Principles of management of urethral injury
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive, high-quality content from multiple authoritative urology textbooks. Let me compile the full answer.
Principles of Management of Urethral Injury
Overview and Anatomical Classification
Urethral injuries are divided into anterior and posterior based on their relationship to the urogenital diaphragm:
- Posterior urethra: membranous + prostatic urethra (proximal to urogenital diaphragm). Almost always injured by pelvic fracture - hence called Pelvic Fracture Urethral Injury (PFUI).
- Anterior urethra: bulbar + penile (distal) urethra. Typically from straddle injuries or penetrating trauma.
Diagnosis - First Steps
Do NOT attempt urethral catheterization if urethral injury is suspected. The cardinal signs are:
- Blood at the urethral meatus - the single most important sign
- Inability to urinate / urinary retention
- High-riding prostate on rectal exam (unreliable - often absent with partial tears)
- Butterfly perineal hematoma - seen in anterior urethral (straddle) injuries
- Pelvic fracture on X-ray / CT
Retrograde Urethrogram (RUG) is the mandatory diagnostic investigation:
- Place a 16-Fr catheter 1 cm into the fossa navicularis, fill balloon with 3 mL water
- Inject 20-30 mL water-soluble contrast in oblique/lateral decubitus position
- Partial disruption: some contrast reaches the bladder
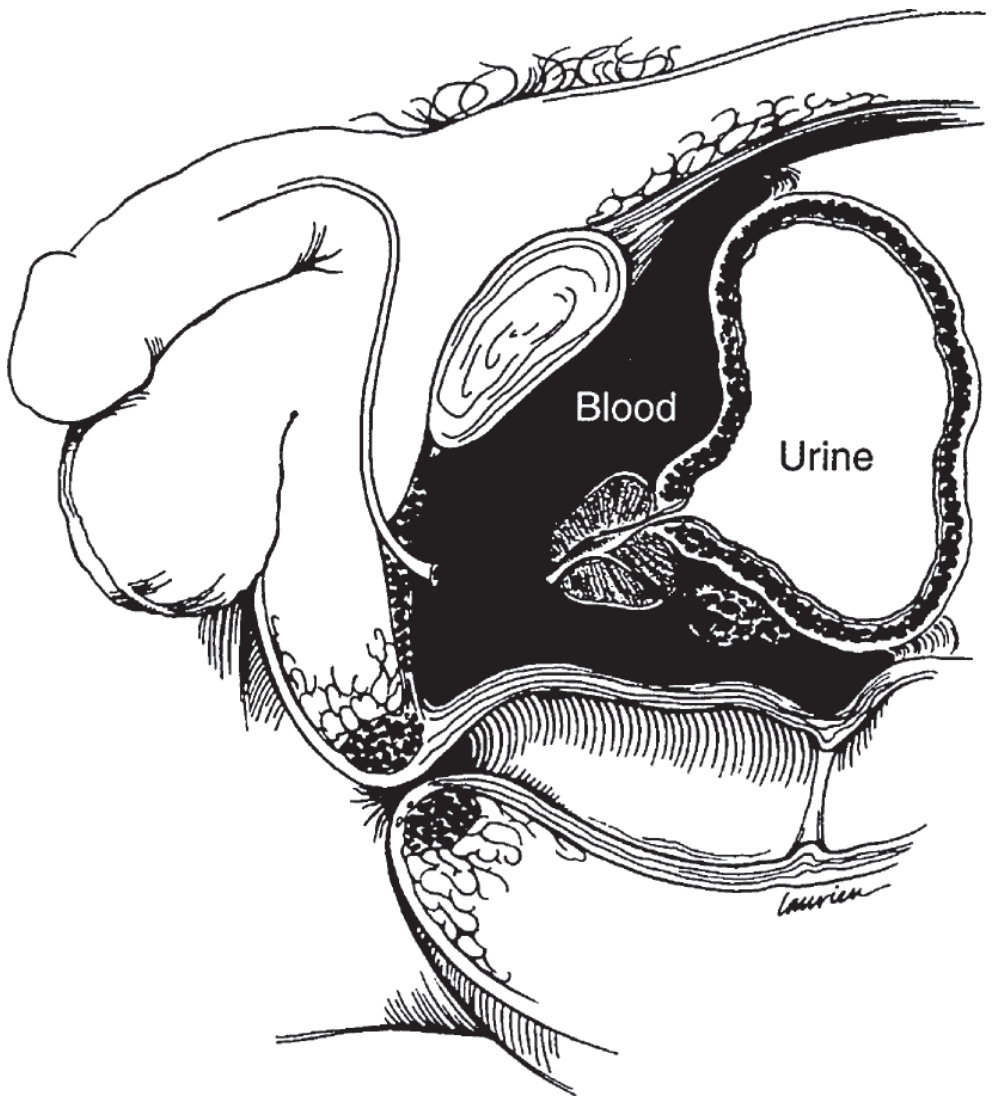
- Complete disruption: no contrast reaches the bladder; free extravasation into pelvis ("pie-in-the-sky" bladder displaced cephalad by hematoma)
"Blood at the urethral meatus is the single most important sign of urethral injury. The importance of this finding cannot be overemphasized, because an attempt to pass a urethral catheter may result in infection of the periprostatic and perivesical hematoma and conversion of an incomplete laceration to a complete one." - Smith and Tanagho's General Urology, 19th Ed
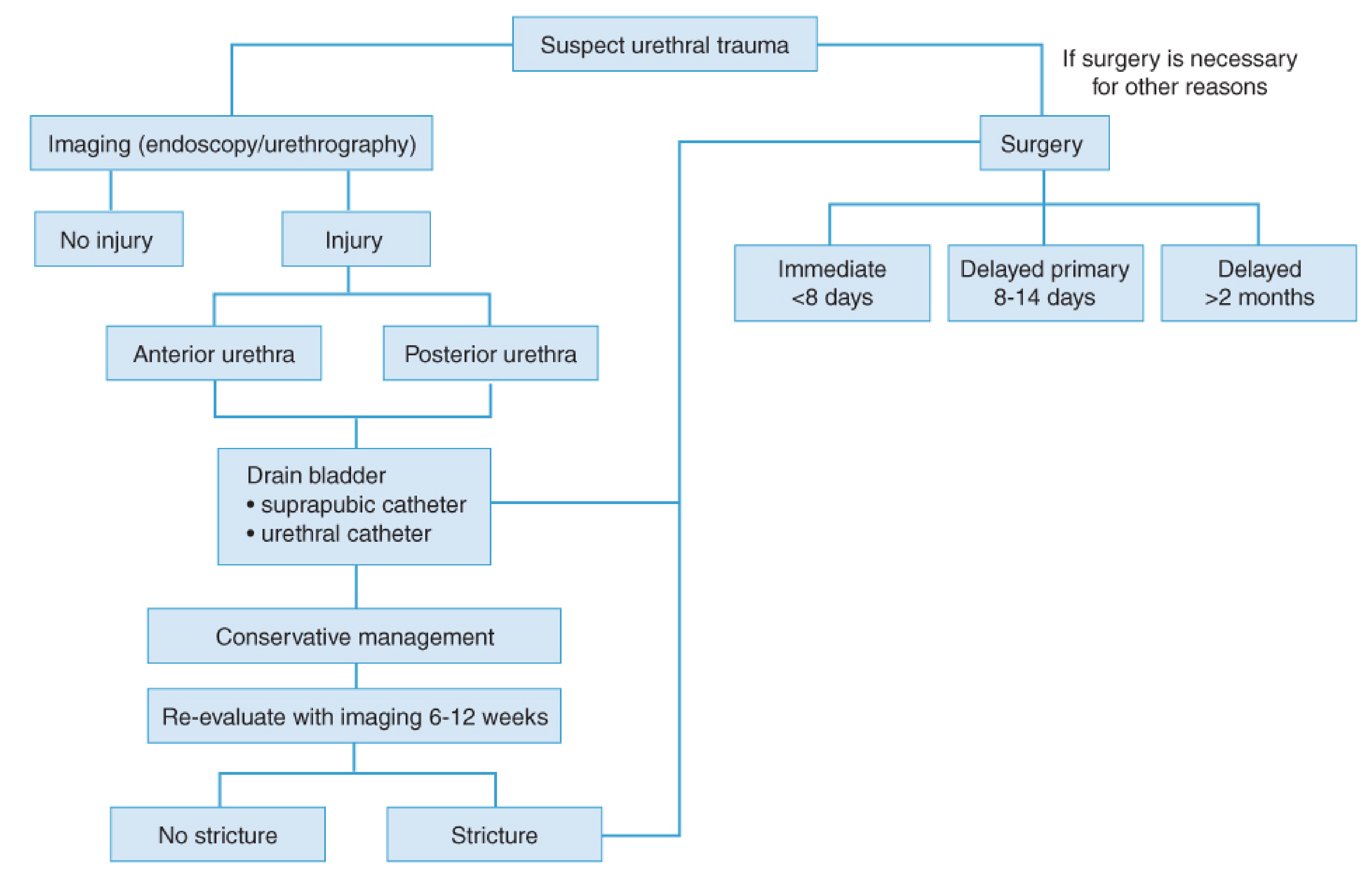
Management Algorithm
Management of Posterior Urethral Injury (PFUI)
The goals are: prompt urinary drainage in the acute setting and minimizing long-term morbidity (stricture, incontinence, erectile dysfunction).
