Prevention of migraine treatment for 21 y old female
Reading File
Finding Sources
Searching PubMed
"migraine" AND "preventive treatment" AND "young women"
Searching the Web
migraine prevention treatment guidelines 2024 young women first line
Finding Sources
Searching PubMed
"migraine" AND "preventive treatment"
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive information from the textbooks and recent guidelines. Let me compile a thorough answer.
Migraine Prevention (Prophylaxis) in a 21-Year-Old Female
When to Start Preventive Treatment
Prophylactic treatment is indicated when:
- Attacks occur ≥2–4 times per month
- Headaches are severe, prolonged, or disabling
- Acute therapies are ineffective, contraindicated, or overused
- Significant impact on quality of life or functioning
(Bradley & Daroff's Neurology; Lippincott Pharmacology)
Key Considerations Specific to Young Women
Hormonal Triggers
Migraine is 3× more common in women after menarche — approximately 25% of women have migraine during reproductive years. Key hormonal interactions:
- Menstrual migraine occurs in up to 60% of female migraineurs (menstrually related) and ~7% have pure menstrual migraine (attacks days −2 to +3 of cycle)
- The trigger is estrogen withdrawal before menstruation, which modulates serotonin, dopamine, and opioid receptor systems
- Oral contraceptives (COCs) can worsen migraine in some women and are contraindicated in migraine with aura due to increased stroke risk
Valproate Caution
Valproate/divalproex sodium is contraindicated in women of childbearing potential due to teratogenicity (neural tube defects). This is a critical prescribing consideration at age 21.
Topiramate Caution
Also teratogenic — requires effective contraception and careful counseling.
Preventive Drug Options
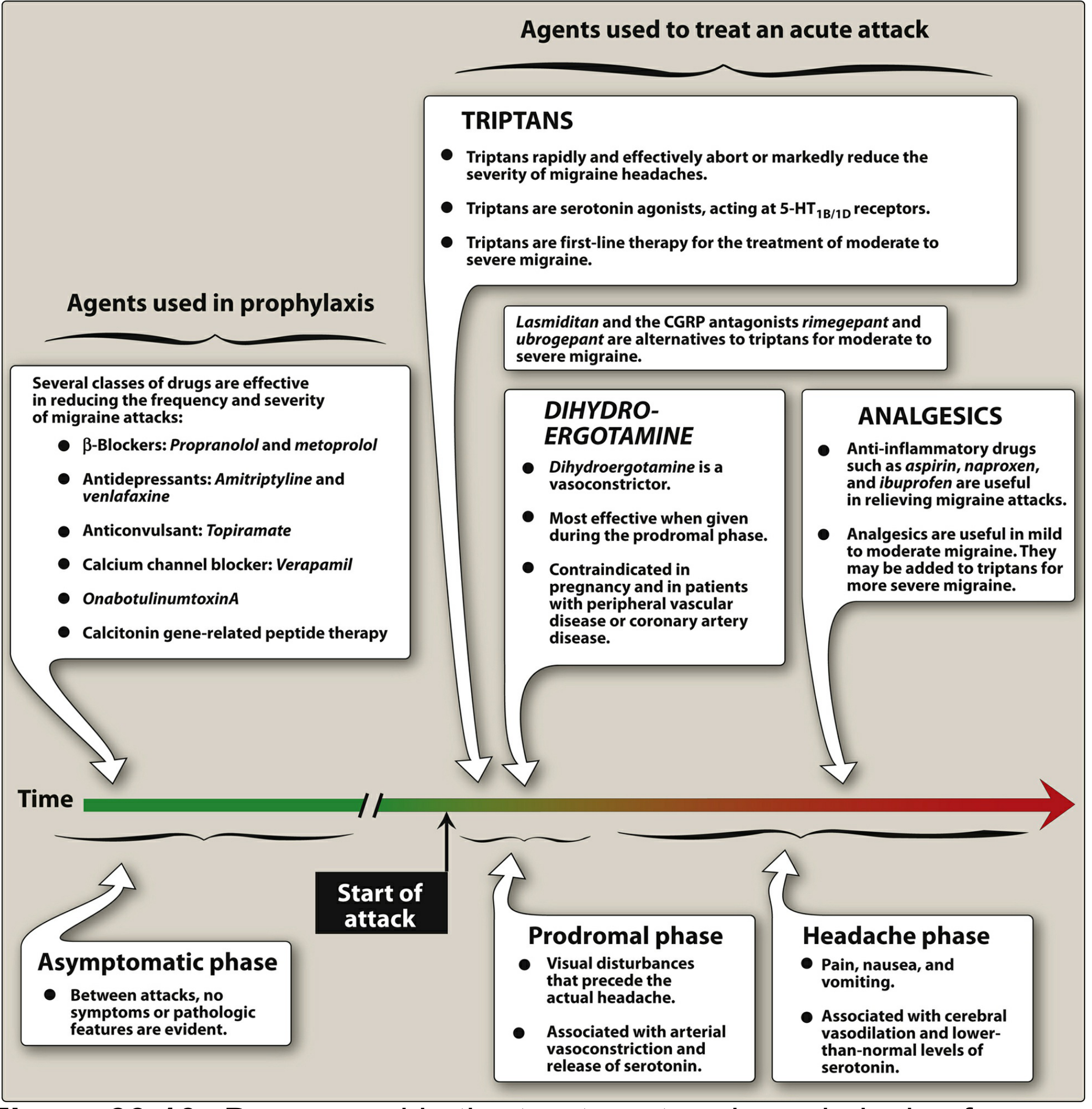
First-Line Agents (Established Efficacy)
| Drug Class | Agents | Dose | Notes |
|---|---|---|---|
| β-Blockers | Propranolol, Metoprolol, Timolol | Propranolol 40–240 mg/day | Drugs of choice; avoid in asthma, depression |
| Anticonvulsants | Topiramate | 75–200 mg/day (titrate slowly) | Weight loss benefit; teratogenic — contraception required; cognitive side effects |
| Anticonvulsants | Divalproex sodium | 500–1750 mg/day | Effective but contraindicated in women who may become pregnant |
Second-Line Agents (Probable Efficacy)
| Drug Class | Agents | Notes |
|---|---|---|
| Antidepressants | Amitriptyline, Venlafaxine | Especially useful with comorbid depression/anxiety; avoid agents causing fatigue/depression |
| Calcium channel blockers | Verapamil | Used particularly for basilar-type migraine |
| NSAIDs | Naproxen sodium | Especially useful for menstrual migraine prophylaxis (perimenstrual use); reduces risk of chronic migraine |
CGRP-Targeting Therapies (Now First-Line per AHS 2024)
The American Headache Society 2024 consensus statement now positions CGRP-targeting therapies as first-line preventive options, alongside traditional agents:
| Type | Agents | Route |
|---|---|---|
| Monoclonal antibodies | Erenumab, Galcanezumab, Fremanezumab, Eptinezumab | Monthly/quarterly injection |
| Oral gepants | Atogepant, Rimegepant | Daily oral tablet |
These are migraine-specific, have a favorable side-effect profile, and are especially valuable in patients who have failed traditional therapies. They carry no teratogenicity concern in the same way as valproate/topiramate, though data in pregnancy remains limited.
Menstrual Migraine — Special Approach for Young Women
Perimenstrual (cyclic) prophylaxis options (for predictable cycles):
- Naproxen sodium 550 mg twice daily from day −2 to day +3
- Frovatriptan 2.5 mg twice daily (perimenstrual) — has longest half-life among triptans
- Estrogen supplementation (transdermal estradiol patch 0.1 mg) perimenstrually may prevent estrogen-withdrawal trigger
For continuous (non-cyclic) migraine throughout the month, standard continuous prophylaxis is preferred.
Non-Pharmacologic Preventive Strategies
These should always accompany medications:
- Trigger identification & avoidance: Keep a headache diary (alcohol, caffeine withdrawal, stress, irregular sleep, skipped meals, strong scents, dietary triggers like nitrates/tyramine-rich foods)
- Regular sleep schedule and consistent wake times
- Regular aerobic exercise
- Stress management / biofeedback / relaxation therapy — evidence-supported
- Riboflavin (Vitamin B2): 400 mg/day — low side-effect profile, RCT evidence for modest reduction in attack frequency
- Magnesium: 600 mg/day (chelated or slow-release) — mixed evidence but well tolerated; especially relevant in menstrual migraine
- Cognitive Behavioral Therapy (CBT)
Practical Prescribing Summary for a 21-Year-Old Female
| Priority | Agent | Key Reason |
|---|---|---|
| First choice | Propranolol or Metoprolol | Proven, safe, no teratogenicity issue |
| With comorbid anxiety/depression | Amitriptyline or Venlafaxine | Dual benefit |
| For menstrual-predominant | Naproxen sodium perimenstrually or Frovatriptan mini-prophylaxis | Targeted and simple |
| CGRP option | Atogepant (oral) or injectable mAb | Excellent tolerability, now first-line per AHS 2024 |
| Avoid | Valproate, Topiramate (without reliable contraception) | Teratogenic risk |
| Avoid | Combined oral contraceptives in migraine with aura | Stroke risk |
Recent Evidence
- Ornello et al. 2025 (Cephalalgia) — Evidence-based pharmacological treatment guidelines [PMID: 40277319] (Systematic Review/Practice Guideline)
- Khoo et al. 2024 (J Headache Pain) — Meta-analysis of menstrual migraine treatment [PMID: 39227797]
- AHS 2024 consensus: CGRP-targeting therapies elevated to first-line preventive status
Sources: Bradley & Daroff's Neurology in Clinical Practice; Lippincott Illustrated Reviews Pharmacology; Textbook of Family Medicine 9e; Kaplan & Sadock's Comprehensive Textbook of Psychiatry; AHS 2024 Consensus Statement
This is a shared conversation. Sign in to Orris to start your own chat.