Crohn's disease
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"Crohn's disease"[MeSH Terms] AND management
Reading File
Reading File
Searching PubMed
"Crohn disease"[MeSH Terms] AND therapy
Reading File
Reading File
Finding Sources
Finding Sources
Searching Images
Crohn disease pathology histology endoscopy
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of Crohn's disease based on Sleisenger and Fordtran's Gastrointestinal and Liver Disease.
Crohn's Disease
Definition & Overview
Crohn's disease (CD) is a chronic, relapsing transmural inflammatory bowel disease that can affect any segment of the gastrointestinal tract from mouth to anus. It is characterized by skip lesions (discontinuous areas of involvement), transmural inflammation, non-caseating granulomas, and a tendency toward stricture and fistula formation.
Epidemiology
- CD and ulcerative colitis (UC) together constitute the two major forms of inflammatory bowel disease (IBD).
- Highest incidence is in North America, Northern Europe, and other Western countries.
- Bimodal age of onset: peaks in the 2nd–4th decades and a smaller peak in the 6th–7th decades.
- Slightly more common in women.
- Higher rates in Ashkenazi Jewish populations; urban > rural.
Pathogenesis
CD results from a dysregulated immune response to intestinal microbiota in genetically susceptible individuals, triggered by environmental factors.
Genetics
- Over 200 genetic loci are associated with IBD. The most important is NOD2 (also called CARD15) on chromosome 16 — variants are associated with stricturing or fistulizing phenotype and increased surgical risk.
- ASCA (anti-Saccharomyces cerevisiae antibody) correlates with small intestinal disease; anti-OmpC predicts internal perforations; anti-CBir1 (antiflagellin) is associated with penetrating/stricturing disease.
Immunology
- Th1-mediated response dominates (IL-12, TNF-α, IFN-γ). IL-23/Th17 axis also implicated.
- Breakdown of intestinal barrier → microbial translocation → uncontrolled innate and adaptive immune activation → chronic transmural inflammation.
- Proteases and matrix metalloproteinases drive tissue destruction, sinus tracts, and fistula formation.
Environmental Factors
- Smoking increases risk and worsens disease course (opposite of UC).
- Appendectomy, altered gut microbiome, Western diet, and prior enteric infections are implicated.
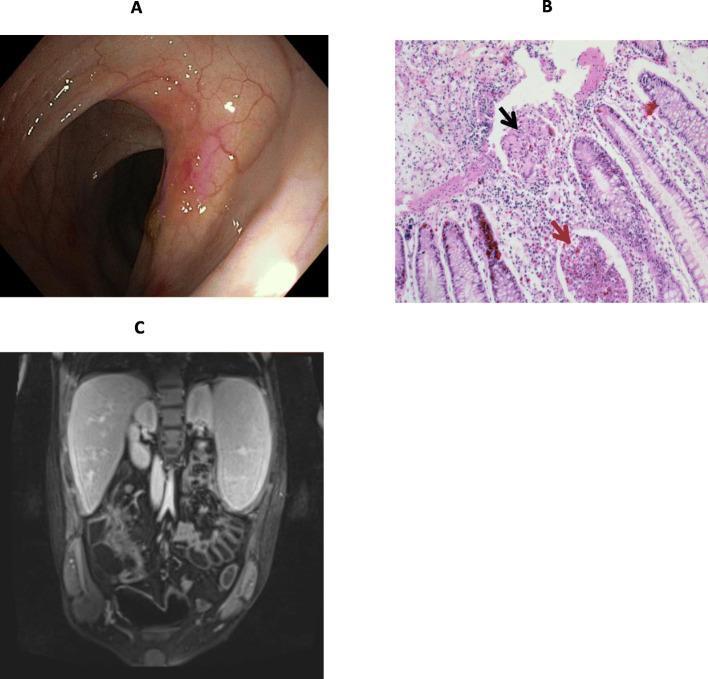
Pathology
| Feature | Description |
|---|---|
| Distribution | Any GI segment; most commonly terminal ileum ± cecum (~80%) |
| Skip lesions | Discontinuous inflammation with normal intervening mucosa |
| Transmural | Affects full bowel wall thickness |