A. Acute / Emergency Phase
Step 1: Treat haemorrhagic shock first. These are usually polytrauma patients.
Step 2: Bladder drainage - Suprapubic Cystostomy (SPT)
- SPT is the preferred initial treatment for most PFUI (AUA guidelines)
- Place carefully - pelvic hematoma may displace the bladder; use ultrasound guidance or open placement if needed
- Advantages: quick, avoids urethral manipulation, allows time for patient stabilization, preserves future reconstructive options
- Can be placed even in patients undergoing ORIF of pelvic fracture (no evidence it increases hardware infection risk)
Step 3: Decision between SPT alone vs. Primary Endoscopic Realignment
| Feature | SPT + Delayed Repair | Primary Endoscopic Realignment |
|---|---|---|
| Stricture rate | Very high (virtually all) but strictures may be more complex | High (~50-70%) but strictures may be shorter/simpler |
| Erectile dysfunction | ~30-35% | ~30-35% (similar) |
| Urinary incontinence | <5% | Similar |
| Timing | Immediate SPT, urethroplasty after 3 months | Within first week, in stable patients |
| Patient stability | Suitable for unstable/polytrauma | Hemodynamically stable only |
- Primary surgical repair (open) is NOT recommended - very high complication rates (incontinence, ED, 69% still develop strictures requiring further surgery)
- Exception: concurrent rectal injury or bladder neck injury requires primary repair to prevent fistula
Partial disruption: One gentle attempt at blind urethral catheter placement is reasonable (succeeds ~50%). Failed attempt does not convert partial to complete injury. If successful, maintain catheter 4-6 weeks.
Complete disruption: Proceed directly to SPT (preferred) or primary endoscopic realignment in stable patients.
B. Primary Endoscopic Urethral Realignment (for stable patients)
- Performed within the first week after injury
- Dual antegrade + retrograde cystoscopy with fluoroscopy to bridge the urethral defect
- Urethral catheter maintained for 4-6 weeks
- Pericatheter RUG or voiding cystourethrogram at catheter removal to assess outcome
- Prolonged attempts should be avoided - do not delay other life-saving care
C. Special Situations
- Female PFUI: Early primary repair within 7 days, especially if concurrent vaginal laceration
- Children: Higher risk of injury extending to bladder neck (rudimentary prostate); manage with extra caution
- Bladder neck injury or rectal injury: Primary operative repair required
D. Delayed Reconstruction - Posterior Urethroplasty
- Timing: After 3 months (allows pelvic hematoma resolution, prostate returns to anatomic position)
- Pre-operative: RUG + VCUG to delineate stricture length (typically 1-2 cm at prostatomembranous junction)
- Procedure of choice: Excision of stricture + end-to-end anastomotic urethroplasty (bulbar urethra to prostatic apex)
- Performed via perineal approach; pubectomy sometimes needed for access
- Success rate >90% in specialist centres
- Posterior urethroplasty is a complex operation - should be performed by reconstructive specialists
Management of Anterior Urethral Injury
Straddle (Blunt) Injuries - Bulbar Urethra
The bulbar urethra is crushed against the pubic rami. Presents with blood at meatus, inability to void, expanding perineal/scrotal hematoma with possible urine extravasation.
Management options:
- Immediate repair: For simple, uncomplicated injuries - minimal debridement, spatulated tension-free end-to-end anastomosis over catheter using fine absorbable suture. Success >95% for short (1.5-2 cm) strictures.
- Catheter alignment + delayed repair: Acceptable in selected cases.
- SPT + delayed reconstruction: Preferred for:
- High-velocity gunshot wounds / shotgun blasts
- Extensive tissue devitalisation (true extent of injury declares itself over time)
- Complex injuries with significant contamination
"Anastomotic urethroplasty is the procedure of choice in the totally obliterated bulbar urethra after a straddle injury... [with] success in more than 95% of cases." - Campbell Walsh Wein Urology
Do NOT use:
- Endoscopic incision/dilation for complete obliterations (doomed to failure)
- Repeated urethral dilations or DVIU for traumatic strictures (worsens fibrosis, makes subsequent reconstruction harder)
- UroLume stents - contraindicated in traumatic urethral strictures
Penetrating Anterior Urethral Injuries
- Hemodynamically stable + uncomplicated: Explore and repair primarily during index admission
- Technique: minimal debridement, spatulate the ends, primary repair over catheter with fine absorbable suture
- Extensive devitalisation / complicated injuries: SPT for urinary diversion + delayed reconstruction (typically >6 weeks)
Penile (Anterior) Urethra Injuries
- Often associated with penile fractures (tunical rupture)
- Urethral involvement in 11-29% of penetrating penile injuries
- Manage with urgent surgical exploration and primary repair
Complications to Prevent and Monitor
| Complication | Incidence | Notes |
|---|---|---|
| Urethral stricture | Virtually 100% after PFUI | Main long-term challenge; addressed with urethroplasty |
| Erectile dysfunction | 30-80% (mean ~50%) after posterior injury | Reduced to 30-35% with SPT + delayed repair |
| Urinary incontinence | <2-5% | Usually associated with bladder neck or sacral nerve injury |
| Urinoma/abscess | Preventable with early drainage | Reason for prompt SPT |
| Pelvic sepsis | Avoided by not manipulating hematoma | Risk with premature open repair |
Key Principles - Summary
- Never attempt urethral catheterization blindly when blood at meatus is present - do RUG first
- RUG is the diagnostic gold standard - defines partial vs complete disruption
- Immediate goal: secure bladder drainage (SPT is preferred for PFUI)
- Primary open repair of PFUI is contraindicated (except bladder neck/rectal injury)
- Partial disruption: single gentle catheter attempt acceptable
- Complete disruption: SPT (first choice) or primary endoscopic realignment in stable patients
- Delayed urethroplasty at 3 months is the definitive treatment for posterior disruption - success >90%
- Anterior straddle injuries: immediate anastomotic repair for uncomplicated injuries; SPT + delayed repair for complex/devitalised tissue
- Penetrating anterior injuries: immediate exploration + primary repair in stable patients
- Endoscopic dilation/DVIU has no role in complete traumatic obliterations
Sources: Campbell Walsh Wein Urology 3-Volume Set; Smith and Tanagho's General Urology, 19th Ed; Fischer's Mastery of Surgery, 8th Ed; Current Surgical Therapy, 14th Ed; Schwartz's Principles of Surgery, 11th Ed; Bailey and Love's Short Practice of Surgery, 28th Ed; Sabiston Textbook of Surgery
Torsion of testes
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Reading File
Loading Image
Loading Image
I now have excellent material from multiple authoritative sources plus high-quality images. Let me compile the comprehensive answer.
Torsion of the Testis
Testicular torsion is one of the few true urological emergencies. It results from twisting of the spermatic cord, which first obstructs venous outflow and then compromises arterial inflow, leading to ischemia and potentially irreversible infarction. Time to intervention is the single most important determinant of outcome.
Types of Torsion
1. Intravaginal Torsion (Bell-Clapper Deformity) - Most Common
The tunica vaginalis has an abnormally high insertion on the spermatic cord, enveloping the testis and lower epididymis completely. This allows the testis to hang freely and rotate within the tunica vaginalis like a clapper inside a bell. This anatomic defect is bilateral, present in ~12% of males.
- Predominantly seen in adolescents and young adults (peak at puberty)
- Incidence: ~1 in 4,000 males under 25 years
- Can occur at any age; has a bimodal distribution - first year of life and puberty
2. Extravaginal Torsion - Neonates
The entire spermatic cord, including the tunica vaginalis, twists. Occurs because the tunica vaginalis is not yet fixed to the scrotal wall. Seen in newborns (in utero or first 30 days of life).
- 70% prenatal (in utero), 30% postnatal
- Salvage rate for prenatal torsion: nearly zero
- Salvage rate for postnatal torsion: up to 44%
Pathophysiology
Torsion of the spermatic cord - venous outflow obstruction - vascular engorgement - thick-walled arteries remain patent - intense congestion - subsequent arterial compromise - hemorrhagic infarction
The degree of torsion and duration of ischemia determine viability. Torsion may range from 180° to >720°.
