Normal anatomy of pancreatic ducts
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Finding Sources
Loading Image
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive information from multiple textbooks. Let me compile the full answer.
Normal Anatomy of Pancreatic Ducts
Embryological Basis
The pancreatic duct system can only be fully understood through its embryology. The pancreas develops from two buds arising from the foregut:
- Ventral bud - smaller, arises from the hepatic diverticulum; its duct (the duct of Wirsung) connects directly to the common bile duct.
- Dorsal bud - larger, arises from the duodenum; its duct (the duct of Santorini) drains directly into the duodenum.
With gut rotation, the ventral anlage rotates clockwise and posteriorly around the duodenum to fuse with the dorsal bud. The ventral anlage becomes the inferior pancreatic head and uncinate process, while the dorsal anlage becomes the body and tail. The two ducts fuse in the pancreatic head in most individuals.
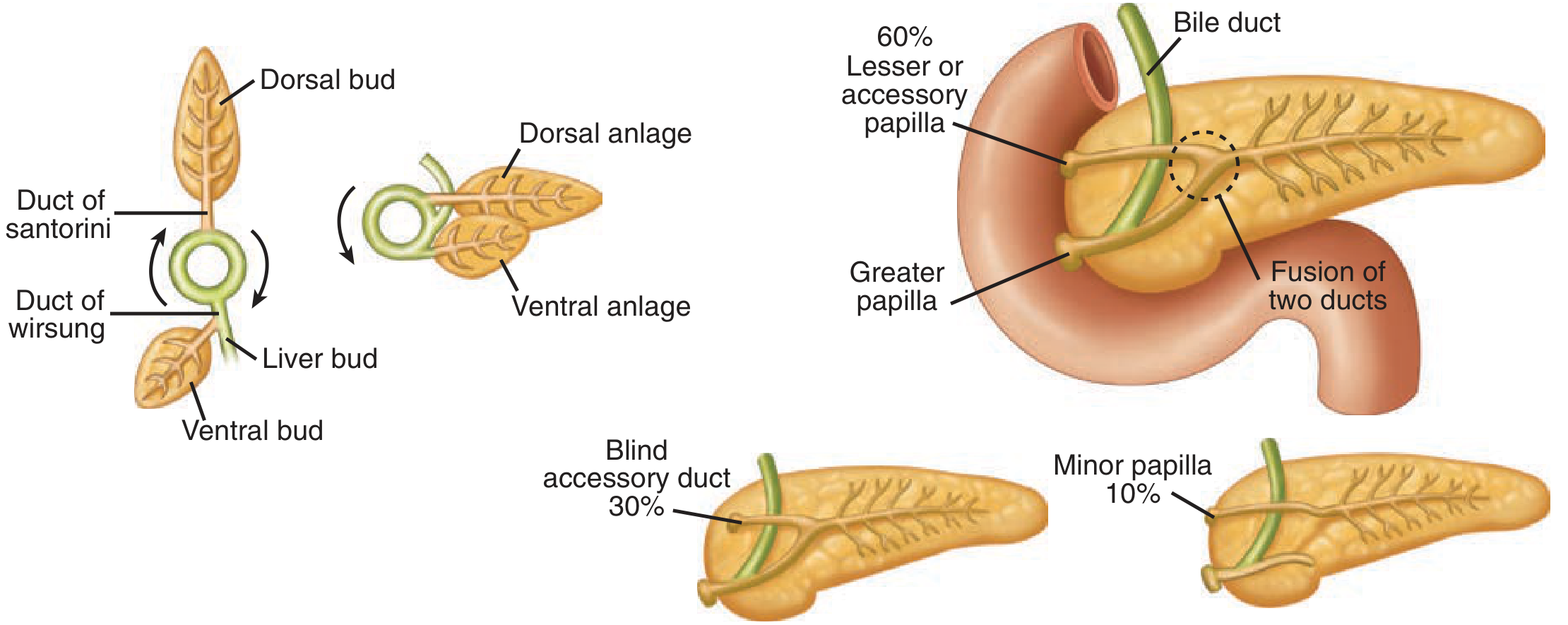
Figure: Embryology of pancreas and duct variations - Schwartz's Principles of Surgery, 11th ed.