| Cobblestone pattern | Mucosal islands surrounded by deep fissuring ulcers |
| Non-caseating granulomas | Pathognomonic but present in only ~50% of biopsies |
| Creeping fat | Mesenteric fat wrapping around bowel wall |
| String sign (radiology) | Marked luminal narrowing from spasm/edema — transiently resolves with glucagon |
Clinical Features
Typical Presentation by Location
Ileocecal (most common):
- Insidious onset of crampy RLQ pain, diarrhea (non-bloody or minimally bloody), weight loss
- RLQ mass or fullness on exam (matted bowel loops)
- Can mimic appendicitis
Colonic disease:
- Diarrhea ± blood (less profuse bleeding than UC)
- Tenesmus less prominent (rectum often spared)
- Abdominal pain more prominent than UC
- May present as fulminant colitis
Perianal disease:
- Occurs in ~24% before intestinal symptoms (mean lead time 4 years)
- Skin tags ("elephant ear" type 1 — soft, nontender; type 2 — edematous, hard)
- Eccentric anal fissures, ulcers, perianal fistulas, abscesses
Upper GI (uncommon in isolation):
- Gastroduodenal CD: "bamboo-joint" gastric folds, H. pylori-negative PUD, epigastric pain
- Esophageal: dysphagia, odynophagia (<2% of patients)
- Proximal jejunal: younger at diagnosis, more extensive resection required
Systemic/Extraintestinal Manifestations
- Musculoskeletal: peripheral arthritis, axial arthropathy (ankylosing spondylitis, sacroiliitis)
- Ocular: episcleritis, uveitis
- Dermatologic: erythema nodosum, pyoderma gangrenosum
- Hepatobiliary: primary sclerosing cholangitis (less common than in UC), fatty liver, cholelithiasis
- Metabolic: vitamin B12/fat-soluble vitamin deficiencies (terminal ileal disease/resection), osteoporosis
Disease Classification
The Montreal Classification categorizes CD by:
- Age at diagnosis: A1 (≤16 yrs), A2 (17–40 yrs), A3 (>40 yrs)
- Location: L1 ileal, L2 colonic, L3 ileocolonic (± L4 upper tract modifier)
- Behavior: B1 inflammatory, B2 stricturing, B3 penetrating (± p perianal modifier)
Disease behavior categories:
- Inflammatory (B1): active inflammation, no fibrosis or fistula
- Stricturing (B2): fibrotic stenosis → obstructive symptoms
- Penetrating/Fistulizing (B3): transmural penetration to adjacent structures
Diagnosis
Endoscopy (ileocolonoscopy + biopsy) is the gold standard.
- Findings: aphthous ulcers → deep longitudinal/serpiginous ulcers → cobblestone mucosa, skip lesions, strictures
Imaging:
- MR enterography (preferred): mural thickening, hyperenhancement, the comb sign (engorged peri-enteric vasculature), fistula/abscess detection — avoids radiation
- CT enterography: similar but radiation exposure
- Capsule endoscopy: evaluates small bowel mucosa (contraindicated if stricture suspected)
Biomarkers:
- CRP: elevated in active disease; correlates with endoscopic activity
- Fecal calprotectin: pooled sensitivity 88%, specificity 67% for CD vs. endoscopically active disease; useful for monitoring relapse and biologic response
- Fecal lactoferrin: also useful marker of intestinal inflammation
Activity scoring:
- CDAI (Crohn's Disease Activity Index): remission = CDAI <150; response = CDAI decrease ≥100 points
- Mucosal healing (endoscopic remission) is now the primary therapeutic target, as symptoms alone poorly correlate with objective disease activity
Treatment
Mild-to-Moderate Disease
- Budesonide 9 mg/day (oral, controlled ileal-release): first-line for ileocecal disease — superior to placebo and 5-ASA, ~15% less effective than prednisolone but far fewer systemic side effects (~90% first-pass hepatic metabolism)
- Aminosalicylates (5-ASA): minimal efficacy in CD (unlike UC)
- Antibiotics (metronidazole, ciprofloxacin): for perianal/fistulizing disease and septic complications; not for luminal disease maintenance
Moderate-to-Severe Disease
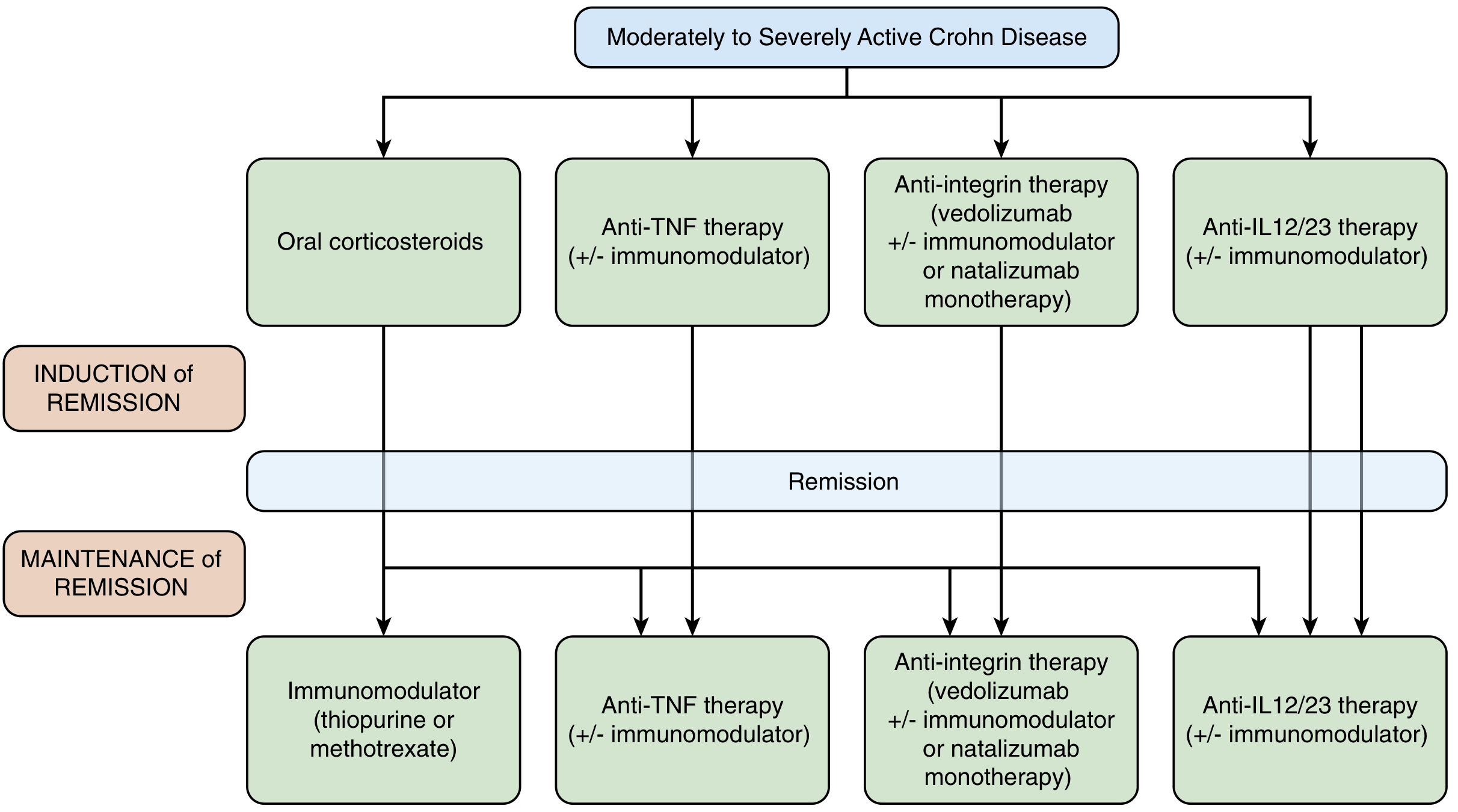
Glucocorticoids (induction only):
- Prednisone 40–60 mg/day tapering over 6–12 weeks; ~80% response at 1 month
- NOT effective for maintenance — no benefit at 6, 12, or 24 months in meta-analyses
- 20% are steroid-resistant; 45% relapse or cannot taper within 1 year (steroid-dependence)
Immunomodulators (maintenance):
- Azathioprine/6-mercaptopurine: effective for steroid-sparing and maintenance; onset 3–4 months; monitor for myelosuppression (check TPMT activity), hepatotoxicity, lymphoma risk
- Methotrexate: 25 mg IM weekly for induction, 15 mg IM for maintenance; alternative for thiopurine-intolerant patients; folate supplementation required
Biologics:
| Agent | Mechanism | Key Data |
|---|---|---|
| Infliximab (anti-TNF) | Chimeric anti-TNF-α IgG1 | ACCENT trial: 39–45% remission at 54 wks (vs. 21% placebo); ACCENT II: 36% fistula closure |
| Adalimumab (anti-TNF) | Fully human anti-TNF | Non-inferior to infliximab; SC administration |
| Certolizumab (anti-TNF) | PEGylated Fab' fragment | Modest benefit; preferred in pregnancy |
| Vedolizumab (anti-integrin) | Gut-selective α4β7 blocker | Safer infection profile; slower onset |
| Ustekinumab (anti-IL12/23) | Anti-p40 subunit | UNIFI/UNIFI-type trials; effective after anti-TNF failure |
| Risankizumab (anti-IL-23p19) | Selective IL-23 blocker | Recent meta-analysis (PMID 40071763, 2025): superior to ustekinumab in RCTs |
Combination therapy (biologic + immunomodulator): reduces immunogenicity and improves trough levels; SONIC trial showed superiority of infliximab + azathioprine over either monotherapy.
Complications