Predisposing Factors
- Bell-clapper deformity (bilateral, congenital)
- Undescended testis (cryptorchid) - more prone to torsion
- Trauma (minor blunt injury)
- Cold weather / cremasteric reflex contraction
- Rapid growth during puberty
- History of previous intermittent torsion
Clinical Features
Symptoms
- Sudden onset of severe unilateral scrotal/testicular pain - the hallmark
- Pain may radiate to the groin, lower abdomen, or flank
- Nausea and vomiting (common, due to visceral pain)
- History of similar intermittent episodes (intermittent torsion) - suggests bell-clapper deformity
- No urinary symptoms (differentiates from epididymitis)
- May wake from sleep with pain
Signs
- High-riding testis with transverse (horizontal) lie - due to shortening of the cord
- Absent cremasteric reflex - most reliable clinical sign
- Diffuse testicular tenderness
- Scrotal oedema and erythema (appear later, not early)
- Prehn's sign negative: elevation of testis does NOT relieve pain (contrast: elevation relieves pain in epididymitis - "Prehn's sign positive")
- A hard, firm testis may indicate late torsion with infarction
Differential Diagnosis - Acute Scrotum
| Feature | Testicular Torsion | Torsion of Appendix | Epididymo-orchitis |
|---|---|---|---|
| Age | <1 yr, puberty | 7-14 years | Adult |
| Onset | Sudden (hours) | 1-2 days | Days to weeks |
| Pain location | Entire testis | Upper pole | Epididymis |
| Testis position | High-riding, transverse | Normal, vertical | Normal, vertical |
| Cremasteric reflex | Absent | Intact | Intact |
| Nausea/vomiting | Yes | Usually absent | Possibly fever |
| Pyuria | Rare | No | Yes |
| Blue-dot sign | No | Yes (upper pole) | No |
| Doppler US | Absent/reduced flow | Normal flow | Increased flow |
| Treatment | Emergency surgery | Analgesia + rest | Antibiotics |
Investigations
Doppler Ultrasound
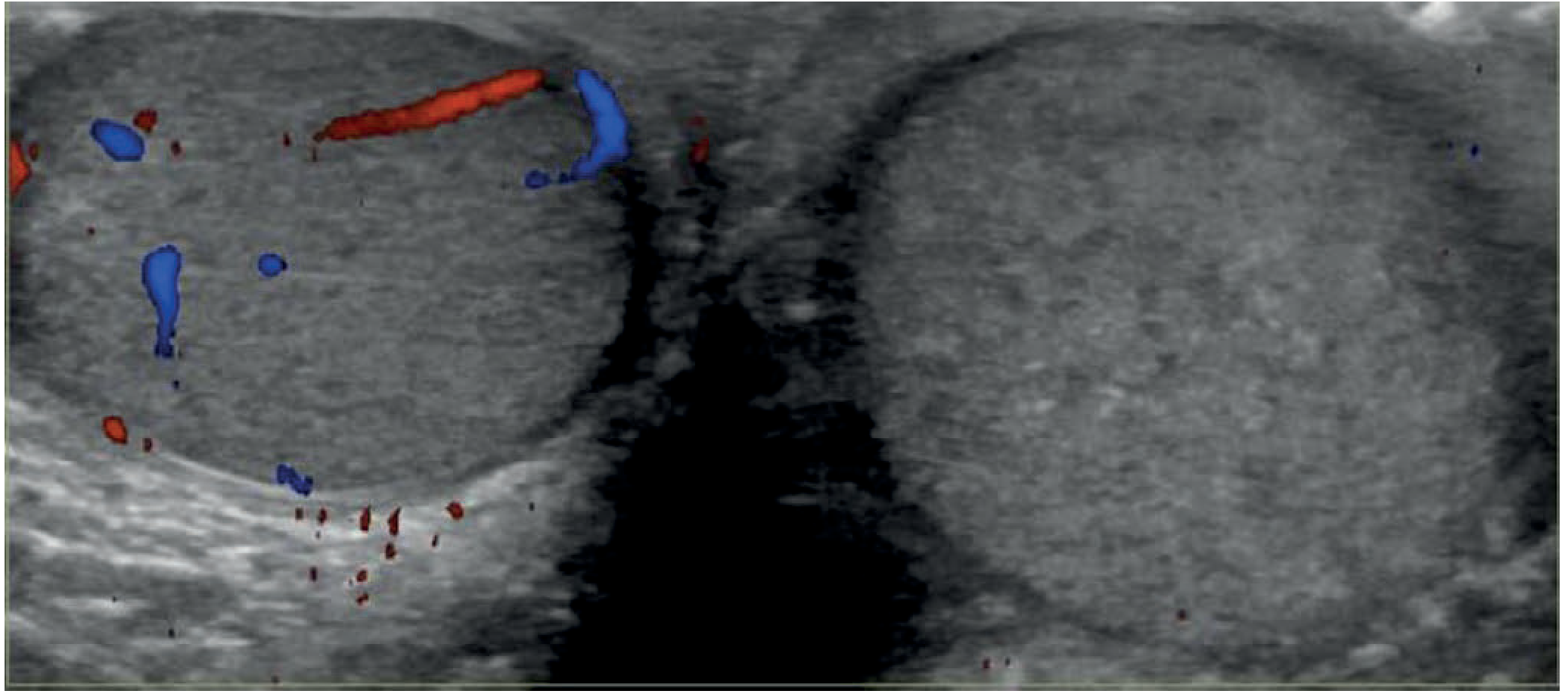
- Investigation of choice - sensitivity 96-100%, specificity 84-95%
- Shows absent or reduced blood flow in the torsed testis on colour Doppler
- Grayscale: testis may be diffusely hypoechoic and enlarged
- "Whirlpool sign": twisting of the spermatic cord above the testis - pathognomonic
- Heterogeneous echotexture = late torsion, likely non-viable testis
- Important: a negative ultrasound does NOT rule out torsion if clinical suspicion is high - do not delay surgical consultation for imaging
Other investigations
- Urinalysis: usually normal (pyuria suggests epididymitis, but may also occur with concurrent UTI in torsion)
- No specific blood tests are diagnostic
The diagnosis of testicular torsion is primarily clinical. If torsion is strongly suspected, do NOT wait for imaging - go directly to the operating room.
Management
TIME IS TESTIS - Salvage Rates by Duration
| Time from onset to detorsion | Testicular salvage rate |
|---|---|
| < 6 hours | >90% |
| 6-12 hours | ~50% |
| 12-24 hours | ~10% |
| >24 hours | Nearly 0% (orchiectomy usually required) |
Step 1: Manual Detorsion (Temporizing)
- May be attempted in the ED while preparing for surgery
- Testis usually rotates medially (toward midline); detorsion is performed by rotating it laterally ("opening a book" - outward rotation)
- Successful manual detorsion is evidenced by pain relief and return of Doppler flow
- Does NOT replace surgery - orchidopexy is still required after successful manual detorsion
- If pain worsens with one direction of rotation, try the opposite direction
Step 2: Emergency Surgical Exploration
Surgical exploration is the definitive treatment and should not be delayed. "If the diagnosis of testicular torsion is possible, then surgical exploration is indicated." - Bailey and Love
Approach: Midline scrotal (trans-scrotal) incision gives access to both testes.
Intraoperative steps:
- Deliver the testis and identify the twist
- Untwist the cord (detorsion)
- Assess viability - wrap in warm moist swabs for 5-10 minutes
- Pink testis with restored circulation → viable → orchidopexy
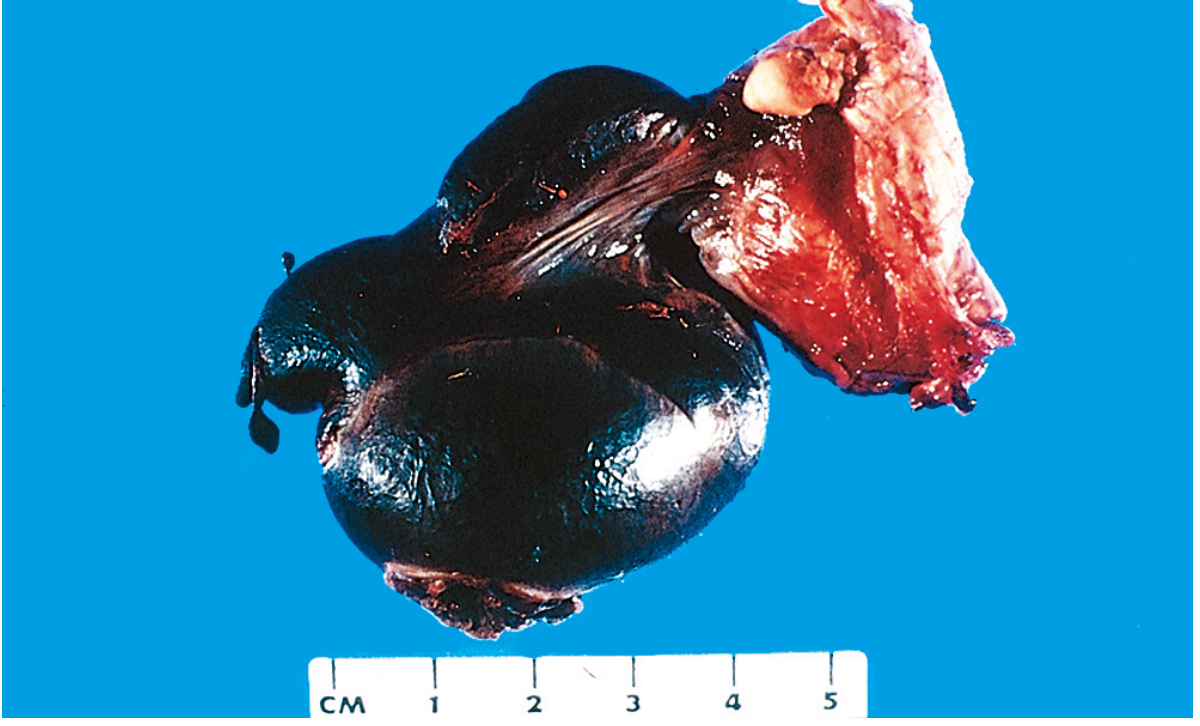
- Black/gangrenous testis with no return of colour → orchiectomy
- Only gangrenous testes should be excised - some severely compromised but non-gangrenous testes recover and those that subsequently atrophy are not harmful
Step 3: Orchidopexy - Fixation of Both Testes
The bell-clapper deformity is bilateral - the contralateral testis is at equal risk of torsion.
