Myasthenia gravis
Reading File
Finding Sources
Searching PubMed
"myasthenia gravis"[MeSH Terms] AND treatment
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have very rich data from multiple authoritative sources. Let me compile the comprehensive answer.
Myasthenia Gravis (MG)
Definition
Acquired myasthenia gravis is the most common primary disorder of neuromuscular transmission (NMT). Autoantibodies bind to proteins at the neuromuscular junction (NMJ) - most commonly the acetylcholine receptor (AChR) - disrupting normal neuromuscular transmission and producing characteristic fatigable muscle weakness.
- Bradley and Daroff's Neurology in Clinical Practice
- Goldman-Cecil Medicine
Pathophysiology
The NMJ has no blood-nerve barrier, making it uniquely vulnerable to autoimmune attack by circulating factors.
Three main antibody targets:
| Antibody | % of MG | Mechanism |
|---|---|---|
| Anti-AChR (IgG1/IgG3) | ~85% of generalized MG | Complement activation → destruction of post-junctional membrane; cross-linking + internalization of AChRs; direct blockade of ACh binding |
| Anti-MuSK (IgG4) | Up to 50% of AChR-negative GMG | Inhibits signaling that concentrates AChRs on the postsynaptic surface |
| Anti-LRP4 | Small subset | Interferes with agrin-MuSK signaling, disrupting NMJ integrity |
Other putative targets include agrin and cortactin.
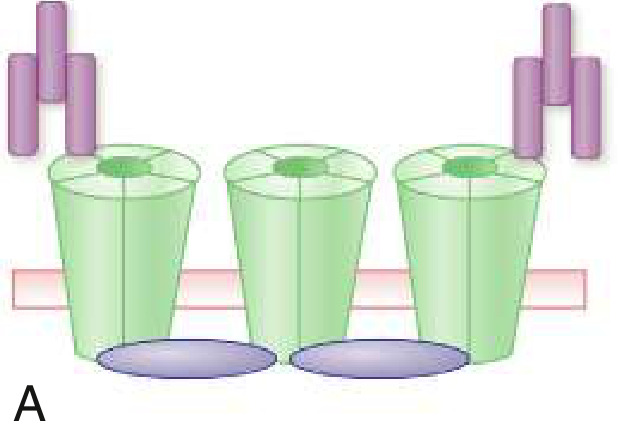
The diagram below shows antibody-mediated AChR cross-linking and removal:
Role of the thymus:
-
In early-onset MG, thymic hyperplasia with germinal centers suggests immune tolerance breakdown initiated in the thymus
-
In thymoma-associated MG, deficiency of the AIRE protein leads to reduced regulatory T cells and increased autoreactivity
-
Thymoma is found in ~10-15% of MG patients
-
Goldman-Cecil Medicine, p. 4111
Epidemiology
-
US prevalence: ~20/100,000 (~60,000 patients total)
-
Prevalence has increased over 50 years due to better ascertainment, reduced mortality, and an aging population
-
Before age 40: women affected ~3x more often than men
-
After age 50: incidence is higher in males; majority of US MG patients are now over 50
-
Genetic predisposition: ~5% of patients have an affected family member; heritability index ~0.65
-
Bradley and Daroff's Neurology, p. 2770
Clinical Subtypes
| Subtype | Key Features |
|---|---|
| Ocular MG (OMG) | Weakness confined to extraocular muscles; 10-15% of Caucasians, up to 58% in Asians; if no generalization by 2 years, 90% chance it stays ocular |
| Generalized MG - Early onset (EOMG) | Age <50, predominantly female, AChR-ab+, thymic hyperplasia, HLA-A1/B8/DRw3 |
| Generalized MG - Late onset (LOMG) | Age >50, predominantly male, may have anti-titin and anti-ryanodine receptor antibodies, atrophic thymus |
| Thymomatous MG | Equal sex ratio, peaks at age 50, striated muscle antibodies common |
| MuSK MG | Predominantly female, cranial/bulbar predominance with muscle atrophy, proximal limb and respiratory involvement; often ChEI-resistant |
| Seronegative MG | No detectable autoantibodies by standard testing |
Clinical Presentation
Weakness that worsens with activity and improves with rest is the hallmark.
Initial symptoms:
- Ptosis or diplopia: ~two-thirds of patients (nearly all develop both within 2 years)
- Difficulty chewing, swallowing, or speaking: ~one-sixth
- Limb weakness: ~10%
Ocular features: Ptosis, ophthalmoplegia, and diplopia from fatigable weakness of periocular muscles - asymmetric and variable.
