For a medical student studying mbbs . Tell me all about anemia in pregnancy
Reading File
Finding Sources
Finding Sources
Searching PubMed
"anemia in pregnancy"[MeSH Terms] AND management
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Searching Images
iron deficiency anemia peripheral blood smear microcytic hypochromic
Searching PubMed
"iron deficiency anemia" AND pregnancy AND treatment
Loading Image
Loading Image
Here is a comprehensive, MBBS-level guide to Anemia in Pregnancy:
Anemia in Pregnancy — Complete MBBS Study Guide
1. Definition
Anemia = hemoglobin (Hb) value below the lower limit of normal, not explained by hydration status.
The normal Hb for adult females is 14.0 ± 2.0 g/dL. In pregnancy, due to hemodilution (plasma volume expands ~40–50%, red cell mass only ~15–25%), the CDC defines anemia in pregnancy as:
| Trimester | Hb threshold |
|---|---|
| First trimester | < 11.0 g/dL |
| Second trimester | < 10.5 g/dL |
| Third trimester | < 11.0 g/dL |
Globally, anemia affects ~38% of pregnant women; about half of these are due to iron deficiency. In the United States, the prevalence is ~17%, with a 4–7× higher incidence in Black women than White women.
2. Physiologic Anemia of Pregnancy
This is not true pathological anemia — it is a normal physiologic adaptation:
- Plasma volume expands 40–50% above baseline (peaks at weeks 16–24)
- Red cell mass expands only 15–25%
- Net result: dilutional decrease in Hb — normocytic, normochronic
Key point: A normocytic anemia with Hb > 11 g/dL (first/third trimester) or > 10 g/dL (second trimester) in an uncomplicated pregnancy can be attributed to physiologic anemia without further workup. Lower values or microcytic/macrocytic anemia require investigation.
3. Classification & Causes
By MCV:
| Type | MCV | Common Causes in Pregnancy |
|---|---|---|
| Microcytic (↓ MCV) | < 80 fL | Iron deficiency (most common), α-thalassemia, β-thalassemia |
| Normocytic (normal MCV) | 80–100 fL | Acute blood loss, anemia of chronic disease, aplastic anemia |
| Macrocytic (↑ MCV) | > 100 fL | Folate deficiency, B12 deficiency, megaloblastic anemia |
4. Iron Deficiency Anemia (IDA) — The Most Common
Why IDA is common in pregnancy:
- Fetal and placental iron needs: ~300 mg
- Expansion of maternal red cell mass: ~500 mg
- Basal losses: ~200 mg
- Total iron demand: ~1,000 mg over pregnancy
- Daily iron requirement rises from ~0.8 mg/day (non-pregnant) to 6–7 mg/day (third trimester)
Clinical Features:
- Symptoms: Fatigue, weakness, lightheadedness, exertional dyspnea, palpitations
- Signs: Pallor (conjunctiva, palms, mucous membranes), tachycardia, angular stomatitis, koilonychia (spoon nails), glossitis, brittle nails
- Pica (craving non-food items — ice, clay, starch) is pathognomonic
- Often discovered incidentally on routine CBC
Stages of Iron Deficiency:
- Iron depletion — Ferritin ↓, iron stores exhausted, no anemia yet
- Iron-deficient erythropoiesis — Serum iron ↓, TIBC ↑, transferrin saturation ↓, no anemia yet
- Iron deficiency anemia — Hb ↓, microcytic hypochromic RBCs on smear
Peripheral Blood Smear in IDA vs Normal:
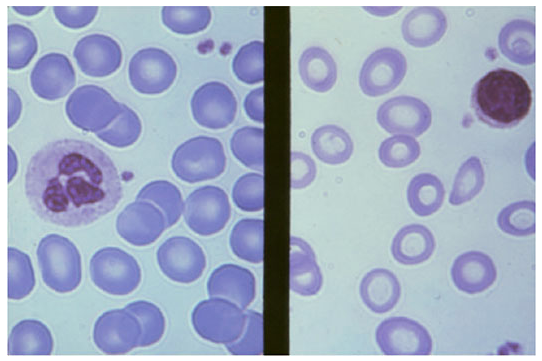
Lab Findings in IDA:
| Investigation | Iron Deficiency | Thalassemia | Anemia of Inflammation |
|---|---|---|---|
| Smear | Micro/hypo | Micro/hypo + target cells | Normal or mild micro/hypo |
| Serum iron | ↓ (<30 μg/dL) | Normal–high | ↓ (<50 μg/dL) |
| TIBC | ↑ (>360 μg/dL) | Normal | ↓ (<300 μg/dL) |
| Transferrin saturation | ↓ (<10%) | 30–80% | 10–20% |
| Serum ferritin | ↓ (<15 μg/L) | Normal–high | ↑ (30–200 μg/L) |
| Hb electrophoresis | Normal | Abnormal (β-thal) | Normal |
Serum ferritin is the single most accurate lab value for diagnosing IDA in pregnancy. — Rosen's Emergency Medicine
Treatment of IDA:
Oral Iron (first-line):
- Ferrous sulfate 325 mg (60 mg elemental iron) — one tablet once or twice daily
- Take on empty stomach for best absorption; vitamin C enhances absorption
- Side effects: nausea, constipation, dark stools — take with food if needed
- Hemoglobin should rise ~1 g/dL per week with adequate therapy
- Continue therapy for 3 months postpartum to replete stores
Intravenous Iron (when oral fails or is not tolerated):
- Indications: intolerance to oral iron, non-compliance, malabsorption, severe or late anemia
- Agents: ferric carboxymaltose, iron sucrose, low molecular weight iron dextran
- IV iron replenishes stores faster and more effectively than oral iron
- A 2024 JAMA systematic review for the USPSTF confirmed iron supplementation reduces IDA in pregnancy but ongoing research examines optimal dosing strategies (PMID: 39163033)
Recombinant erythropoietin: Reserved for refractory cases; a 2025 systematic review (PMID: 39087437) found limited evidence for its routine use in pregnancy.