- If the torted testis is viable: bilateral orchidopexy (fixation of both testes)
- If the torted testis is non-viable (orchiectomy): contralateral orchidopexy is still mandatory
- Method of fixation: 3-point fixation of each testis to the dartos pouch using non-absorbable sutures (e.g. prolene), or fashioning a dartos pouch for each testis
- Absorbable sutures should NOT be used as they may dissolve before permanent fibrous fixation occurs
- Patient must be counselled and consented for orchidectomy before exploration
Neonatal Torsion (Extravaginal)
- Prenatal torsion: Non-urgent; testis nearly always non-viable; contralateral orchidopexy performed urgently to prevent asynchronous contralateral torsion
- Postnatal torsion: Treat as emergency - similar to adult torsion - low but real salvage rate (up to 44%)
- 93% of pediatric urologists would immediately explore a neonate with postnatal torsion
Torsion of the Appendix Testis (Hydatid of Morgagni)
A separate but important differential:
- Appendix testis = remnant of Müllerian duct; appendix epididymis = Wolffian remnant
- Both are small pedunculated structures at the upper pole - can twist and infarct
- Age: 7-14 years (most common cause of acute scrotum in this age group)
- Blue-dot sign: dark infarcted appendage visible through scrotal skin at upper pole
- Doppler US: normal testicular flow; may show increased perifocal flow
- Treatment: analgesia and rest (self-limiting); surgical exploration reserved for severe pain or equivocal diagnosis
- Does NOT require orchidopexy
Complications of Testicular Torsion
| Complication | Notes |
|---|---|
| Testicular infarction/atrophy | Main risk with delayed presentation |
| Infertility | Contralateral testicular damage possible (sympathetic orchidopathia / immune-mediated) |
| Hormonal deficiency | Rare, mainly if bilateral torsion |
| Psychological impact | Significant in adolescents post-orchiectomy |
Key Points Summary
- Testicular torsion is a surgical emergency - do not delay for investigations
- Bell-clapper deformity is the underlying anatomical defect in adolescent/adult torsion, and it is bilateral
- The classic triad: sudden onset pain + high-riding testis + absent cremasteric reflex
- Prehn's sign is negative in torsion (elevation does not relieve pain)
- Doppler US is the investigation of choice but must not delay surgery in clinically obvious cases
- Surgery within 6 hours gives >90% salvage rate
- After detorsion, assess viability before deciding on orchidopexy vs. orchiectomy
- Both testes must always be fixed - the contralateral testis is at equal anatomical risk
- Non-absorbable sutures must be used for orchidopexy
- Torsion of the appendix testis (blue-dot sign) is managed conservatively; testicular torsion always requires surgery
Sources: Rosen's Emergency Medicine 9th Ed; Bailey and Love's Short Practice of Surgery 28th Ed; Campbell Walsh Wein Urology 3-Volume Set; Robbins, Cotran & Kumar Pathologic Basis of Disease
Anatomical limits of ilio-inguinal block dissection.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive, well-illustrated answer. Let me compile it.
Anatomical Limits of Ilio-Inguinal Block Dissection
Overview
Ilio-inguinal block dissection (ilioinguinal lymph node dissection, ILND) is a combined superficial inguinal + deep pelvic (iliac) lymphadenectomy. It removes all lymph node-bearing tissue from the femoral triangle below (inguinal component) and the pelvic side-wall nodes above the inguinal ligament (iliac component). It is most commonly performed for:
- Penile carcinoma (primary indication)
- Vulvar carcinoma
- Lower limb melanoma with palpable or proven groin metastases
- Scrotal / anal carcinoma
The operation is conceptually in two parts - inguinal (superficial) and iliac (deep/pelvic) - which together constitute the complete ilioinguinal dissection.
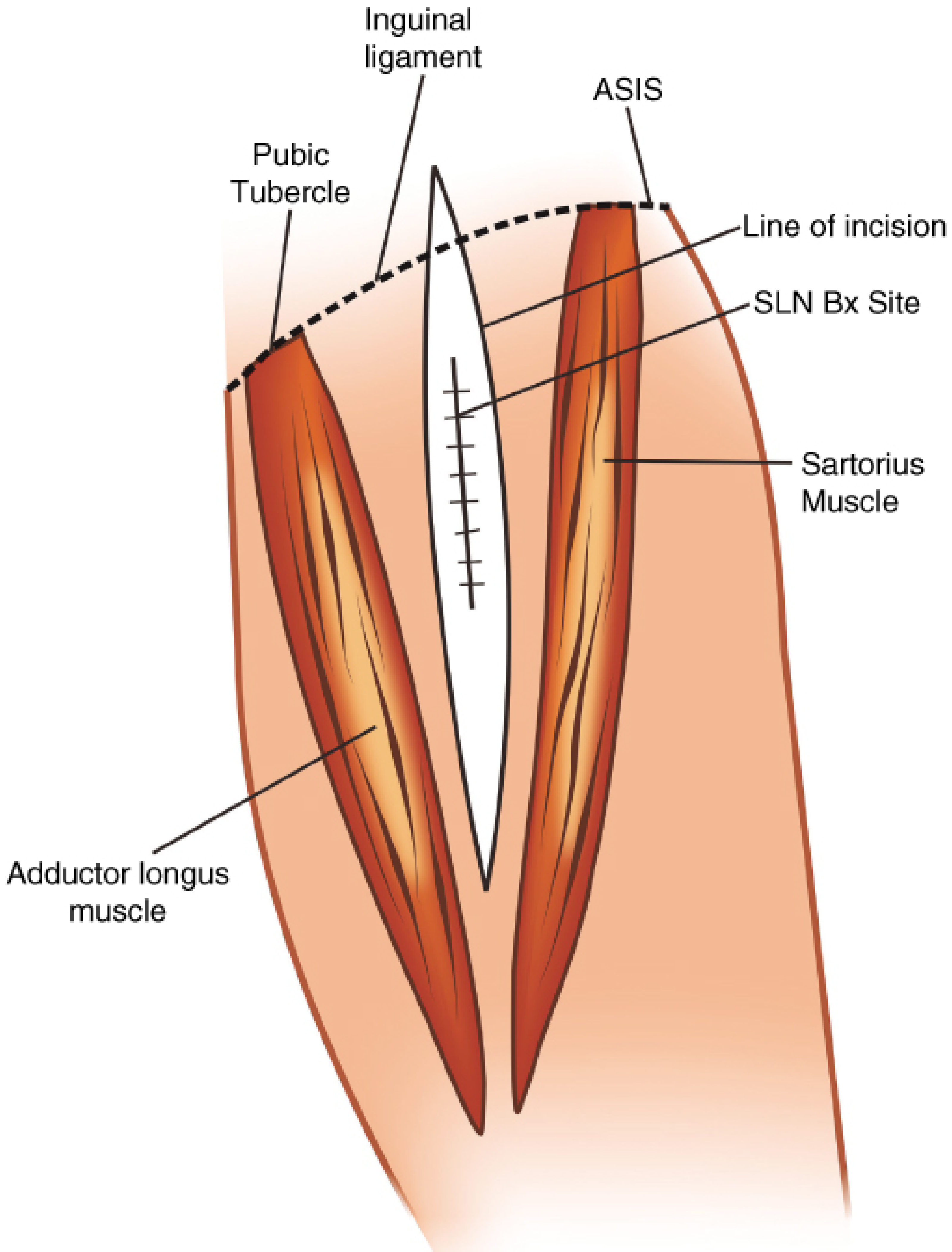
Part 1: Inguinal (Superficial) Component - Limits of the Femoral Triangle
The inguinal dissection removes all lymph-node-bearing fibrofatty tissue within and around the femoral triangle, including both the superficial (above fascia lata) and deep (below fascia lata, around femoral vessels) inguinal nodes.