Fistulas & Abscesses
- Perianal fistulas: 15–35% of patients; simple (low-lying) vs. complex (multiple tracts, involve scrotum/labia/buttocks)
- Enteroenteric, enterovesical, enterocutaneous, rectovaginal fistulas from transmural penetration
- Intra-abdominal abscess: spiking fevers + focal tenderness; masked by steroids → maintain high suspicion; managed with percutaneous drainage + antibiotics, then elective resection
Stricture
- Long-standing transmural inflammation → fibrotic stenosis
- Distinguish from inflammatory stricture (responds to anti-inflammatory therapy) vs. fibrostenotic (requires endoscopic dilation or surgery)
- All strictures require biopsy to exclude malignancy
Malignancy
- Colorectal cancer: increased risk with colonic CD (similar to UC); surveillance colonoscopy recommended after 8–10 years of colonic disease
- Small bowel adenocarcinoma: rare but elevated relative risk
Small Bowel Obstruction (SBO)
- CD is the cause in ~5% of all SBOs
- Must distinguish: active inflammatory flare vs. fibrotic stricture vs. unrelated cause (adhesions, hernia, cancer)
- Up to 75% of CD patients require at least one abdominal surgery in their lifetime
Surgery
- Risk of surgery: 16% at 1 year, 33% at 5 years, 47% at 10 years after diagnosis (population-based data)
- Rates have declined significantly over recent decades with expanded biologic therapy
- Guiding principle: preserve intestinal length — wide margins do NOT reduce recurrence
- Most common operation: ileocecal resection with primary anastomosis (often laparoscopic)
- Strictureplasty: preferred over resection for scattered strictures to spare bowel
- Laparoscopic ileocecal resection vs. infliximab (LIR:C trial): equivalent QOL at 12 months in limited (<40 cm) ileal disease — surgery may be a primary alternative in selected patients
- After resection: recurrence at anastomosis in 20–50%; routine post-operative colonoscopy at 6–12 months + early re-introduction of immunomodulators/biologics reduces recurrence
Recent Evidence
Three recent systematic reviews are relevant:
- IL-23p19 antagonists vs. ustekinumab (PMID 40071763, Am J Gastroenterol 2025): meta-analysis of RCTs shows IL-23p19 antagonists (risankizumab, mirikizumab) outperform ustekinumab
- Perianal Crohn's disease (PMID 40315877, Lancet Gastroenterol Hepatol 2025): novel diagnostic criteria and management consensus for isolated perianal CD
- Persistence of advanced therapies (PMID 38651771, Aliment Pharmacol Ther 2024): meta-analysis on long-term drug persistence in IBD
Sources: Sleisenger and Fordtran's Gastrointestinal and Liver Disease (Chapters 115, 116, 123)
This is a shared conversation. Sign in to Orris to start your own chat.