5. Folate Deficiency Anemia (Megaloblastic)
Why common in pregnancy:
- Folate requirements nearly double during pregnancy (from 400 μg to 600–800 μg/day)
- Increased cell proliferation demands more folate for DNA synthesis
- Poor dietary intake, multiple pregnancy, hemolytic states all increase risk
Clinical Features:
- Megaloblastic anemia: macrocytic (MCV > 100), hypersegmented neutrophils
- Glossitis, angular stomatitis, mild jaundice
- No neurological deficits (unlike B12 deficiency)
- Increased risk of neural tube defects in the fetus if deficiency is in early pregnancy
Peripheral Smear in Megaloblastic Anemia:
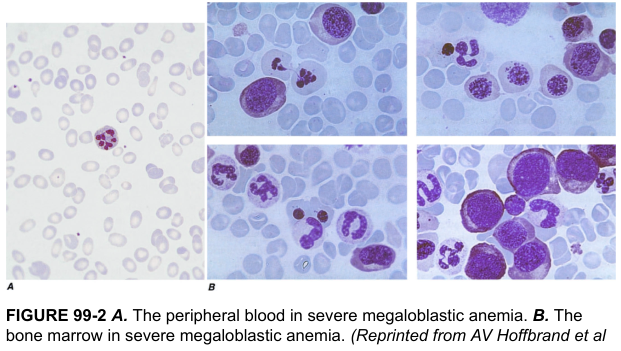
Lab Findings:
- Hb ↓, MCV ↑ (>100 fL), MCHC normal
- Hypersegmented neutrophils (>5 lobes in >5% of neutrophils)
- Serum folate ↓, RBC folate ↓ (more reliable)
- LDH ↑, indirect bilirubin ↑ (ineffective erythropoiesis)
- Megaloblasts in bone marrow
Treatment:
- Folic acid 5 mg/day orally until recovery, then maintenance
- Prevention (all pregnancies): Folic acid 0.4–0.5 mg/day from at least 4 weeks before conception to 12 weeks gestation → reduces neural tube defect risk by ~70%
- High-risk women (prior NTD, anticonvulsants): 4–5 mg/day
6. Vitamin B12 Deficiency
- Less common than folate deficiency in pregnancy
- Causes: strict vegetarianism/veganism, pernicious anemia (autoimmune), post-gastric surgery
- Macrocytic anemia + subacute combined degeneration of spinal cord (posterior and lateral column demyelination — neurological feature that distinguishes B12 from folate deficiency)
- Treatment: Hydroxocobalamin or cyanocobalamin IM injections
7. Sickle Cell Anemia in Pregnancy
- HbSS carries the highest risk — maternal mortality significantly elevated
- Complications:
- Increased vaso-occlusive crises (due to hyperviscosity, dehydration, infection)
- Preeclampsia, placental abruption
- Preterm labor, fetal growth restriction, stillbirth
- Acute chest syndrome
- Management:
- Prophylactic folic acid (5 mg/day — higher doses due to hemolysis)
- Hydration, analgesia for crises
- Avoid hydroxyurea in pregnancy (teratogenic)
- Exchange transfusion for severe complications (acute chest, stroke)
- Serial ultrasound for fetal growth
- Genetic counseling — partner screening for HbS trait
8. Thalassemia in Pregnancy
α-Thalassemia:
| Genotype | Genes deleted | Clinical status |
|---|---|---|
| Silent carrier | 1 gene | Normal, undetectable |
| α-Thal trait (minor) | 2 genes | Mild microcytic anemia, no symptoms |
| HbH disease | 3 genes | Moderate hemolytic anemia |
| Hb Bart's (hydrops fetalis) | 4 genes | Incompatible with life; intrauterine or neonatal death |
- α-Thal trait: mild microcytic anemia → must distinguish from IDA (normal ferritin, no response to iron)
- If both partners carry α-thal trait in cis (--/αα) conformation → 25% risk of Hb Bart's → offer prenatal diagnosis
β-Thalassemia:
- β-Thal minor (trait): Mild anemia, microcytic; elevated HbA2 >3.5% on electrophoresis; well tolerated in pregnancy; folic acid supplementation
- β-Thal major (Cooley's anemia): Rarely pregnant without transfusion support; managed with regular transfusions, chelation (avoid deferoxamine in first trimester), and careful monitoring
- β-Thal intermedia: Variable; may worsen in pregnancy; manage as per severity
9. Aplastic Anemia in Pregnancy
- Rare but life-threatening
- Pancytopenia: anemia + neutropenia + thrombocytopenia
- Most serious complications: hemorrhage and sepsis — leading causes of maternal death in aplastic anemia
- Bone marrow biopsy: hypocellular marrow
- Management:
- Supportive transfusions (packed RBCs, platelets)
- Immunosuppression (antithymocyte globulin, cyclosporine)
- Bone marrow transplantation ideally deferred until after delivery
- High-dose corticosteroids considered in some cases
10. Anemia of Chronic Disease / Infection
- Normocytic, normochromic anemia
- Associated with chronic infections (HIV, TB, pyelonephritis), chronic renal disease, chronic liver disease, autoimmune conditions
- Pathophysiology: ↑ hepcidin → ↓ iron release from macrophages → functional iron deficiency
- Distinguish from IDA: ferritin is normal or elevated in ACD
- HIV-associated moderate–severe anemia in pregnancy → workup for tuberculosis (per Rosen's)
- Treatment: treat underlying condition; iron supplementation only if concurrent IDA confirmed
11. Maternal and Fetal Consequences of Anemia
Maternal Effects:
- Fatigue, impaired work capacity
- Cardiac decompensation (high-output heart failure in severe anemia)
- Increased susceptibility to infection
- Postpartum hemorrhage poorly tolerated
- Peripartum cardiomyopathy risk
- Increased maternal mortality (severe anemia, Hb < 6 g/dL)
Fetal/Neonatal Effects:
- Fetal growth restriction (FGR)
- Preterm birth
- Low birth weight
- Neonatal anemia
- Increased perinatal morbidity and mortality
- Neural tube defects (folate deficiency in first trimester)
12. Screening and Routine Evaluation
- CBC at booking (first antenatal visit) and again at 28–32 weeks
- WHO and most national guidelines recommend screening all pregnant women
- Additional tests based on CBC morphology (see Table below)
Evaluation Algorithm:
CBC with differential + reticulocyte count
↓
MCV < 80 (Microcytic) MCV 80-100 (Normocytic) MCV > 100 (Macrocytic)
↓ ↓ ↓
Serum ferritin, TIBC, Reticulocyte count Serum folate, B12,
serum iron, Hb electrophoresis ± bone marrow LDH, PBS
↓
Ferritin ↓ → IDA
Ferritin normal + micro → Thalassemia (electrophoresis)
Ferritin ↑ → ACD
13. Prevention
| Intervention | Details |
|---|---|
| Iron supplementation | Universal supplementation in high-prevalence areas; selective in low-prevalence settings |
| Folic acid supplementation | 0.4–0.5 mg/day starting pre-conception; 4–5 mg/day in high-risk women |
| Dietary advice | Iron-rich foods (meat, legumes, green leafy vegetables), vitamin C-rich foods to enhance iron absorption |
| Deworming | In endemic areas — helminth infections cause blood loss and impair iron absorption |
| Malaria prophylaxis | In endemic areas — malaria is a major cause of anemia in pregnancy |
14. High-Yield Summary for Exams
| Feature | IDA | Folate deficiency | B12 deficiency | Thalassemia trait |
|---|---|---|---|---|
| MCV | ↓ | ↑ | ↑ | ↓ |
| Ferritin | ↓ | Normal | Normal | Normal/↑ |
| TIBC | ↑ | Normal | Normal | Normal |
| Smear | Micro, hypochromic | Macrocytic, hyperseg neutrophils | Macrocytic, hyperseg neutrophils | Micro, hypochromic + target cells |
| Hb electrophoresis | Normal | Normal | Normal | Abnormal (β-thal) / normal (α-thal) |
| Neuro signs | No | No | Yes (SACD) | No |
| Treatment | Ferrous sulfate / IV iron | Folic acid 5 mg | Vit B12 IM | Folic acid; genetic counseling |
Key Sources
- Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice, Chapter 55 (Anemia in Pregnancy), pp. 1329–1344
- Goldman-Cecil Medicine, Section on Physiologic Anemia of Pregnancy, p. 1676
- Harrison's Principles of Internal Medicine, 21st ed., pp. 1721, 2889
- Recent USPSTF systematic review on iron supplementation in pregnancy: JAMA 2024 (PMID 39163033)
This is a shared conversation. Sign in to Orris to start your own chat.