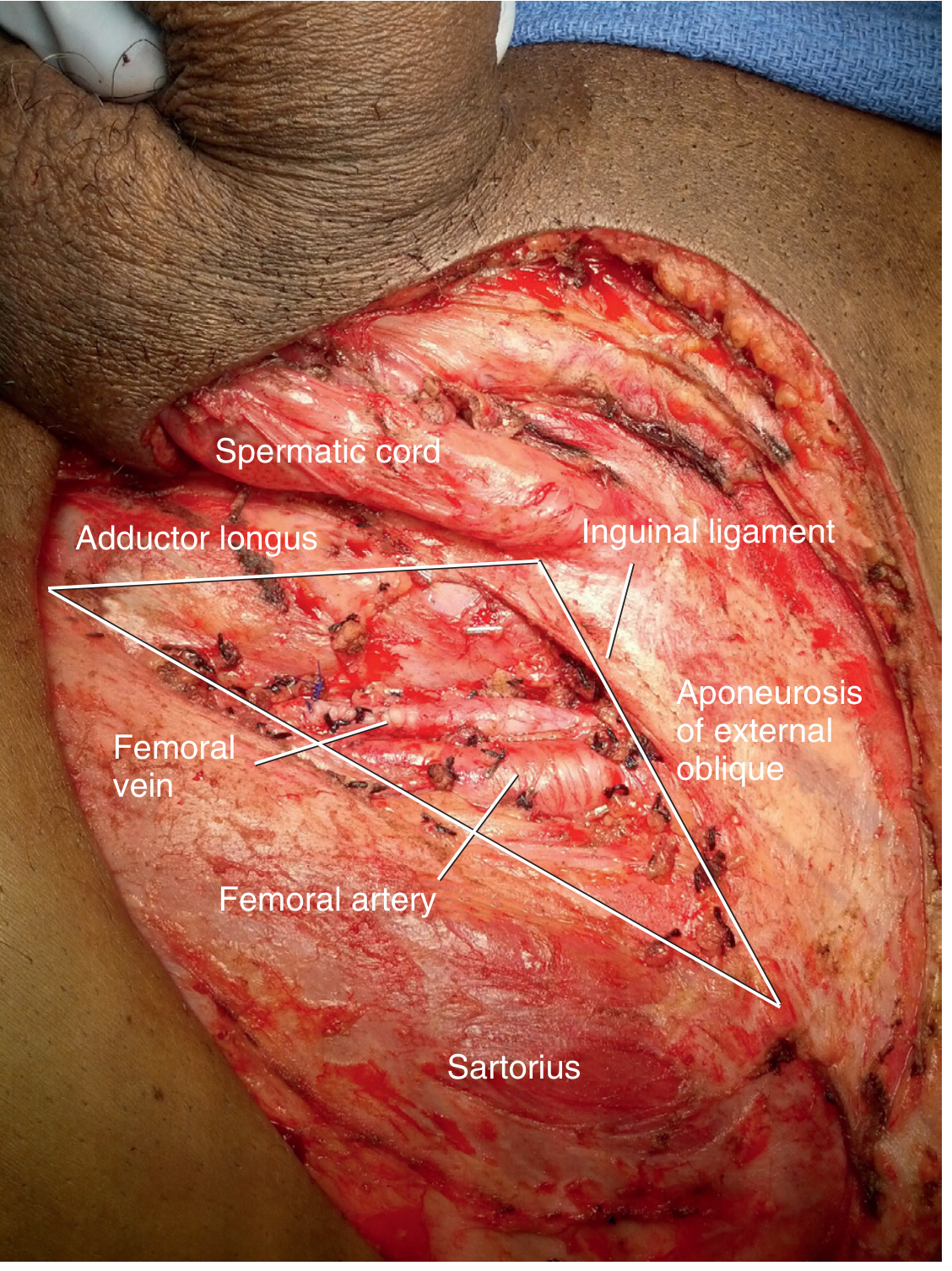
Boundaries of the Femoral Triangle (Inguinal) Dissection
| Boundary | Structure |
|---|---|
| Superior | Inguinal ligament (and aponeurosis of external oblique) |
| Lateral | Medial border / fascia of sartorius muscle |
| Medial | Lateral border / fascia of adductor longus muscle |
| Inferior (apex) | Apex of the femoral triangle (junction of sartorius and adductor longus) |
| Superficial (roof) | Skin and subcutaneous tissue (Scarpa fascia) - raised as a flap |
| Deep (floor) | Fascia lata / femoral sheath enclosing femoral vessels |
The superior extension of tissue removal also includes lymph node-bearing tissue above the inguinal ligament, superficial to the external oblique aponeurosis, within the area bounded by the pubic tubercle medially and the anterior superior iliac spine (ASIS) laterally.
"The femoral triangle defined by the inguinal ligament superiorly, the adductor longus muscle medially, and the sartorius muscle laterally. The femoral nerve, artery, and vein course medial to lateral within the femoral triangle." - Hinman's Atlas of Urologic Surgery
Key Anatomical Diagram
Structures Encountered / Preserved
- Femoral nerve (deep to iliacus fascia) - preserved; motor to quadriceps, sartorius, pectineus; sensory to anterior thigh
- Femoral artery and vein - skeletonised; femoral canal nodes (including Cloquet's node) removed
- Saphenous vein - ligated at saphenofemoral junction in standard dissection (preserved in modified/limited dissection)
- Saphenofemoral junction - the fossa ovalis (saphenous hiatus) is an important landmark
- Lateral femoral cutaneous nerve - at risk along sartorius; injury causes meralgia paraesthetica
- Lymphatic channels - all ligated/clipped to prevent lymphocele
Deep inguinal nodes lie below the fascia lata, medial to the femoral vein - these are removed separately after incising the femoral sheath. The deepest node in the femoral canal is Cloquet's node (node of Rosenmuller), which lies just below the inguinal ligament medial to the femoral vein.
Part 2: Iliac (Deep/Pelvic) Component - Limits of the Pelvic Dissection
The pelvic dissection is performed via a midline suprapubic extraperitoneal approach, removing all nodes from the obturator fossa and along the external and internal iliac vessels.
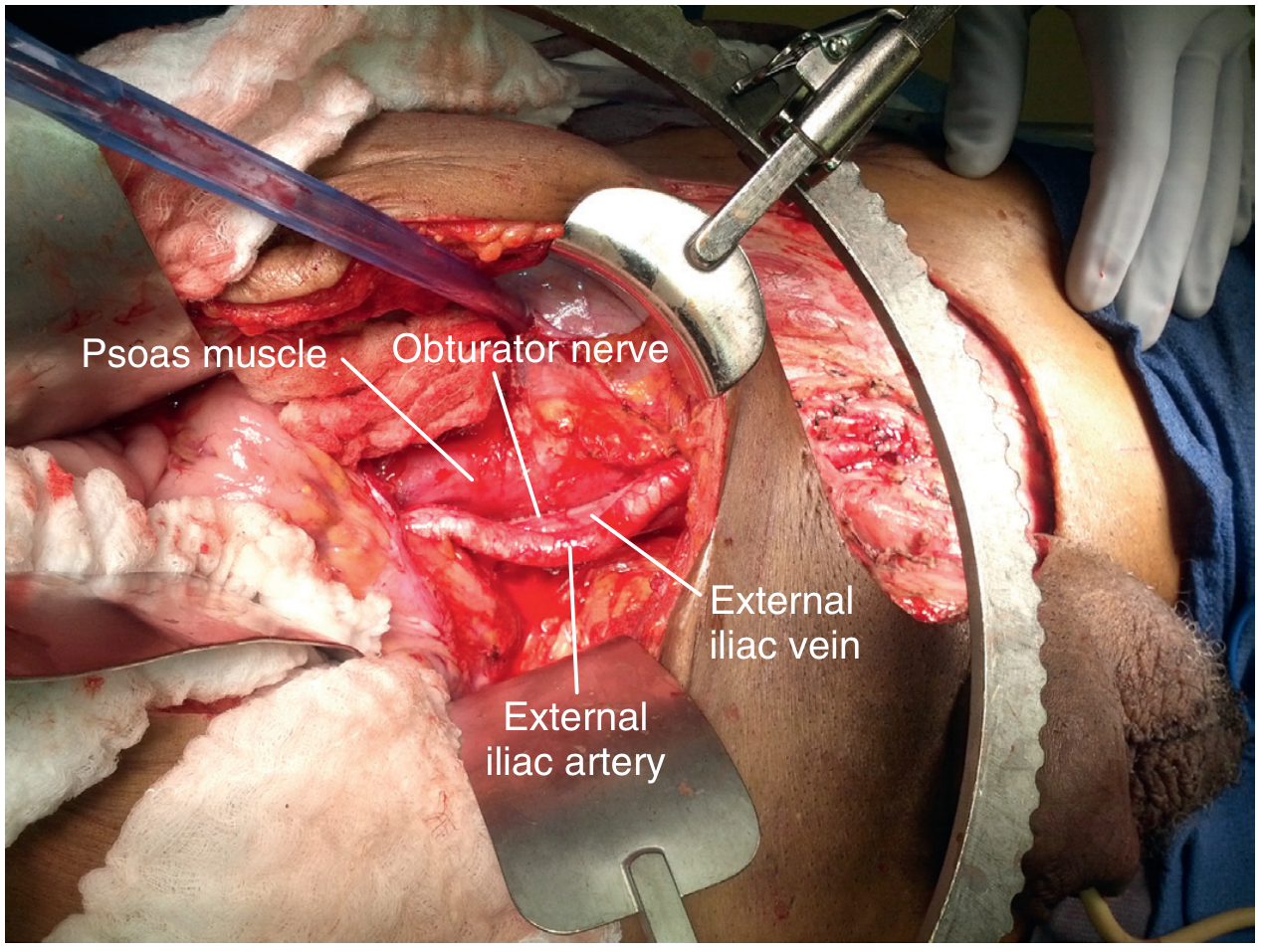
Boundaries of the Pelvic (Iliac) Dissection
| Boundary | Structure |
|---|---|
| Proximal (superior) | Bifurcation of the common iliac vessels |
| Lateral | Ilioinguinal nerve (genitofemoral nerve) / medial border of psoas muscle |
| Medial | Obturator nerve |
| Inferior | Inguinal ligament (where pelvic dissection connects to inguinal dissection) |
| Deep | Obturator foramen / lateral pelvic wall |
Nodal Groups Removed in the Pelvic Component
- External iliac nodes - along the external iliac artery and vein
- Internal iliac (hypogastric) nodes - along the internal iliac vessels
- Obturator nodes - in the obturator fossa, between the external iliac vein and the obturator nerve
"The boundaries of PLND include the bifurcation of the common iliac vessels proximally, the ilioinguinal nerve laterally, and the obturator nerve medially. During PLND, all nodal tissue is removed from the obturator, internal iliac, and external iliac regions." - Hinman's Atlas of Urologic Surgery
Summary: Complete Ilioinguinal Dissection Limits at a Glance
SUPERIOR: Bifurcation of common iliac artery
↕ (pelvic component along external/internal iliac vessels)
SUPERIOR: Inguinal ligament / aponeurosis of external oblique
↕ (inguinal / femoral triangle component)
INFERIOR: Apex of femoral triangle (junction of sartorius + adductor longus)
LATERAL: Sartorius muscle (inguinal) / ilioinguinal nerve (pelvic)
MEDIAL: Adductor longus muscle (inguinal) / obturator nerve (pelvic)
ROOF: Skin flaps raised (Scarpa fascia level)
FLOOR: Fascia lata → femoral sheath → pelvic sidewall
Modified Ilio-Inguinal Dissection (Catalona, 1988)
For clinically node-negative groins with high-risk primary tumours, a modified dissection is used with a smaller template:
- Superomedial quadrant of the inguinal region only (where the majority of positive nodes are found)
- Dissection does not extend lateral to the femoral artery or caudal to the fossa ovalis
- Saphenous vein is preserved (reduces lymphoedema)
- No sartorius transposition required
- Yields equivalent oncological control with significantly lower morbidity
Important Structures Preserved
| Structure | Reason |
|---|---|
| Femoral nerve | Motor (quadriceps, sartorius) + sensory (anterior thigh) |
| Obturator nerve | Motor (adductors); injury causes adductor weakness |
| Great saphenous vein (in modified) | Reduces leg lymphoedema |
| Lateral femoral cutaneous nerve (if possible) | Prevents meralgia paraesthetica |
Sartorius Transposition
After radical ilioinguinal dissection, the sartorius muscle is detached from its origin at the ASIS and rotated medially to cover and protect the skeletonised femoral vessels - protecting against erosion, haemorrhage, and secondary infection, especially if post-operative radiotherapy is planned.