The Main Pancreatic Duct (Duct of Wirsung)
The main pancreatic duct (MPD) runs from the tail of the pancreas to the major duodenal papilla (ampulla of Vater). Key features:
| Feature | Detail |
|---|---|
| Course | Extends from tail to head, running midway between superior and inferior borders, closer to the posterior surface |
| Diameter | 2-4 mm; tapers from 4 mm (head) to 2 mm (tail) |
| Length | Runs the full length of the gland |
| Pressure | ~twice that of the common bile duct, preventing bile reflux into the duct |
| Termination | Joins the common bile duct, empties at the ampulla of Vater (major papilla) on the medial aspect of the 2nd part of the duodenum |
The main duct runs close and nearly parallel to the distal common bile duct for 2-3 mm before they combine into a common channel.
- Schwartz's Principles of Surgery, 11th ed.
- Yamada's Textbook of Gastroenterology, 7th ed.
The Accessory Pancreatic Duct (Duct of Santorini)
The duct of Santorini is present in 40-70% of people and usually communicates with the main duct. It:
- Passes transversely to the right in the upper part of the pancreatic head
- Lies anterior to the intrapancreatic common bile duct
- Usually opens at the minor (lesser) papilla approximately 2 cm proximal to the ampulla of Vater
Common Channel at the Ampulla
The junction between the pancreatic and common bile ducts at the ampulla of Vater is variable:
- In ~1/3 of patients, the bile duct and pancreatic duct remain distinct to the end of the papilla
- In ~1/3, the ducts merge at the end of the papilla
- In ~1/3, a true common channel exists for several millimeters
The ampulla can measure up to 1 cm on imaging and projects into the duodenal lumen with enhancement similar to adjacent duodenal wall.
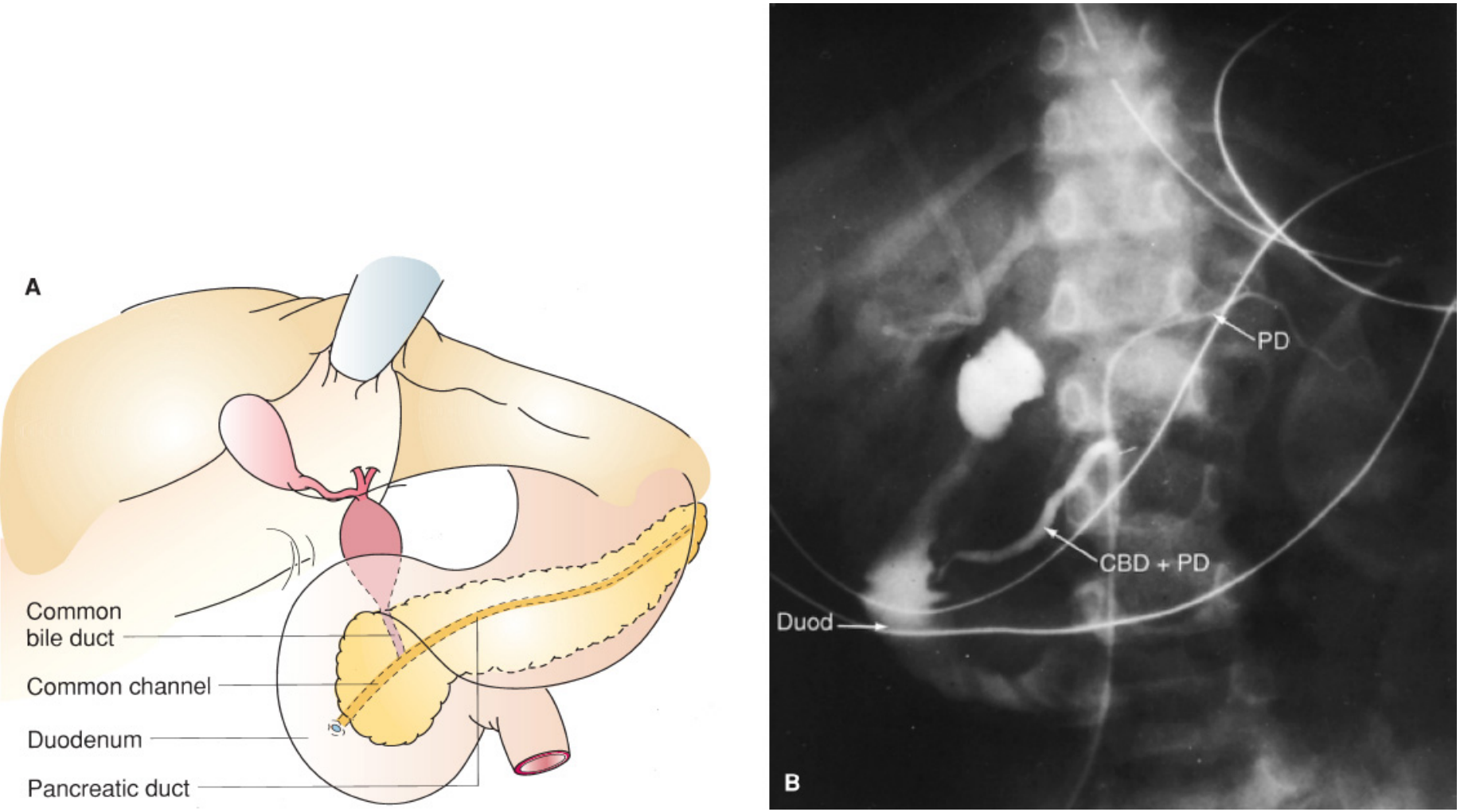
Figure: Anatomy of the duodenum, common bile duct and pancreatic duct (diagram + ERCP) - Mulholland & Greenfield's Surgery, 7th ed.
Sphincter of Oddi
The sphincter of Oddi is circular smooth muscle surrounding the common channel at the ampulla. It has three functional components:
- Choledochal sphincter - surrounds the common bile duct just distal to its entry through the duodenal wall
- Pancreatic duct sphincter - a short ring of circular smooth muscle surrounding the main pancreatic duct just before its termination