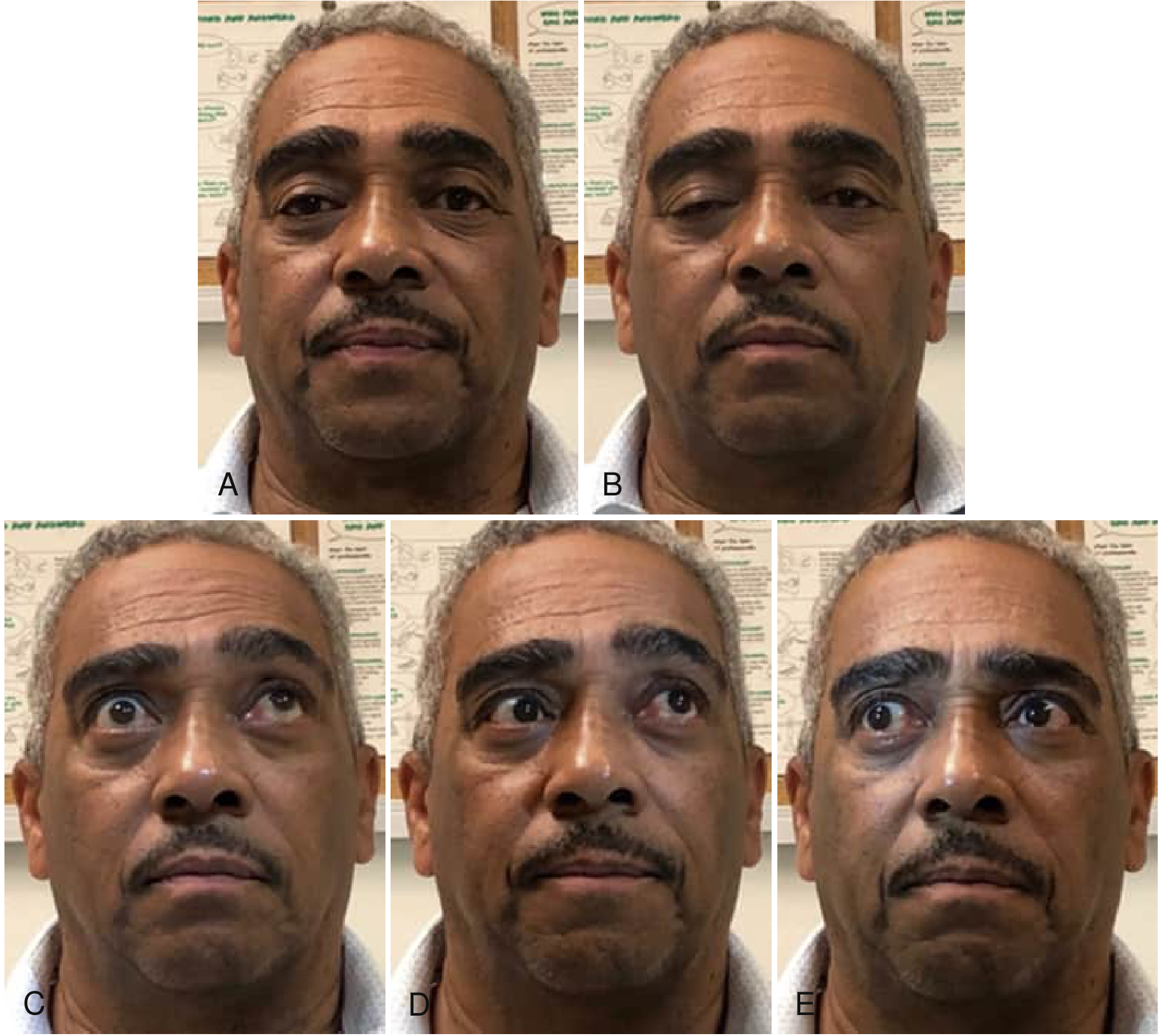
Fig: Progressive right lid ptosis during sustained gaze (A-B), incomplete superior movement both eyes (C), skew deviation on left gaze (D), and incomplete movement on right gaze (E).
Pattern of fatigue: Symptoms are typically worst in the evening, worsen with prolonged muscle use, and may be minimal in the morning.
Bulbar involvement:
- Dysphagia occurs at oral, pharyngeal, and esophageal levels
- Silent aspiration in ≥35% of MG patients with dysphagia
- Dysarthria ("nasal voice") and difficulty chewing
- Dysphagia is a major precipitant of myasthenic crisis in ~56% of cases
Respiratory weakness can lead to myasthenic crisis - respiratory failure requiring mechanical ventilation.
Diagnosis
Serological Testing
- Anti-AChR antibodies (binding, blocking, modulating): Positive in ~85% generalized MG; establishes diagnosis when elevated
- Anti-MuSK antibodies: Test in AChR-ab-negative patients
- Anti-LRP4 antibodies: Considered in double-seronegative patients
Electrodiagnostic Testing
- Repetitive nerve stimulation (RNS): Decremental response ≥10% at low frequencies (2-3 Hz) - characteristic but not always positive, especially in OMG
- Single-fiber EMG (SFEMG): Most sensitive test; shows increased jitter and impulse blocking; required when RNS and antibodies are negative (particularly in OMG)
Pharmacological Testing
- Edrophonium (Tensilon) test: Short-acting ChEI; brief improvement in ptosis/ophthalmoplegia confirms diagnosis. Requires monitoring (risk of bradycardia/cholinergic crisis)
- Ice pack test: Application of ice to ptotic eyelid - improvement suggests MG (cold reversibly improves NMT)
Imaging
-
CT chest (with contrast): Mandatory in all MG patients to screen for thymoma
-
Wills Eye Manual; Bradley and Daroff's Neurology
Treatment
Treatment is layered based on acuity and severity.