Sources: Hinman's Atlas of Urologic Surgery, 4th Ed; Fischer's Mastery of Surgery, 8th Ed; Campbell Walsh Wein Urology 3-Volume Set; Smith and Tanagho's General Urology, 19th Ed
Briefly describe the causes of fever on post operative day 2 in a 50 year old patient who has been operated for rectal carcinoma. [5]
Finding Sources
Finding Sources
Reading File
Reading File
I have everything needed. This is a 5-mark short answer question - focused, practical, and exam-oriented. Let me deliver a concise, well-structured answer.
Causes of Fever on Post-Operative Day 2 Following Rectal Carcinoma Surgery
Post-operative fever occurring within the first 48 hours is predominantly due to non-infectious, inflammatory (SIRS) causes - a normal physiological response to surgical tissue injury mediated by pro-inflammatory cytokines (IL-1, IL-6, TNF-α). However, infectious causes must be actively excluded, especially in this patient given the contaminated (colorectal) field.
The classic mnemonic is the "5 Ws":
1. Wind - Pulmonary (Most Common)
Atelectasis is the single most common cause of fever in the first 24-48 hours post-operatively.
- Caused by: shallow breathing from pain/opiate analgesia, residual anaesthetic, prolonged recumbency, and abdominal splinting
- Collapse of small airways reduces mucociliary clearance and promotes micro-aspiration
- Features: low-grade fever, reduced breath sounds at lung bases, mild hypoxia
- Treatment: early mobilisation, incentive spirometry, physiotherapy, adequate analgesia
Early pneumonia (hospital-acquired or aspiration) may also begin to manifest by day 2, especially after prolonged anaesthesia or in patients with poor pulmonary reserve.
2. Water - Urinary Tract Infection (UTI)
- Almost all patients after rectal cancer surgery have a urinary catheter in situ - an ascending infection risk from day 1 onwards
- Particularly relevant here as pelvic dissection (APR or anterior resection) may involve close proximity to the bladder, and post-operative urinary retention is common
- Features: dysuria, cloudy urine, pyrexia; confirmed on urine culture
3. Wound / Abdominal Infection
Although full wound infections typically present later (day 4-7), early wound cellulitis or subcutaneous haematoma can begin to manifest at day 2.
More importantly for rectal surgery:
- Anastomotic leak / peritoneal soiling: Early sub-clinical anastomosis disruption with bacterial contamination of the peritoneal cavity can present with fever from day 2. This is a particular concern after anterior resection of the rectum.
- Pelvic haematoma: Blood in the pelvis acts as a culture medium; an infected pelvic haematoma may cause fever early
- Perineal wound (after abdominoperineal resection): The large perineal wound is in direct proximity to the anal canal and perineal flora, making early infection possible
4. Walking - Deep Vein Thrombosis (DVT)
- Rectal cancer surgery is a major operation with a long pelvic dissection, carrying a high thromboembolic risk (cancer, pelvic surgery, immobility = Virchow's triad)
- DVT may produce a low-grade fever from day 2 onwards due to the inflammatory reaction around the thrombus
- Pulmonary embolism (PE) can also present with fever and is a potentially fatal cause
- DVT prophylaxis (LMWH + compression stockings + early mobilisation) is mandatory
5. Wonder Drugs - Drug Fever / Transfusion Reaction
- Drug fever: antibiotics (particularly beta-lactams), anaesthetic agents, or other medications can trigger a hypersensitivity-mediated pyrexia within 24-48 hours
- Blood transfusion reaction: common in major colorectal cancer surgery where blood loss is significant; a febrile non-haemolytic transfusion reaction typically occurs within hours of transfusion but may present up to 48 hours later
- Malignant hyperthermia: rare but important - triggered by volatile anaesthetic agents (halothane, sevoflurane) + succinylcholine; presents intraoperatively or in recovery (not day 2)
Additional Causes Specific to Rectal Cancer Surgery
| Cause | Comment |
|---|---|
| SIRS / surgical cytokine response | Most common overall cause day 0-2; fever is a normal physiological response to tissue trauma |
| Anastomotic leak | Critical concern; any fever + abdominal pain + tachycardia on day 2 should prompt investigation (CT abdomen) |
| Intra-abdominal abscess | Less likely at day 2 but begins to form from collections |
| Acalculous cholecystitis | Seen in major surgery / critical illness; bile stasis from fasting |
| IV line / central catheter sepsis | Any indwelling vascular access device is a source |
Summary Table: Timing of Post-Operative Fever Causes
| Day | Cause |
|---|---|
| 0-2 hrs | Malignant hyperthermia, transfusion reaction |
| Day 1-2 | Atelectasis (Wind), SIRS/inflammatory response |
| Day 2-3 | UTI, DVT, drug fever |
| Day 4-5 | Wound infection, anastomotic leak |
| Day 5-7 | Pneumonia, abscess, line sepsis |
"Immediate postoperative fever occurring within the first 48 hours after surgery is most likely due to proinflammatory mediators causing SIRS. A fever that develops 72 hours or more after surgery is more likely to be due to infection." - Sabiston Textbook of Surgery
Sources: Sabiston Textbook of Surgery; Tintinalli's Emergency Medicine
Discuss the various measures to be taken while operating on a patient with haemophilia A. [5]
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
I have excellent material from Sabiston, Miller's Anaesthesia, and Cummings. I now have all necessary information for a well-structured 5-mark answer.
Measures While Operating on a Patient with Haemophilia A
Brief Background
Haemophilia A is an X-linked recessive disorder caused by a deficiency of Factor VIII (anti-haemophilic factor). Severity is classified by residual Factor VIII activity:
- Mild: Factor VIII >5% (5-40 IU/dL)
- Moderate: 1-5%
- Severe: <1%
Laboratory findings: prolonged aPTT with normal PT, normal bleeding time, and normal platelet count.
Operating on such a patient requires meticulous pre-operative, intra-operative, and post-operative planning, ideally with a multidisciplinary team (surgeon, haematologist, anaesthetist).
I. Pre-Operative Measures
1. Multidisciplinary Planning
- Elective surgery should only proceed after thorough coordination between the surgeon, haematologist, and anaesthetist
- Ensure availability of all laboratory and therapeutic resources before, during, and after surgery
- Avoid elective surgery if possible until haemostasis is optimised
2. Inhibitor Screening
- Up to 25% of patients with severe Haemophilia A develop inhibitory alloantibodies against Factor VIII after repeated exposure
- Pre-operative inhibitor screen should be performed at least one week before surgery
- If inhibitors are present, standard Factor VIII replacement will be ineffective - alternative agents are required (see below)
3. Assessment of Severity and Treatment Planning
- Measure baseline Factor VIII level
- Target Factor VIII level for major surgery: 80-100% of normal (>1 IU/mL)
- For minor surgery: 50-80% may suffice
4. Factor VIII Replacement (Core Measure)
| Disease Severity | Pre-operative Treatment |
|---|---|
| Mild (Factor VIII >5%) | DDAVP (Desmopressin) 0.3 mcg/kg IV/SC, given 90 minutes before surgery. Raises Factor VIII up to 5-fold. Redose daily or twice daily as needed. Monitor for hyponatraemia. |
| Moderate/Severe | Factor VIII concentrate (recombinant or plasma-derived), administered 10-20 minutes before incision |
| Inhibitor-positive | Bypass agents: recombinant activated Factor VIIa (rFVIIa / NovoSeven) or activated Prothrombin Complex Concentrate (FEIBA). Porcine Factor VIII is an alternative. |
Formula for Factor VIII dosing:
Units required = Body weight (kg) × Desired rise in Factor VIII (%) × 0.5
Factor VIII has a half-life of 8-12 hours, so dosing is repeated every 8-12 hours to maintain therapeutic levels.