- Ampullary sphincter - surrounds the common channel itself
Contraction and relaxation are regulated by complex neural (CCK, secretin) and hormonal factors, controlling the flow of pancreatic and biliary secretions into the duodenum.
- Yamada's Textbook of Gastroenterology, 7th ed.
Histological Organization of the Duct System
The ductal hierarchy, from smallest to largest:
- Centroacinar cells - unique to the pancreas; pale-staining cells that line the acinar lumen and begin the duct system
- Intralobular (intercalated) ducts - drain individual acini
- Interlobular ducts - drain lobules; lined by columnar cells, goblet cells, and occasional argentaffin cells
- Main pancreatic duct - surrounded by thick connective tissue and elastic fibers
By weight, the glandular constituents are: 80% exocrine tissue, 18% ductular system, 2% endocrine tissue.
- Yamada's Textbook of Gastroenterology, 7th ed.
Normal Anatomical Variations (Prevalence)
Based on postmortem preparations, the "typical" ductal anatomy is actually present in as few as 33% of people:
| Variant | Prevalence |
|---|---|
| Patent accessory duct draining into minor papilla | ~33% |
| Absent/non-patent accessory duct | ~48% |
| Blind accessory duct (ends in duodenal wall, no opening) | ~8-30% |
| Independent openings of CBD and MPD | ~6% |
| Long common channel (5-15 mm) | ~6% |
| Absent main duct | ~5% |
| Pancreas divisum (ducts fail to fuse, 90% of pancreas drains via Santorini) | ~2-10% |
| Double accessory duct | ~1% |
Pancreas divisum is the most clinically important variant - it occurs in ~10% of patients and results from failure of the ducts of Wirsung and Santorini to fuse. Most of the pancreas then drains through the duct of Santorini and the lesser papilla, while only the inferior head and uncinate drain via the major papilla.
- Schwartz's Principles of Surgery, 11th ed.; Yamada's Textbook of Gastroenterology, 7th ed.
Summary Diagram
| Structure | Origin | Drains Into | Papilla |
|---|---|---|---|
| Duct of Wirsung (main PD) | Ventral anlage | Common channel with CBD | Major papilla (ampulla of Vater), 2nd part duodenum |
| Duct of Santorini (accessory PD) | Dorsal anlage | Directly into duodenum (when patent) | Minor papilla, 2 cm proximal to major |
This is a shared conversation. Sign in to Orris to start your own chat.