment | Prostaglandin drops | IV Acetazolamide + Pilocarpine → LPI |
| Definitive surgical Rx | Trabeculectomy | LPI |
📌 SECTION 18: KEY CLINICAL TRIALS TO KNOW (MCQ Exam)
| Trial | Key Finding |
|---|---|
| OHTS (Ocular Hypertension Treatment Study) | Treating OHT reduces 5-yr risk of POAG from 9.5% to 4.4% |
| EMGT (Early Manifest Glaucoma Trial) | Treating elevated IOP reduces progression risk significantly; PXEG progresses fastest (-3.13 dB/yr) |
| AGIS | IOP consistently <18 mmHg = minimal visual field progression |
| CNTGS (Collaborative NTG Study) | Reducing IOP by 30% slows progression in NTG |
| LiGHT Trial | Selective Laser Trabeculoplasty (SLT) as first-line is at least as effective as drops |
📌 SECTION 19: QUICK-FIRE MCQ MEMORY TRICKS
🧠 MNEMONICS & MEMORY AIDS
1. ISNT RULE - Normal rim thickness:
"I Saw Numerous Things"
Inferior > Superior > Nasal > Temporal
2. Congenital glaucoma signs:
"3 Bs" = Buphthalmos, Buphthalmos... no wait:
"3 EBs" = Epiphora, Blepharospasm, photophoBia
3. Drugs to AVOID in angle-closure:
"ACE" = Anticholinergics, Cycloplegics, Epinephrine/sympathomimetics
(Also: topiramate!)
4. Gonioscopy mnemonic (structures in angle, front to back):
"Silly Teachers Should Come In"
Schwalbe's line, TM, Scleral spur, Ciliary body, Iris
5. Prostaglandin side effects:
"PIER" = Pigmentation (iris), Increased lashes, Eye redness, pRetinal oedema (rare)
6. Trabeculectomy antimetabolites:
"MMC > 5-FU" (MMC = Mitomycin C is more potent)
7. Layers damaged in glaucoma:
Retinal Ganglion Cells → their axons = RNFL
"RGC axons are the RNFL, RNFL loss = disc cupping"
📌 SECTION 20: COMPLETE SUMMARY TABLE
| Category | POAG | NTG | PACG (Acute) | Congenital |
|---|---|---|---|---|
| Age | >40 yrs | Adult | ~62 yrs | Birth - 3 yrs |
| IOP | >21 | Normal (≤21) | Very high (40-80) | High |
| Angle | Open | Open | Closed | Poorly developed |
| Symptoms | None (early) | None (early) | Pain, halos, N/V | Epiphora, photophobia, blepharospasm |
| Key sign | Large C/D ratio | Disc haemorrhage, notching | Steamy cornea, semi-dilated pupil | Buphthalmos, Haab's striae |
| Race | Black, Caucasian | Any | Asian, women | Any |
| Refraction | Myopia | Any | Hypermetropia | N/A |
| 1st line Rx | Prostaglandin drops | Prostaglandin drops | IV Acetazolamide + Pilocarpine | Surgery (Goniotomy) |
| Definitive Rx | Trabeculectomy | Trabeculectomy if progressive | Laser Peripheral Iridotomy | Goniotomy/Trabeculotomy |
| Prognosis | Slow progression | Variable | Good if treated fast | Good with early surgery |
📌 SECTION 21: FLOWCHART - CLINICAL APPROACH TO A GLAUCOMA PATIENT
Patient with suspected glaucoma
│
Measure IOP (Goldmann Applanation)
│
┌────────┴─────────┐
IOP > 21 IOP ≤ 21
│ │
↓ ↓
Gonioscopy Suspect NTG
│ (if optic disc damaged)
│
┌─┴──────────┐
Open Closed
│ │
POAG or PACG or
Secondary Secondary
OAG CAG
│ │
↓ ↓
Optic disc Acute attack?
assessment │ │
│ YES NO
Perimetry │ │
│ Emergency LPI
OCT Rx prophylaxis
│
Target IOP?
│
Medical → Laser → Surgery
📌 EXAM TIPS - What Examiners Love to Ask
- "Most common cause of blindness worldwide" → Cataract (#1); Glaucoma (#2)
- "Gold standard for IOP measurement" → Goldmann Applanation Tonometry
- "First sign of glaucoma" → RNFL loss (before visual field loss!) / Paracentral scotoma on perimetry
- "Semi-dilated, fixed, oval pupil + painful red eye + steamy cornea" → Acute angle closure EMERGENCY
- "First line drug for POAG" → Prostaglandin analogue (once daily at night)
- "Beta-blockers are contraindicated in" → Asthma, COPD, Heart block
- "Krukenberg spindle + spoke iris defects + young myope" → Pigmentary glaucoma
- "White flakes on lens + raised IOP" → Pseudoexfoliation glaucoma
- "Goniotomy/trabeculotomy" → Treatment of congenital glaucoma
- "Pilocarpine mechanism" → Contracts ciliary muscle → opens TM spaces → increases outflow
- "Malignant glaucoma worsens with" → Miotics (pilocarpine makes it worse!)
- "Sturge-Weber + glaucoma" → Occurs in 30% ipsilateral to facial haemangioma
Source: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition. This guide covers all high-yield exam topics for both theory and MCQ papers.
This is a shared conversation. Sign in to Orris to start your own chat.