5. Avoid Drugs that Impair Haemostasis
- Strictly avoid aspirin and NSAIDs (inhibit platelet aggregation, worsen bleeding)
- Avoid intramuscular injections
- Regional anaesthesia (e.g. epidural, spinal) should be used with extreme caution and only after adequate Factor VIII cover
II. Intra-Operative Measures
6. Anaesthesia
- General anaesthesia is preferred in most cases
- Regional blocks are relatively contraindicated due to risk of haematoma formation in deep tissues
- Endotracheal intubation should be atraumatic (risk of pharyngeal/laryngeal haematoma)
7. Surgical Technique
- Meticulous haemostasis at every step - careful ligation of every bleeding point
- Use of diathermy (electrocautery) liberally to control small vessel bleeding
- Avoid unnecessary dissection; work in dry surgical field
- Use of haemostatic agents: topical thrombin, oxidised cellulose (Surgicel), or fibrin glue at the operative site
- Minimise dead space to prevent haematoma formation
8. Intra-operative Factor VIII Monitoring
- Serial Factor VIII level monitoring intra-operatively during prolonged procedures
- Maintain Factor VIII levels >80% throughout the operation
- Multiple IV access lines should be available - keep sampling line separate from infusion line for accurate monitoring
9. Blood Products Availability
- Cross-matched blood, fresh frozen plasma (FFP), and cryoprecipitate should be immediately available in the operating theatre
- Cryoprecipitate is rich in Factor VIII (80-100 units/bag), vWF, fibrinogen, and Factor XIII - useful as adjunct when Factor VIII concentrate is unavailable
III. Post-Operative Measures
10. Continued Factor VIII Replacement
- Factor VIII levels must be maintained post-operatively:
- First 3 days: maintain >80%
- Days 4-7: maintain >50%
- Days 7-14: maintain >30-50%
- Factor VIII infused every 8-12 hours (half-life) or as a continuous infusion
11. Post-operative Analgesia
- Avoid NSAIDs and aspirin for pain relief
- Use paracetamol or opioids as appropriate
- Tranexamic acid (antifibrinolytic) may be given perioperatively to stabilise clot formation, especially for oral/dental or mucosal surgery
12. Monitoring and Early Detection of Bleeding
- Regular clinical assessment for signs of haematoma or internal bleeding
- Drain output monitoring
- Repeated coagulation tests and Factor VIII levels
- Prompt re-exploration if unexpected bleeding occurs
Summary Framework (Mnemonic: PRE - INTRA - POST)
| Phase | Key Measures |
|---|---|
| Pre-op | MDT planning, inhibitor screen, Factor VIII assay, DDAVP (mild) or Factor VIII concentrate (severe), avoid NSAIDs |
| Intra-op | GA preferred, meticulous haemostasis, diathermy, haemostatic agents, Factor VIII monitoring, cryoprecipitate available |
| Post-op | Continue Factor VIII replacement (taper over 14 days), tranexamic acid, no NSAIDs, monitor for bleeding |
"Preoperative treatment for hemophilia A depends on disease severity. Severe phenotypes should be treated with administration of factor concentrates in the immediate preoperative setting, within 10 to 20 minutes of incision. Reducing the need for repeat dosing of factor concentrates minimizes the likelihood of inhibitor development." - Sabiston Textbook of Surgery
Sources: Sabiston Textbook of Surgery; Miller's Anaesthesia, 10th Ed; Cummings Otolaryngology, 7th Ed
What are the anesthetic issues during laparoscopic surgery? [5]
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have comprehensive, authoritative content. Let me compile the complete answer.
Anaesthetic Issues During Laparoscopic Surgery
Overview
Laparoscopic surgery creates a unique physiological environment that differs fundamentally from open surgery. The anaesthetist must manage the combined effects of:
- CO₂ pneumoperitoneum (elevated intra-abdominal pressure + CO₂ absorption)
- Patient positioning (Trendelenburg, reverse Trendelenburg)
- General anaesthesia in the context of these derangements
"Proper anaesthesia management during laparoscopic surgery requires a thorough knowledge of the pathophysiology of the CO₂ pneumoperitoneum." - Schwartz's Principles of Surgery, 11th Ed
I. Cardiovascular Effects
CO₂ insufflation raises intra-abdominal pressure (IAP) to 12-15 mmHg, producing complex cardiovascular consequences:
Mechanical Effects
- Compression of the inferior vena cava (IVC) → decreased venous return → reduced cardiac filling and preload
- Compression of the aorta → increased systemic vascular resistance (SVR)
- In hypovolaemic patients, IVC compression can cause severe reduction in venous return and cardiac output
Neurohumoral Effects
- Peritoneal stretch activates the sympathetic nervous system → catecholamine release + activation of renin-angiotensin-aldosterone system + vasopressin release
- Results in: ↑ MAP, ↑ SVR, ↑ left ventricular afterload → increased myocardial work
- Net effect: ↑ heart rate, ↑ blood pressure, ↑ SVR - this combination can provoke myocardial ischaemia in patients with pre-existing coronary artery disease
Position-Related Cardiovascular Effects
| Position | Cardiovascular Effect |
|---|---|
| Trendelenburg (head down) | ↑ venous return, ↑ preload, ↑ cardiac output (beneficial) |
| Reverse Trendelenburg (head up) | ↑ SVR, ↓ venous return, ↓ cardiac output |
Arrhythmias
- Vagal stimulation from peritoneal stretch can cause bradycardia, especially during rapid initial insufflation
- Hypercapnia (from CO₂ absorption) sensitises the myocardium → risk of ventricular arrhythmias
- Carbon dioxide gas embolism (rare but catastrophic) - causes sudden severe hypotension, raised CVP, "mill-wheel" murmur, and cardiac arrest
II. Respiratory / Pulmonary Effects
Mechanical
- Cephalad displacement of the diaphragm by elevated IAP → reduced functional residual capacity (FRC), atelectasis, increased airway resistance
- Decreased lung compliance → higher ventilatory pressures required
- V/Q mismatch → increased alveolar-arterial oxygen gradient → potential hypoxia
- Risk of endobronchial intubation - diaphragm pushed up may shift the carina, advancing an ETT into a main bronchus
CO₂ Absorption
- CO₂ is absorbed rapidly from the peritoneal cavity into the bloodstream
- Causes hypercapnia (↑ PaCO₂) and respiratory acidosis
- Must be managed by increasing minute ventilation (↑ respiratory rate or tidal volume)
- In patients with severe COPD or limited respiratory reserve, CO₂ may not be adequately cleared → may require conversion to open surgery or use of helium as an insufflant
Subcutaneous / Extra-peritoneal CO₂
- Insufflation into extraperitoneal tissue planes causes surgical emphysema → CO₂ tracks into the mediastinum, neck, and face
- Causes marked hypercapnia that cannot be corrected by increased ventilation alone
III. Anaesthetic Technique
Choice of Anaesthesia
- General endotracheal anaesthesia (GETA) with controlled mechanical ventilation is mandatory for all laparoscopic procedures
- Reasons: pneumoperitoneum restricts diaphragmatic movement; extreme positioning; prolonged procedures; cardiopulmonary derangements make spontaneous ventilation unsafe
- Regional anaesthesia is only occasionally suitable for very brief, minimal procedures
Airway Management
- Endotracheal intubation with controlled ventilation is essential
- Muscle relaxation is mandatory - prevents straining, allows adequate IAP, reduces risk of diaphragmatic injury
- Ventilator settings adjusted to increase minute ventilation to compensate for CO₂ absorption and maintain normocapnia (ETCO₂ 35-40 mmHg)
Anaesthetic Agents
- Short-acting agents preferred (desflurane, sevoflurane) - most laparoscopic procedures are day-case operations
- Propofol TIVA is an excellent choice - antiemetic properties help prevent post-operative nausea and vomiting (PONV), a major problem after laparoscopy
- Nitrous oxide (N₂O): controversial - may cause bowel distension (diffuses into gut lumen); increases PONV risk; accumulates in the peritoneal cavity and may support combustion; best avoided
IV. Monitoring Requirements
| Monitor | Importance |
|---|---|
| End-tidal CO₂ (capnography) | Mandatory - tracks CO₂ absorption and adequacy of ventilation |
| ECG (continuous) | Detects arrhythmias, ischaemia |
| SpO₂ (pulse oximetry) | Detects hypoxia |
| Non-invasive BP | Cardiovascular monitoring |
| Temperature | Prolonged laparoscopy can cause hypothermia |
| Airway pressure | Detects rise from pneumoperitoneum or endobronchial intubation |
| Neuromuscular monitoring | Confirms adequate relaxation |
| Invasive arterial line (if cardiac disease) | Beat-to-beat BP monitoring during high-risk cases |
V. Positioning-Related Issues
- Trendelenburg: used for pelvic/lower GI surgery - increases intracranial pressure (ICP), intraocular pressure (IOP); risk of brachial plexus injury from shoulder braces; facial/airway oedema in prolonged cases
- Reverse Trendelenburg: used for upper GI/cholecystectomy - reduces venous return; risk of VAE
- Rare but serious: cases of postoperative blindness (ischaemic optic neuropathy) reported after prolonged steep Trendelenburg, especially with preexisting glaucoma, diabetes, or atherosclerosis
VI. Renal Effects
- Pneumoperitoneum reduces renal perfusion by compressing renal vasculature and raising venous pressure
- Oliguria is common during laparoscopy - anaesthetist should not automatically over-replace fluids assuming large insensible losses (as in open surgery)
- Insensible fluid losses during laparoscopy are negligible - IV fluid administration should be conservative and targeted to maintaining circulating volume
VII. Post-Operative Nausea and Vomiting (PONV)
- One of the most common complications after laparoscopic surgery and a major cause of unexpected admission after day-case laparoscopy
- Caused by: peritoneal gas insufflation, opioids, patient positioning, N₂O use
- Prevention: ondansetron + dexamethasone (dual antiemetic prophylaxis), propofol TIVA, avoiding N₂O, minimising opioids
- Nonnarcotic analgesics (e.g. ketorolac/NSAIDs when haemostasis is secured) should be used to reduce opioid requirements
VIII. DVT / Thromboembolism
- Elevated IAP compresses iliac veins and impedes venous return from the lower limbs → venous stasis
- Trendelenburg position further exaggerates this
- Sequential compression devices applied before induction; pharmacological DVT prophylaxis (LMWH) peri-operatively
Summary of Key Anaesthetic Issues
| System | Issue |
|---|---|
| Cardiovascular | ↑ SVR, ↑ BP, ↓ venous return, arrhythmias, gas embolism |
| Respiratory | ↓ FRC, ↑ airway pressure, hypercapnia, V/Q mismatch |
| Anaesthetic technique | GETA mandatory; muscle relaxation; short-acting agents |
| Monitoring | Capnography essential; invasive monitoring if comorbidities |
| Positioning | ICP/IOP effects; nerve injury; optic neuropathy |
| Renal | Oliguria; conservative fluid management |
| Post-op | PONV - dual antiemetic prophylaxis essential |
| Thrombosis | DVT prophylaxis from time of induction |
Sources: Barash, Cullen & Stoelting's Clinical Anaesthesia, 9th Ed; Schwartz's Principles of Surgery, 11th Ed; Hinman's Atlas of Urologic Surgery, 4th Ed
Prophylaxis for DVT. [5]
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Excellent - I have comprehensive, authoritative content from Sabiston (Caprini score table), Campbell Walsh (ACCP risk table), and Schwartz's. I can now write a focused 5-mark answer.