1. Symptomatic Therapy
Pyridostigmine (Mestinon) - acetylcholinesterase inhibitor; first-line symptomatic treatment
- Prevents ACh breakdown, increasing available transmitter at the NMJ
- Dose: typically 30-60 mg PO every 4-6 hours
- Note: Often less effective or even worsening in MuSK-MG
2. Immunosuppressive Therapy
| Agent | Role |
|---|---|
| Prednisone | First-line long-term immunosuppression; initial worsening possible |
| Azathioprine | Steroid-sparing agent; onset takes 12-18 months |
| Mycophenolate mofetil | Alternative steroid-sparing agent |
| Cyclosporine / Tacrolimus | Second-line options |
| Rituximab | Particularly effective in MuSK-MG; now supported by a 2025 Cochrane systematic review |
| Methotrexate | Alternative in refractory cases |
3. Rapid Short-Term Therapies (for crisis or pre-operatively)
- Plasmapheresis (PLEX): Rapidly removes circulating antibodies; effect lasts 4-6 weeks
- Intravenous immunoglobulin (IVIg): Comparable efficacy to PLEX; mechanism includes Fc receptor saturation and immune modulation
4. Novel Biologics (FDA-Approved)
Recent years have seen approval of targeted therapies that dramatically expand options for generalized refractory MG:
Complement Inhibitors (C5 blockade):
- Eculizumab (anti-C5 monoclonal Ab, IV q2 weeks) - AChR-ab+ GMG
- Ravulizumab (long-acting anti-C5, IV q8 weeks) - AChR-ab+ GMG
- Zilucoplan (synthetic peptide targeting C5, SC daily) - AChR-ab+ GMG
- All require meningococcal vaccination
FcRn Inhibitors (reduce IgG antibody levels):
- Efgartigimod (IV or SC, weekly x4 cycles) - generalized MG
- Rozanolixizumab - SC, approved for GMG
A 2025 network meta-analysis comparing these novel biologics confirmed meaningful superiority over placebo for multiple outcomes. A 2024 network meta-analysis also evaluated the risk-benefit profile across agents.
- Harrison's Principles of Internal Medicine 22E (2025)
5. Thymectomy
- Recommended for all thymoma patients (does not cure MG but removes tumor)
- Beneficial in non-thymomatous AChR-ab+ patients aged 18-60 (MGTX trial showed improved outcomes vs. prednisone alone at 3 years)
- Less clear benefit in late-onset, MuSK-MG, or seronegative MG
Myasthenic Crisis
A life-threatening emergency involving respiratory failure from severe diaphragmatic and accessory muscle weakness.
Precipitants: Infection, surgery, aspiration, certain medications (aminoglycosides, fluoroquinolones, magnesium, beta-blockers, neuromuscular blocking agents), or rapid tapering of immunotherapy.
Management:
- Secure airway (early intubation threshold is low)
- Hold pyridostigmine (can increase secretions)
- PLEX or IVIg as primary immune therapy
- ICU monitoring
Key Drugs to Avoid in MG
- Aminoglycoside antibiotics
- Fluoroquinolones
- Magnesium sulfate
- Beta-blockers (systemic)
- Neuromuscular blocking agents (depolarizing and non-depolarizing)
- D-penicillamine (can induce MG)
Summary Table
| Feature | Detail |
|---|---|
| Pathogenesis | Autoantibodies to AChR, MuSK, or LRP4 at NMJ |
| Hallmark symptom | Fatigable weakness, worse with activity, better with rest |
| Most common initial symptom | Ptosis/diplopia (~67%) |
| Key diagnostic test | Anti-AChR antibody; SFEMG most sensitive |
| First-line symptomatic Rx | Pyridostigmine |
| First-line immunosuppression | Prednisone ± azathioprine |
| Crisis Rx | PLEX or IVIg + ICU support |
| Emerging therapies | Complement inhibitors (eculizumab, ravulizumab, zilucoplan); FcRn inhibitors (efgartigimod, rozanolixizumab) |
Sources: Bradley and Daroff's Neurology in Clinical Practice; Goldman-Cecil Medicine; Harrison's Principles of Internal Medicine 22E (2025); Ganong's Review of Medical Physiology; Cochrane Review on Rituximab for MG (2025); Network Meta-Analysis of Novel Biologics in gMG (2025)
This is a shared conversation. Sign in to Orris to start your own chat.