Prophylaxis for Deep Vein Thrombosis (DVT)
Rationale
DVT and its life-threatening complication - pulmonary embolism (PE) - are among the most preventable causes of hospital mortality. Together they constitute venous thromboembolism (VTE). Risk is greatest after major abdominal surgery, orthopaedic procedures, and in patients with malignancy, immobility, or prior VTE.
The triad of Virchow (venous stasis + endothelial injury + hypercoagulability) underpins all DVT prophylaxis strategies.
Step 1: Risk Stratification - Caprini Score
Before initiating prophylaxis, every surgical patient should be risk-stratified using the Caprini Risk Assessment Model:
| Points | Risk Factors |
|---|---|
| 1 point each | Age 41-60, minor surgery, obesity (BMI >25), varicose veins, OCP/HRT, pregnancy/postpartum, immobility, acute MI, COPD |
| 2 points each | Age 61-74, major surgery >45 min, laparoscopy >45 min, central venous access, malignancy, immobility >72 hrs |
| 3 points each | Age ≥75, history of DVT/PE, family history of thrombosis, Factor V Leiden, antiphospholipid antibodies, elevated homocysteine |
| 5 points each | Elective major lower limb arthroplasty, pelvic/hip fracture, stroke, spinal cord injury, multiple trauma |
Recommended prophylaxis by score:
| Caprini Score | Risk | Management |
|---|---|---|
| 0-4 | Low-moderate | Early ambulation |
| 5-8 | High | Early ambulation + IPC + 7-10 days anticoagulation |
| >9 | Highest | IPC + 30 days anticoagulation |
Prophylactic Measures
A. Non-Pharmacological (Mechanical) Methods
1. Early Ambulation
- The single most important and simplest measure
- Begin within hours of surgery once patient is stable
- Activates the calf muscle pump, the primary mechanism of venous return in the legs
- Suitable for all risk levels; insufficient alone for moderate-high risk
2. Graduated Compression Stockings (GCS / TED Stockings)
- Provide 15-40 mmHg graduated pressure from ankle to thigh
- Reduce venous pooling and stasis in lower limb superficial and deep veins
- Applied pre-operatively, worn throughout hospital stay
- Contraindicated in: peripheral arterial disease (ABPI <0.8), severe leg oedema, active skin infection
- Effective as adjunct in low-risk patients; inadequate alone for high-risk
3. Intermittent Pneumatic Compression (IPC) / Sequential Compression Devices (SCD)
- Pneumatic cuffs applied to calves (and sometimes thighs), inflating sequentially from ankle upward
- Simulate the calf muscle pump; also stimulate release of endogenous fibrinolytic factors (tissue plasminogen activator)
- Applied before induction of anaesthesia and continued intra-operatively and post-operatively
- Highly effective; particularly valuable when pharmacological prophylaxis is contraindicated (active bleeding, neurosurgery, recent surgery)
- The preferred mechanical method in high-risk cases where anticoagulation is risky
4. Foot Pumps / Venous Foot Pumps
- Compress the plantar venous plexus, augmenting venous return
- Alternative when leg SCDs cannot be used (e.g. leg fractures)
B. Pharmacological Methods
1. Low-Dose Unfractionated Heparin (LDUH)
- 5,000 units SC every 8-12 hours
- Enhances antithrombin III activity; inhibits Factor Xa and thrombin
- Start 2 hours pre-operatively (or immediately post-operatively in bleeding-risk cases)
- Advantages: cheap, reversible with protamine, no dose adjustment for renal impairment
- Disadvantages: risk of Heparin-Induced Thrombocytopenia (HIT), requires twice/thrice daily injection, less efficacious in orthopaedic surgery
2. Low Molecular Weight Heparin (LMWH) - Preferred Agent
- e.g., enoxaparin 40 mg SC once daily (20 mg once daily if CrCl <30 mL/min)
- Selectively inhibits Factor Xa (greater Xa:IIa ratio than UFH)
- Advantages: once-daily dosing, more predictable response, lower risk of HIT, no routine monitoring required
- Start 10-12 hours before surgery or 6-12 hours after surgery
- Continue for 7-10 days (general surgery) or 28-35 days (major orthopaedic surgery, cancer surgery)
- Contraindicated in severe renal failure (accumulates); requires dose reduction for CrCl <30 mL/min
3. Fondaparinux
- Synthetic pentasaccharide; selective Factor Xa inhibitor
- 2.5 mg SC once daily, started 6-8 hours post-operatively
- Licensed for orthopaedic and general surgical prophylaxis
- Advantage: no risk of HIT (does not bind platelet factor 4)
- Disadvantage: longer half-life; no reversal agent; avoided in renal impairment
4. Direct Oral Anticoagulants (DOACs)
- Rivaroxaban (Factor Xa inhibitor), Dabigatran (direct thrombin inhibitor), Apixaban (Factor Xa inhibitor)
- Approved primarily for orthopaedic surgery (hip and knee replacement) prophylaxis
- Oral administration; predictable pharmacokinetics; no routine monitoring
- Reversal agents now available (andexanet alfa for Xa inhibitors; idarucizumab for dabigatran)
5. Aspirin
- 160 mg as sole agent is an alternative only when LMWH and fondaparinux are contraindicated
- Inhibits platelet aggregation (TXA₂ pathway)
- Inferior to LMWH; not recommended as first-line for surgical VTE prophylaxis
- Used adjunctively after hip/knee arthroplasty in selected lower-risk patients
6. Warfarin / Vitamin K Antagonists
- Mainly used for extended post-discharge prophylaxis or in orthopaedic surgery
- Target INR 2.0-3.0
- Disadvantage: narrow therapeutic window, requires INR monitoring, multiple drug interactions, slow onset
C. Inferior Vena Cava (IVC) Filter
- Indicated when: anticoagulation is absolutely contraindicated (e.g. active major haemorrhage) and DVT/PE risk is very high
- Retrievable filters preferred - removed once anticoagulation can be resumed
- Prevents PE but does not prevent DVT; may increase long-term risk of DVT
Risk-Stratified Prophylaxis (ACCP Guidelines)
| VTE Risk | Prophylaxis |
|---|---|
| Very low | Early ambulation only |
| Low | Mechanical (IPC or GCS) |
| Moderate | LMWH or LDUH, or IPC |
| High | LMWH or LDUH plus IPC |
| High-risk cancer surgery | LMWH + IPC + extended post-discharge LMWH (28 days) |
Duration of Prophylaxis
| Setting | Duration |
|---|---|
| General surgery, low-moderate risk | Until fully mobile or discharged |
| Major abdominal/pelvic surgery | 7-10 days |
| Cancer surgery | Extended: 28-35 days post-op |
| Hip/knee replacement | 28-35 days |
Summary
"Options for DVT prophylaxis include intermittent pneumatic compression, use of graduated compression stockings, and administration of low-dose unfractionated heparin, low molecular weight heparin, fondaparinux, and vitamin K antagonists. Prophylaxis should be stratified based on the patient's level of risk." - Schwartz's Principles of Surgery, 11th Ed
The optimal strategy combines mechanical + pharmacological measures in moderate-to-high risk patients, with risk stratification (Caprini score) guiding intensity and duration.
Sources: Sabiston Textbook of Surgery; Schwartz's Principles of Surgery, 11th Ed; Campbell Walsh Wein Urology 3-Volume Set
This is a shared conversation. Sign in to Orris to start your own chat.